Article Text

Abstract
Introduction Significant progress has been made in the diagnosis and management of congenital anomalies (CA). In our study, we aimed to evaluate prenatal diagnosis, trend of surgical CA, mortality rate and the factors affecting their prognosis in our country.
Methods We enrolled in our study all children with CA who underwent surgery from January 2008 to December 2017. We compared prenatal diagnosis, incidence and mortality for two 5-year periods: the first period in 2008–2012 and the second period in 2013–2017.
Results During the study period, a total of 321 cases with CA were presented, with an incidence of 0.69–1.18 per 1000 live births. Intestinal, anal and esophageal atresia remain the most important CAs (23%, 18% and 16%), followed by diaphragmatic hernia and gastroschisis (10% and 7%). Comparing the incidence for the two periods, we did not find statistical differences (p=0.73), but the mortality rate has been reduced from 31.4% during the first period to 24.6% during the second period (p=0.17). Prenatal diagnosis has increased: 28% in the second period compared with 10% in the first period (p<0.001), without significantly affecting the prognosis (p=0.09). Birth of premature babies resulted in a significantly negative predictive factor for the prognosis of these anomalies (p=0.0002).
Conclusion Incidence of CA has not changed over the years in our country. Advances in intensive care, surgical techniques and parenteral nutrition made in recent years have significantly increased the survival of neonates born with surgical CA. Birth of premature babies was a significantly negative predictive factor for the prognosis of these anomalies.
- congenital anomalies
- incidence
- prenatal diagnosis
- outcome
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Congenital anomalies affect 1 in 33 newborns, resulting in about 3.2 million people with disabilities each year.1 Despite the advances made in both the diagnosis and treatment, mortality from congenital anomalies remains significant, one of the most important causes of perinatal deaths.2–5 According to WHO’s 63rd Health Assembly report, 303 000 newborns die within 4 weeks of life worldwide due to congenital anomalies.3 6 They are not just an important cause of death, but they also result in long-term disabilities, with significant effect on individuals, families, the health system and the society.2 Significant breakthroughs have been made in the last 50 years in the diagnosis and management of congenital abnormalities.7 8 The truly complex abnormalities are now treated with success of up to 90%.7 Establishing prenatal diagnosis has made it possible for births of children with congenital problems requiring surgical intervention to be carried out in specialized centers that have neonatal surgical management. Improving the accessibility and quality of pediatric surgical care in low-income and lower-middle-income countries has the potential to substantially reduce mortality and long-term disability.7 8 In various studies there is a question about these data for low-income and middle-income countries, sparse including on the incidence.7 Through our paper we would like to present some data about congenital anomalies in our country, prenatal diagnosis, trend of surgical congenital anomalies, mortality rate and the factors affecting their prognosis.
Methods
This is a 10-year retrospective study from January 1, 2008 to December 31, 2017. All children who underwent surgery for congenital surgical anomalies at University Hospital Center “Mother Teresa,” Tirana, are included. Children with congenital cardiac and neurological disorders have been excluded from the study. Data on the number of live births in Albania are obtained from the National Register of the Institute of Statistics. Determination of the incidence was made possible by the fact that the infantile surgery of our hospital is the only center in Albania that performs surgical interventions for newborn babies. We evaluated the trend of incidence for each anomaly during the last 10 years. We compared prenatal diagnosis, incidence and mortality rate for two 5-year periods: the first period in 2008–2012 and the second period in 2013–2017.
Results
During the study period, a total of 321 cases of congenital anomalies have underwent surgery, with an incidence of 0.69–1.18 per 1000 live births (table 1). Comparing the incidence for the two periods, we did not find statistical differences (p=0.73, 95% CI −0.1138 to 0.1548), but the mortality rate has been reduced from 31.4% during the first period to 24.6% during the second period (p=0.17, OR=0.71, 95% CI 0.4381 to 1.1661).
Incidence of surgical congenital anomalies during the study period
Assessing the type of pathology, it was noted that the largest number of congenital anomalies was recorded for intestinal atresia with 73 cases (23% of cases), anal atresia with 57 cases (18%) and esophageal atresia with 16% of cases, followed by diaphragmatic hernia in 10% of cases and gastroschisis in 7% of cases, and fewer cases with Hirschsprung disease, hypertrophic pyloric stenosis, mesenterium commune and so on.
We have evaluated each anomaly for both incidence and prognosis, and if there were significant changes between the two periods.
The incidence of intestinal atresia ranged from 0.09 to 0.32 per 1000 live births (table 2). There seems to be a slight reduction in the number of cases during the second period, but without a statistically significant difference between the two periods (p=0.71). Assessing the mortality of cases with intestinal atresia, we noticed that we have an important reduction in mortality in the second period (18% in the second period compared with 30% in the first period).
Incidence of intestinal atresia, anal atresia, esophageal atresia, diaphragmatic hernia and gastroschisis during a 10-year period
Incidence of anal atresia varied from 0.03 to 0.25 cases for 1000 live births, with 93% survival during the first period and 100% survival during the second period.
Esophageal atresia has an incidence ranging from 0.06 to 0.23 cases per 1000 live births, but without a statistically significant difference between the two periods (p=0.67). The mortality rate for esophageal atresia remains high in both periods, but to underline is the fact that during the last year we had 100% survival. The incidence ranges from 0.06 to 0.15 per 1000 live births for diaphragmatic hernia, without statistically significant differences between the two periods. There remains concern with regard to the very high mortality in both periods of up to 50%–66% of cases.
The incidence of gastroschisis ranges from 0.03 to 0.09 per 1000 live births. There is no statistically significant difference in incidence, but what was noticeable is an important reduction in mortality from 40% to 27% during the second period.
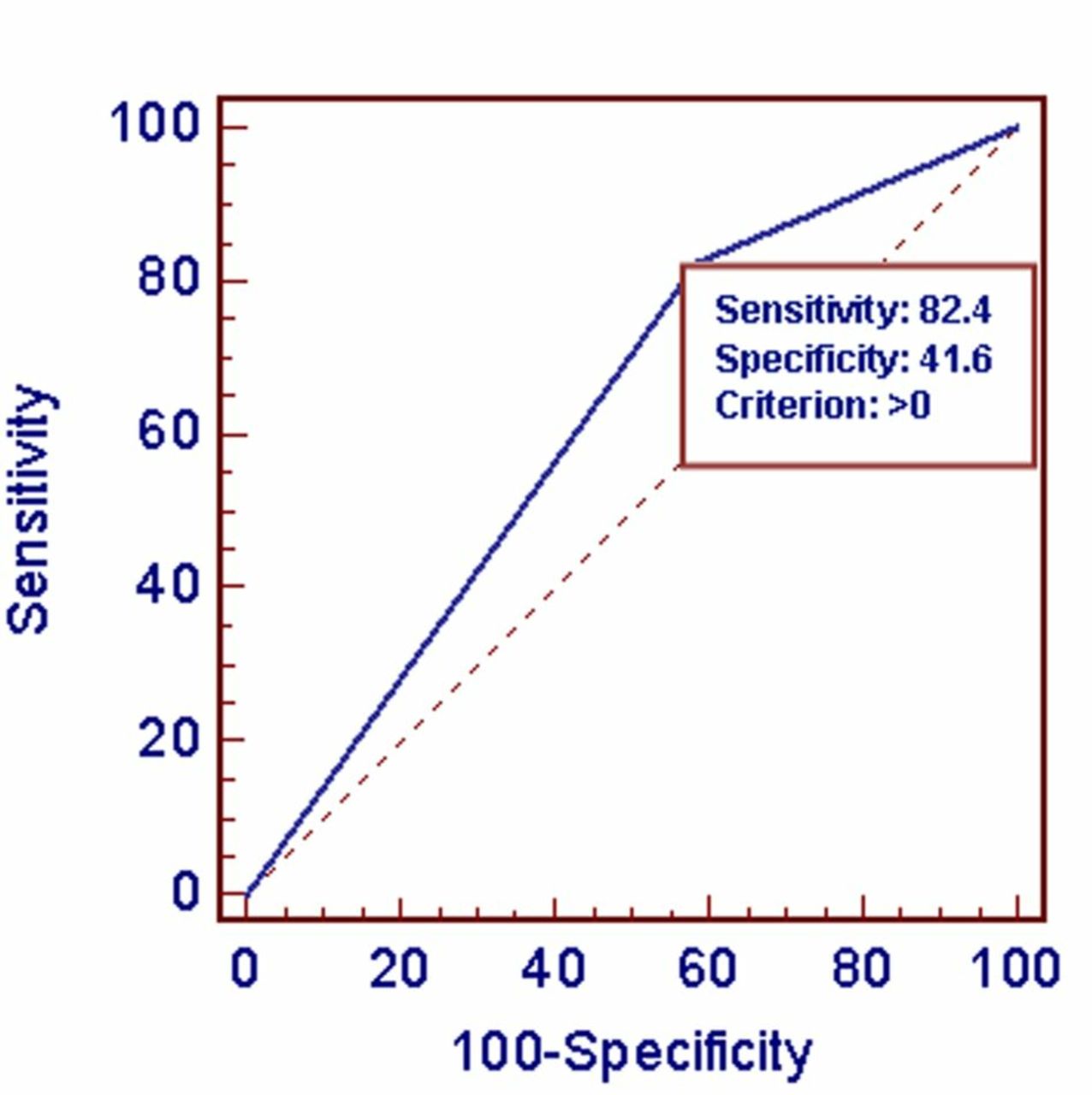
One important element we wanted to evaluate in our study was prenatal diagnosis. What was noticeable was the very low prenatal diagnosis with 19% of cases (61 cases). However, it is worth noting the very good diagnostic level by neonatologists, as in 52.3% of cases (168 cases) the diagnosis was suspected on the first day of delivery, thus positively influencing the time of surgical intervention. Only in 28.6% of cases (92 cases) the diagnosis was made after the first day, with an average of diagnosis of 3.35±8.2 days. The time of diagnosis may have influenced significantly by the fact that the largest part of anomalies comes from rural zones (61.1%, 196 cases). Only in 38.9% of cases (125 cases) was birth made in the capital. Prenatal diagnosis has increased significantly to 28% in 2013–2017 compared with 2008–2012 when it was about 10% (p<0.001). Considering the importance of prenatal diagnosis, we evaluated its impact on mortality as a predictive positive factor for the prognosis of these anomalies. On receiver operating characteristics (ROC) curve analysis (figure 1), no statistically significant influence was observed (p=0.09). We observed with ROC curve analysis that premature birth had a statistically significant effect on the negative prognosis of these anomalies, thus supporting the fact that it constitutes a highly significant predictive negative factor (p=0.0002, area under the curve=0.620).

{kind=link}
Premature birth as a prognostic factor for congenital anomalies.
Discussion
Congenital anomalies are one of the major causes of neonatal morbidity and mortality.1–9 They affect approximately 2% of births in Europe.10 Despite improvements in perinatal care, serious birth defects account for 20% of all newborn deaths and a significant percentage in later morbidity of infant and childhood.1–8
Prenatal diagnosis, as discussed above, has significantly changed our understanding of congenital anomalies that can be treated surgically. Prenatal performance has increased considerably.5 11 From the assessment at several hospital centers in France, a significant increase in prenatal diagnosis was observed from 67.7% in the 1990–1995 period to 80.2% in the 1996–2001 period.12 In our country, despite an increase in prenatal diagnosis, compared with another study of the pediatric intensive care for the period 2000–2005, prenatal diagnosis remains low (19%), different from developed countries. As reported by Pasquier et al 12 and even in our study, the rate of prenatal diagnosis decreases with increasing distance between the residence and the referral center.
In our study 61.1% of cases originate from districts where prenatal diagnosis was ≈10%, affecting significantly the total prenatal diagnosis. It should be noted that prenatal diagnosis remains unsatisfactory in Tirana (≈25%).
Significant progress has been made in the last 50 years in the diagnosis and management of congenital anomalies. Very complex anomalies are treated with success of up to 90%.7 Even in our study we can say with satisfaction that mortality has been reduced significantly, from 31.4% in the first period of 2008–2012 to 24.6% in the second period of 2013–2017. With improvement in prenatal diagnosis, we expected to have probably some changes in the incidence of congenital anomalies, but there seems to be no significant change in the incidence of anomalies over the years, except a slight reduction for intestinal atresia during the second period.
Intestinal atresia is a common cause of neonatal obstruction, secondary to mesenteric vascular accidents during intrauterine life. They constitute the most frequent congenital anomaly, with 73 cases or 23% of all cases with congenital anomalies, followed by anal atresia with 18%, esophageal atresia with 16% and diaphragmatic hernia with 10%.
The incidence of intestinal atresia in our study ranges from 1:3000 to 1:11 000 live births. We underline that intestinal atresia includes duodenal and jejunoileal atresia. Worldwide, the incidence of duodenal atresia ranges from 1:5000 to 1:10 000 live births, whereas for jejunoileal atresia it was 1:400 to 1:2000 live births.13–16 What was observed in our study of intestinal atresia was the reduction of the total number of cases with intestinal atresia by almost 18% in the second period of 2013–2017 (median incidence from 0.23 to 0.19 per 1000 live births). The advances made in recent years in the intensive care, in surgical techniques and in parenteral nutrition have significantly increased the survival of neonates born with jejunoileal atresia.13–16 Surgical correction aims to preserve the bulk of the intestine, often through multiple anastomoses. Of course, there is no need to overcome the importance of prenatal diagnosis, which makes it possible to avoid delayed treatment. All of these elements have made possible a reduction in mortality in 11%–16% over the last decades. Even in our study, we see a satisfactory reduction of mortality from 30% in the first period of 2008–2012 to 18% in the second period of 2013–2017 (OR=0.51, 95% CI 0.17 to 1.57, p=0.24).
Esophageal atresia occupies the third place in surgical congenital anomalies in our country. The incidence in our country varies from 1:4300 to 1:16 600 live births. Worldwide, the incidence of esophageal atresia ranges from 1:2500 to 1:4500 live births.17–19 The prevalence of esophageal atresia has been shown to vary across different geographic settings.20 The highest incidence is described in Finland with 1:2500 live births.17 It is obvious that we are one of the countries with low incidence. There were no changes in incidence, but with high mortality in total compared with developed countries (despite 100% survival during the last year).17 21–23 The survival rate of esophageal atresia in developed countries has reached a plateau since 1980 and seems to be currently stable at around 95%.24 Pedersen et al 17 reported survival from 86.9% to 99.2% for esophageal atresia from 23 European countries in 1987–2006. Calisti et al 22 in their study reported survival from esophageal atresia in 90.6% of cases. In their study neither the age of pregnancy nor the weight at birth seemed to influence the prognosis of this pathology. Mortality was generally associated with associative cardiovascular anomalies and duration in invasive ventilation. Okamoto et al 25 in their study outline that survival of cases with esophageal atresia is associated with birth weight and with major cardiac anomalies. According to them, infants weighing >1500 g and who do not have major cardiac problems should have 100% survival, while the presence of a risk factor decreases survival to 80% and the presence of two risk factors decreases it to 30%–50%.25
Diaphragmatic hernia is one of the challenging anomalies for the intensivist. Its worldwide incidence is estimated to be 1:2000 to 1:5000 live births.26 There were geographic differences within Europe, with higher rates of gastroschisis in the UK and lower rates in Italy.27 The incidence in our country varies from 1:6600 to 1:16 600 live births, confirming that the incidence of this pathology in our country is low. Despite the fact that surgery is simple, choosing the right time for intervention and preoperative and postoperative stabilization remain quite difficult.28–30 This is why mortality of this pathology despite prenatal diagnosis remains high in developed countries as well.26 28–38 Mortality of this pathology is 30%–62%, with more favorable prognosis in the absence of other congenital anomalies.26 29 32 35 38 However, the survival rate in different institutions varies widely from 25% to 95%.26 29 32 35 36 38 Mortality of diaphragmatic hernia remains high in our country (50%–66%), without distinction between the two periods.
Gastroschisis is one of the main congenital anomalies. The incidence of this pathology in our study is approximately 1:11 000 live births. The European Surveillance of congenital anomalies (EUROCAT) workgroup reported that the incidence of gastroschisis increased from 0.60 to 10 000 births in 1980 to 2.33 for 10 000 births in 2000.27 There is no significant difference in the incidence of this pathology between the two periods in our study. To be appreciated is the fact that with the advances that have been made both in the surgical intervention and in the postoperative care, we have a significant reduction of mortality from 40% in the first period of 2008–2012 to 27% in the second period of 2013–2017. Overall, children born with this condition have an excellent prognosis, and today the survival rate is around 90%–95%.39–41
Given the value of prenatal diagnosis such as the emergence of a specialist tertiary center, the avoidance of urgent transfer and the timely completion of corrective surgical intervention, we have evaluated the impact of prenatal diagnosis on mortality. There was no statistically significant difference between the two periods, but it must be pointed out that the level of prenatal diagnosis remains very low in our country giving us clear information that it serves as a predictive positive factor for the prognosis of these pathologies.
Meanwhile, premature birth was a significant predictive factor for the prognosis of children with congenital surgical anomalies. Linhart et al 42 in their study also stressed that congenital anomalies in the preterm are an independent risk factor for neonatal morbidity and perinatal mortality. According to an experience in an Indian tertiary center, prematurity was a significant factor affecting survival.43 Deurloo et al 44 in their study found out that mortality among premature infants was higher than among those born in term (p=0.003). Manchanda et al 45 in their study with multivariate analysis also revealed that only gestational age was a significant predictor of overall mortality.
Conclusion
Incidence of congenital anomalies has not changed over the years in our country. Prenatal diagnosis is increasing recently, although it remains low. Advances in intensive care, surgical techniques and parenteral nutrition made in recent years have significantly increased the survival of neonates born with surgical congenital anomalies. Birth of premature babies was a significantly negative predictive factor for prognosis of these anomalies.
References
Footnotes
Contributors IB conceptualized, supervised data collection and drafted the initial manuscript. RL, EC, DS, IG and DK contributed to the acquisition of data. EK and SS revised the manuscript. DK carried out the statistical analyses and corrected the English version. All authors reviewed the manuscript critically and approved the final manuscript as submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.