Article Text

Abstract
Introduction Pediatric thyroidectomy is performed by a variety of surgical specialties. Thyroidectomy can result in a number of complications. Previous studies cite that the most common complications in children are pain and transient hypocalcemia. The purposes of this report are to assess the adverse events of thyroidectomies performed in the pediatric population and to assess the relationship between surgical specialties and postoperative thyroidectomy complications.
Methods We conducted a cross-sectional analysis of cases from January 1, 2014 through November 1, 2015 using the National Surgical Quality Improvement Program database for patients undergoing excision of cyst or adenoma of the thyroid, unilateral thyroid lobectomy, or total thyroidectomy.
Results Of the 344 patients who underwent thyroidectomy, 10 (2.9%) experienced at least one complication. The most common complications were readmission, surgical site infections, and wound disruption. There was a statistically significant association between complication incidence and surgical specialty (p=0.006). Pediatric otolaryngology had a statistically significantly higher number of complications than pediatric surgery (p<0.008).
Conclusion Overall, the incidence of adverse events following pediatric thyroidectomy was low.
- otorhinolaryngologic diseases
- pediatrics
- endocrinology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Pediatric thyroidectomy is a relatively uncommon procedure.
The most common complications of pediatric thyroidectomy are pain and transient hypocalcemia.
Pediatric otolaryngology procedures generally have a low complication rate.
What are the new findings?
The complication rate of pediatric thyroidectomy was found to be 2.9% in this study.
The most common complications were readmission, surgical site infection, and wound disruption.
The most common reason for readmission was hypocalcemia.
There was a higher percentage of complications when the procedure was performed by pediatric otolaryngology as opposed to pediatric surgery; however, owing to the low complication rate and to possible confounders, this finding is difficult to interpret.
How might it impact on clinical practice in the foreseeable future?
Families should be reassured regarding the safety of pediatric thyroidectomy.
Further efforts to reduce complications such as hypocalcemia should be encouraged.
Introduction
Pediatric thyroidectomy is a relatively uncommon procedure.1 Depending on the indication for thyroidectomy, the patient may undergo partial or total thyroidectomy. While the most frequent complications in children are pain and transient hypocalcemia,2 other potential complications include vocal fold paralysis, nerve injury, vascular injury, tracheal injury, esophageal injury, and mortality.3 4
This analysis uses data from the National Surgical Quality Improvement Program (NSQIP), a national, risk-adjusted program that tracks surgical data and postoperative complications occurring within 30 days. NSQIP data have previously been used to explore complications following adult thyroidectomy.5–8 Additionally, NSQIP data have shown that pediatric otolaryngology procedures generally have a low complication rate.9 At the beginning of this project, there was no similar literature using NSQIP data to investigate complications of thyroidectomy in a pediatric population. During the finalization of this paper, Patel et al10 published an analysis of pediatric complications of thyroidectomy using NSQIP, where they compared complication rates between hemithyroidectomy, total thyroidectomy, and total thyroidectomy with neck dissection.
The goal of this review is to further evaluate the national outcomes of thyroidectomies in the pediatric population. This review differs from Patel et al’s10 review in that it examines a different year of NSQIP data and does not compare the complication rates of specific procedures performed. Moreover, our secondary goal is to assess the pediatric thyroidectomy complication rate as it relates to the specialty of the surgeon. According to previously published literature, the complication rate following pediatric thyroidectomy is associated with surgeon volume.11–13 As such, we hypothesize that there will be a difference in complication rates between surgical specialties. We also examined pediatric thyroidectomy complications in relation to age, gender, race, ethnicity, medical history, and comorbid conditions.
Methods
This retrospective review of NSQIP data were acquired through a Pediatric Participant User File from Lehigh Valley Health Children’s Hospital, an NSQIP participating site. All data were de-identified. The study included all cases from January 1, 2014 through November 1, 2015 with a current procedure terminology code of 60200 (excision of cyst or adenoma of the thyroid), 60220 (unilateral thyroid lobectomy), or 60240 (total thyroidectomy).
Descriptive statistics were generated for the entire sample. All variables related to demographics, complications, and comorbidities tracked by NSQIP were analyzed. Complication rate was calculated for each individual complication along with an overall complication rate. This overall complication rate included the following adverse events: postoperative readmission, postoperative surgical site infection (SSI), death, or reoperation. If a patient experienced a complication more than once within the 30-day follow-up, the patient was only counted as having that complication once. To account for patients being able to experience the same complication more than once, a count of the total number of complications experienced by the sample was computed.
The χ2 test was used to assess if there was an association between surgical specialties and categorical outcomes, and a patient experiencing at least one outcome and categorical outcomes. If >20% of expected cell counts were less than 5, the Fisher’s exact test was used. The Kruskal-Wallis test was used to assess if there was an association between surgical specialties and continuous outcomes, and a patient experiencing at least one outcome and continuous outcomes. Pairwise comparisons were performed to determine which surgical specialty was statistically significantly associated with another. The Bonferroni correction was applied for categorical comparisons, and the Dwass-Steel-Critchlow-Fligner correction was applied for continuous comparisons. SAS (V.9.4) was used to conduct the analysis.
Results
The NSQIP database from January 1, 2014 through November 1, 2015 included 344 patients who underwent a thyroidectomy procedure. The demographics of the sample are shown in table 1. The median age of patients was 14.9 years. There were 89 (25.9%) boys and 255 (74.1%) girls. Majority of patients were white (252, 82.4%) and non-Hispanic (265, 80.1%).
Demographics by surgical specialty (N=344)
Of the total 344 patients who underwent a thyroidectomy procedure, 126 (36.6%) were seen by pediatric otolaryngology, 133 (38.7%) by pediatric surgery, 19 (5.5%) by otolaryngology, and 66 (19.2%) by general surgery (table 1). The specialties of pediatric plastic surgery, plastic surgery, pediatric orthopedics, and orthopedics were not included in this analysis because no patients within this sample were treated by these specialties.
As shown in table 2, 24 (7.0%) patients underwent excision of thyroid cyst or adenoma, 108 (31.4%) underwent unilateral thyroidectomy, 166 (48.3%) underwent total thyroidectomy, and 46 (13.4%) underwent total thyroidectomy with limited neck dissection. There was a significant association between surgical specialty and procedure code (p=0.014). However, when pairwise comparisons were made to determine which surgical subspecialties were significantly different, all pairwise comparisons found no statistical significance (all p>0.008).
Procedure code by surgical specialty
As shown in table 3, 10 of the 344 (2.9%) patients experienced at least one complication, whereas 334 (97.1%) patients did not have any complications. There was a statistically significant association between complication incidence and surgical specialty (p=0.006). The rate of pediatric otolaryngology complications was significantly different from that of pediatric surgery (p<0.008). Pediatric otolaryngology had 6.3% of patients with at least one complication, whereas pediatric surgery had zero patients with at least one complication.
Primary complications by surgical specialty
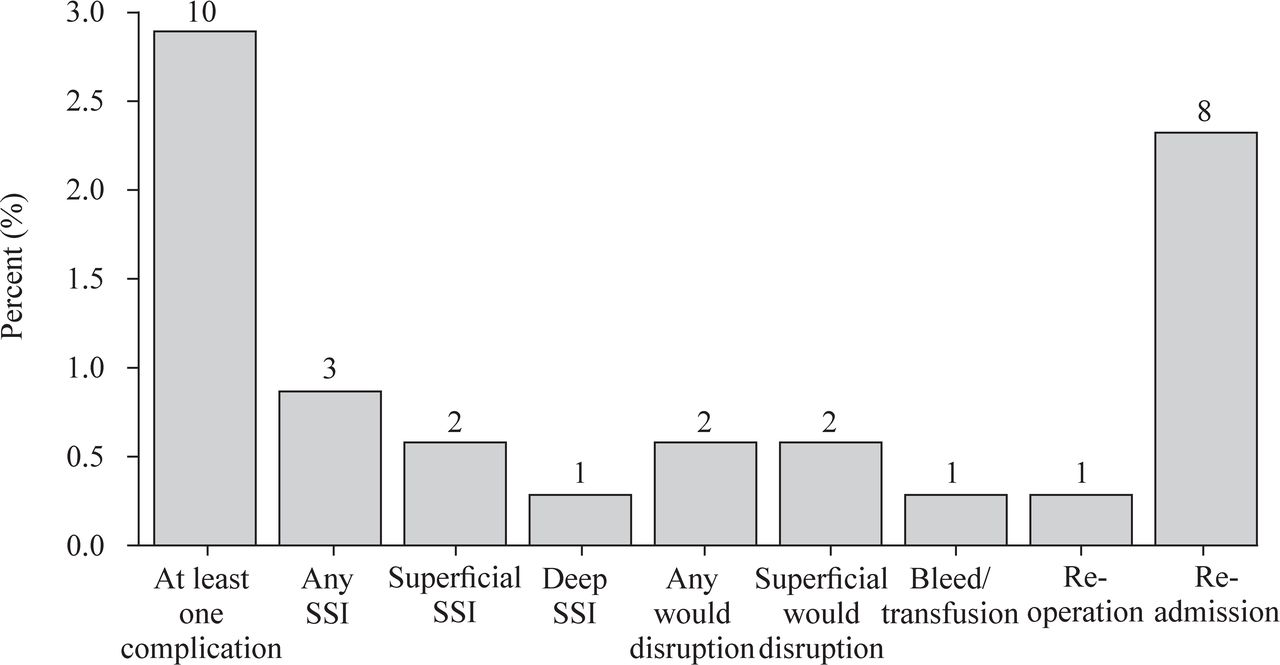
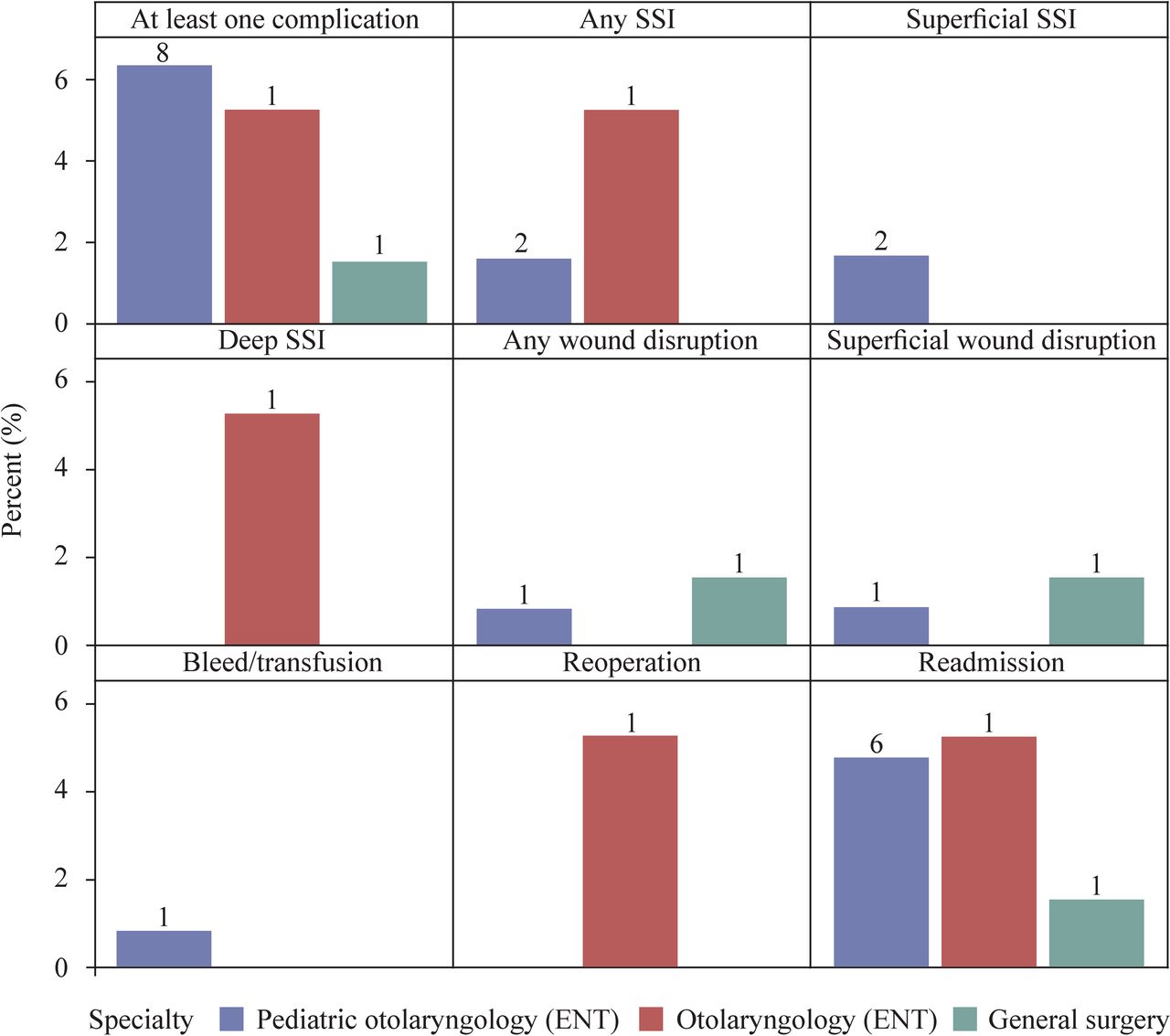
The breakdown of the 10 patients who experienced at least one complication is shown in figure 1. The most common complications were readmission (8 of 10), SSI (3 of 10), and superficial wound disruption (2 of 10). Other complications were bleeding (1 of 10) and reoperation (1 of 10). The breakdown of complications among pediatric otolaryngology, otolaryngology, and general surgery is shown in figure 2. Table 3 shows that among the eight patients who experienced readmission, the most common reason for readmission was hypocalcemia (3 of 8). Other reasons for readmission were deep SSI (1 of 8), sepsis (1 of 8), other (2 of 8), and unknown (1 of 8).

Percentage of patients who experienced each complication. Data label on bar is the number of observations in the group. SSI, surgical site infection.

{kind=link}
{kind=link}
Percentage of patients who experienced a complication within each specialty. Data label on bar is the number of observations in the group. ENT, ear, nose and throat; SSI, surgical site infection.
As shown in table 3, there was a significant association between surgical specialty and a patient having at least one SSI (p=0.044). However, when pairwise comparisons were made to determine which surgical subspecialties were significantly different from each other with regard to patients with at least one SSI, all pairwise comparisons returned as not statistically significant (all p>0.008).
There was also a statistically significant association between surgical specialty and readmission within 30 days (p=0.024). However, when pairwise comparisons were made to determine which surgical subspecialties were statistically different from each other with regard to readmission, all pairwise comparisons returned as not statistically significant (all p>0.008).
Of the patient comorbidities investigated as shown in table 4, the only statistically significant comorbidity associated with complications was previous cardiac surgery (p=0.029). Among the 10 patients who had at least one complication, one of them had a previous cardiac surgery (10%). Table 4 lists other comorbidities by complication status. Patients with other comorbidities did have complications following thyroidectomy, but these other comorbidities did not have a significant association with complication status.
Patient conditions by complication status (n=344)
Discussion
In this assessment of pediatric thyroidectomy from the NSQIP database, the overall complication rate was 2.9%. The most common complication was readmission, followed by SSI and wound disruption. The most common reason for readmission was hypocalcemia. There was a significant association between specialty and experiencing at least one complication, with a higher percentage of complications occurring in pediatric otolaryngology as compared with pediatric surgery. A history of cardiac surgery was significantly associated with complications. Because there is only one patient with a history of cardiac surgery in this sample, it is difficult to assess the relevance of this finding.
The overall incidence of complications following pediatric thyroidectomy is low, which is consistent with previous reports.9 10 According to a study by Zong et al,14 the incidence of postoperative complications was the same for lobectomy and total thyroidectomy in pediatric patients. This is consistent with the findings of Patel et al10 that complication rates were not significantly different between hemithyroidectomy, total thyroidectomy, and total thyroidectomy with neck dissection. The study by Patel et al10 also used NSQIP data to examine the complications of pediatric thyroidectomy. They focused on comparing complications between hemithyroidectomy, total thyroidectomy, and total thyroidectomy with neck dissection, which differed from our review. They identified a total of 29 complications out of 720 cases, for a complication rate of 4.0%.10 This is similar to the complication rate of 2.9% identified in our review.
The complications seen most frequently in our review were readmission, SSI, and wound disruption. This is consistent with the most common complications identified in Patel et al’s NSQIP review.10 In our review, readmission was most commonly due to hypocalcemia. Hypocalcemia is known to be one of the most prevalent adverse events following pediatric thyroidectomy.3 A review of the Kids’ Inpatient Database found that almost 20% of pediatric patients presented with hypocalcemia following thyroidectomy.1 Furthermore, as many as 8% of these patients developed permanent hypocalcemia.1 15 Further research has shown an increased risk of postoperative hypocalcemia in patients of younger age, patients with hyperthyroidism, and those undergoing lymphadenectomy.16 These patients may benefit from closer monitoring to prevent hypocalcemia and from additional guidelines on postoperative calcium supplementation. Compared with the treatment for post-thyroidectomy-related hypocalcemia in adults, there is much less literature about guidelines for the pediatric population. According to the report by Patel et al17 in 2018, an intraoperative parathyroid hormone level can determine whether or not the patient requires an empiric treatment of calcium carbonate and calcitriol. Proper standard management of postoperative pediatric calcium supplementation may help to reduce readmission.
A history of cardiac surgery was significantly associated with postoperative complications, although it was based on the adverse events of only one patient. The exact reason for this association is unclear. One possibility is that pediatric patients undergoing cardiac surgery are likely to have more comorbidities that complicate anesthesia. One study has shown that pediatric patients with a history of cardiac surgery are prone to recurrent laryngeal nerve injury due to exposure of one or both recurrent laryngeal nerves during cardiac surgery.18 Theoretically, this could predispose these patients to complications during thyroidectomy owing to an overlap in the surgical fields. In a pediatric patient, the incision for a thyroidectomy may be close in proximity to the incision for a cardiac surgery, and there may be overlap in the dissection through fibrotic tissue. This may lead to distortion of landmarks. NSQIP data do not allow for specific cases to be examined, so we are unable to further explore the connection between a history of cardiac surgery and complications following thyroidectomy. Case studies of such patients may be helpful in elucidating the reasons for increased complications.
Our study has shown a statistically significant difference in complication rates among surgical specialties, with pediatric otolaryngology having significantly more complications than pediatric surgery. SSI and 30-day readmission showed statistical significance when compared across specialties, but pairwise complications between specialties were not significantly different. It is important to note that while this review examined comorbidities, it did not control for them when comparing complication rates between specialties. While a statistically significant difference was identified, it was entirely possible that this difference was caused by a confounding variable, such as a certain comorbidity, that was not accounted for in the analysis. This difference in complication rate is academically interesting, but we do not believe it to be clinically relevant, especially in the context of the low complication rate found in pediatric thyroidectomy. The overall finding from this review is that pediatric thyroidectomy is generally a safe procedure across specialties.
Previous studies have cited variation in surgical volume as a contributing factor for postoperative complication rates. Tuggle et al13 found that the greatest predictor of low complication rates in pediatric thyroidectomies was whether a particular surgeon had a high volume of similar cases when compared with pediatric specialization. They observed 6% and 11% complication rates for high-volume surgeons and pediatric surgeons, respectively. In addition, Baumgarten et al19 reported that centers with a large pediatric thyroidectomy volume fared better in complication rates compared with centers with a lower volume. A large cohort study reported in JAMA Otolaryngology in 2016 showed that surgeons who performed over 30 thyroidectomies a year tended to have more favorable clinical outcomes.20 These studies demonstrated how variations in volume could contribute to differences in complications. However, the studies do not specify which complications are affected by surgeon volume. It stands to reason that a surgeon’s ability to recognize landmarks and to perform a procedure without damaging nearby structures would improve with practice, and therefore that complications, such as hypocalcemia and recurrent laryngeal nerve damage, would decrease with experience. Other complications seen in this study, such as SSI and wound disruption, may not follow the same pattern.
In this study, it was observed that the volume distribution was relatively comparable between pediatric surgery and pediatric otolaryngology, with pediatric surgery completing 133 cases and pediatric otolaryngology 126 cases. General otolaryngology and general surgery had fewer surgeries (19 and 66, respectively). One drawback to the NSQIP database is that we are unable to determine how many surgeons are performing these cases. It is possible that few pediatric surgeons are performing many thyroidectomies or that many pediatric otolaryngologists are each performing only a few thyroidectomies. Individual surgeon volume could explain the lower complication rate seen in pediatric surgery in this study. Drews et al12 also reported that patients managed by pediatric surgeons had fewer complications than those managed by pediatric otolaryngologists. They attributed this to differences in postoperative management (ie, the use of postoperative laryngoscopy) and to the larger volume of patients seen by pediatric surgeons. Further studies are necessary to elucidate possible reasons for varying complication rates between specialties.
The number of thyroidectomies and lobectomies has been climbing steadily since 2006. According to Sosa et al21 there have been over 350 000 procedures done from 2009 to 2011 in the USA. For the pediatric population, however, thyroidectomy and partial thyroidectomy are not common procedures. A recent study indicated that a combined total of 2753 procedures were done from 2009 to 2012 in the USA.1 In this study, only 344 cases are documented, among which 2.9% experienced postoperative complications. The small number of complications is a limitation of this study. This low statistical power made it difficult to analyze the complications. The NSQIP database is an asset in that it allows for analysis of far more patients than in any single institution. However, NSQIP is largely designed to examine complications related to general surgery. As such, it does not track all variables relevant to pediatric thyroidectomy, such as hypocalcemia which does not result in readmission. This report did find that patients operated on by pediatric otolaryngologists presented with a higher percentage of postoperative complications. It is uncertain whether these higher incidences of complications are related to previous existing comorbidities or to a surgeon’s volume. A closer look at these factors for post-thyroidectomy complications is needed in the future, especially with a larger study population size. Given the limited number of postoperative complications documented in the current study, it is difficult to draw causal conclusions. However, the complication rate found in this study is low, and pediatric thyroidectomy is a generally safe procedure.
Acknowledgments
A special thanks to Jennifer Macfarlan, MPH, and Shae Duka, BS, biostatistician and research assistant, at the Network Office of Research & Innovation at Lehigh Valley Health Network, for their hard work and statistical analysis, and to Debra Trexler, RN, for helping us collect the data needed for our review.
References
Footnotes
Twitter @harry_young_shi
Contributors AS, HT, WD, and CSK developed the initial study design. AS, HT, and WD obtained and organized the NSQIP data set. AS, RJ, SH, MJ, and CSK were responsible for writing and editing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was reviewed and deemed quality improvement by the Lehigh Valley Health Network Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. The data analyzed in this work were obtained from the National Surgical Quality Improvement Program (NSQIP) data repository. NSQIP data access can be requested by participating sites through the following website: https://www.facs.org/quality-programs/acs-nsqip.