Article Text

Abstract
Background Pediatric patients affected by scoliosis have complex psychological and social care needs, and may benefit from psychosocial interventions. We therefore aimed to summarize evidence of the efficacy of psychosocial interventions for this patient population.
Methods Literature was identified by searching Medline, PsycINFO, Embase, EBSCO Cumulated Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Central Register of Controlled Trials (CENTRAL) from database inception to 20 March 2022. Articles that evaluated the effectiveness of psychosocial interventions for pediatric patients diagnosed with scoliosis and reported at least one quantitative outcome were included. Article eligibility, data extraction, and quality assessment (using the Cochrane Collaboration’s Risk of Bias Tool and Methodological Index for Non-Randomized Studies) were performed by two independent researchers. Findings are presented using narrative synthesis.
Results We identified ten studies, all of which focused on adolescent idiopathic scoliosis. Studies included a total of 1007 participants, most of whom were female. Three studies focused on patients undergoing bracing, six on patients undergoing spinal surgery, and one on patients broadly. Brace compliance monitoring and counseling were found to significantly improve brace compliance quality and quantity. Proactive mental healthcare delivery by nurses after spinal surgery was similarly found to improve outcomes. Several studies examined the efficacy of brief educational interventions; most did not report clear evidence of their efficacy. The methodological quality of studies was often unclear due to limitations in articles’ reporting quality.
Conclusions Research on the efficacy of psychosocial interventions for pediatric patients with scoliosis is limited, with interventions involving frequent patient-provider interactions showing the most promise. Future clinical and research efforts should focus on developing and testing psychosocial interventions for this patient population, with emphasis on multidisciplinary teams delivering holistic care.
Trial registration number PROSPERO number CRD42022326957
- Psychology, Child
- Orthopedics
- Musculoskeletal Diseases
- Health Services
- Child Psychiatry
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ABOUT THIS TOPIC
Pediatric patients affected by scoliosis have complex psychosocial care needs and may benefit from psychosocial interventions, however a comprehensive overview of this evidence base is lacking.
WHAT THIS STUDY ADDS
We therefore conducted a systematic review of the efficacy of psychosocial interventions for pediatric patients with scoliosis.
We found interventions involving frequent patient-provider interactions improved pediatric patients’ outcomes the most, with brace compliance monitoring and counselling significantly improving brace compliance quality and quantity, and proactive mental healthcare delivery by nurses following spinal surgery also improving mental and physical health outcomes.
Several studies examined the efficacy of less intensive, brief educational interventions; most did not report clear evidence of their effectiveness.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
Research on the efficacy of psychosocial interventions for pediatric patients with scoliosis remains limited; therefore, we propose that future clinical and research efforts be directed towards developing psychosocial interventions for this patient population, particularly those emphasizing multidisciplinary teams delivering holistic care.
Introduction
Scoliosis can dramatically alter a child or adolescent’s daily life.1 2 During and after diagnosis, affected patients and their caregivers report numerous physical, psychological, and social care needs.1–4 Effective management of scoliosis therefore requires holistic care that addresses these complex needs—failing to do so can lead to poor physical and mental health outcomes.1 3 5
Several systematic reviews have been published on surgical, bracing, and exercise interventions to improve outcomes in pediatric patients with adolescent idiopathic scoliosis (AIS).6–13 However, there are no reviews that have comprehensively summarized literatures on the effectiveness of psychosocial interventions for this patient population, with existing reviews focusing primarily on describing pediatric patients’ and caregivers’ psychosocial well-being.2 3 14 It is critical to have an overview of this evidence base because psychosocial interventions may offer a means of significantly improving biopsychosocial outcomes, as has been suggested by qualitative literature in the field.1 15
Therefore, this systematic review aims to summarize evidence of the efficacy of psychosocial interventions on patient and health service outcomes (such as psychological symptoms, treatment compliance, and healthcare utilization) among pediatric patients with scoliosis in any setting.
Methods
Study design
This systematic review was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.16–18 Its protocol was prospectively registered and available on International Prospective Register of Systematic Reviews (PROSPERO).19
Search strategy
Relevant literature was identified by searching Medline, PsycINFO, Embase, EBSCO Cumulated Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Central Register of Controlled Trials (CENTRAL) from database inception to March 2022. No language or publication date restrictions were applied. Searches were run for a combination of ‘psychosocial intervention’, ‘pediatric’, and ‘scoliosis’ using standardized subject and free-text terms, including synonyms and alternative spellings (online supplemental material 1). The search strategy was developed in collaboration with an information specialist (CW). Manual reference list searches of the articles included were conducted. We also searched for gray literature by (1) contacting authors of relevant conference abstracts or dissertations found through the electronic database search for associated publications and (2) screening ClinicalTrials.gov and WHO International Clinical Trials Registry Platform (ICTRP) for completed relevant trials.
Supplemental material
Selection criteria
Articles were included if they met the following selection criteria: (1) the study aimed to evaluate the effectiveness of a psychosocial intervention (defined below); (2) participants were pediatric patients (aged ≤21 years, the highest threshold used for defining pediatric patients in research and clinical practice) diagnosed with scoliosis; (3) the study reported at least one quantitative patient outcome (eg, psychological symptoms, treatment compliance) or health service outcome (eg, healthcare utilization) at any follow-up timeframe; (4) the full text was available to allow for data extraction and quality appraisal; and (5) the article was a primary study (ie, not review, editorial). We included all randomized controlled trials (RCTs) examining the efficacy of psychosocial interventions, irrespective of the comparison group used. We did not anticipate finding a large number of RCTs and therefore broadened our selection to include non-randomized studies as well.
We defined psychosocial interventions as ‘interpersonal or informational activities, techniques, or strategies that target biological, behavioral, cognitive, emotional, interpersonal, social, or environmental factors with the aim of improving health functioning and well-being’.20 Our review included studies whose intervention included a core psychosocial component (such as counseling, psychoeducation, or coordination of care). We excluded studies concentrating primarily on comparing surgery, bracing, or exercises with usual care, as their findings were unlikely to elucidate the impact of psychosocial interventions.
Data collection
All articles identified through the database search were imported into Covidence, an electronic software platform for managing reviews. Two independent reviewers (MvN did all of them and AR and KT split their role) screened articles’ titles and abstracts to determine if they met selection criteria and reviewed the full text of all articles deemed to be potentially relevant. Two reviewers (AR and MvN) independently (1) extracted the following data from eligible articles: study setting; study design; sample characteristics; intervention group and control group characteristics; all patient or healthcare outcome measure(s); and associated result(s) (eg, mean difference), and (2) conducted quality assessments of all randomized and non-randomized studies using the Cochrane Collaboration’s Risk of Bias Tool and Methodological Index for Non-Randomized Studies, respectively.21 22 Disagreements in article inclusion, data extraction, or quality assessment ratings were resolved through consensus discussion with a third independent reviewer (KT and JV).
Data analysis
The findings of the systematic review are presented using narrative synthesis and tables, highlighting the results of all outcome measures reported in eligible articles. Heterogeneity between psychosocial interventions included in the review (1) precluded pooling findings by meta-analyses and (2) made conducting formal analyses of causes of heterogeneity between studies unnecessary.
Results
Overview
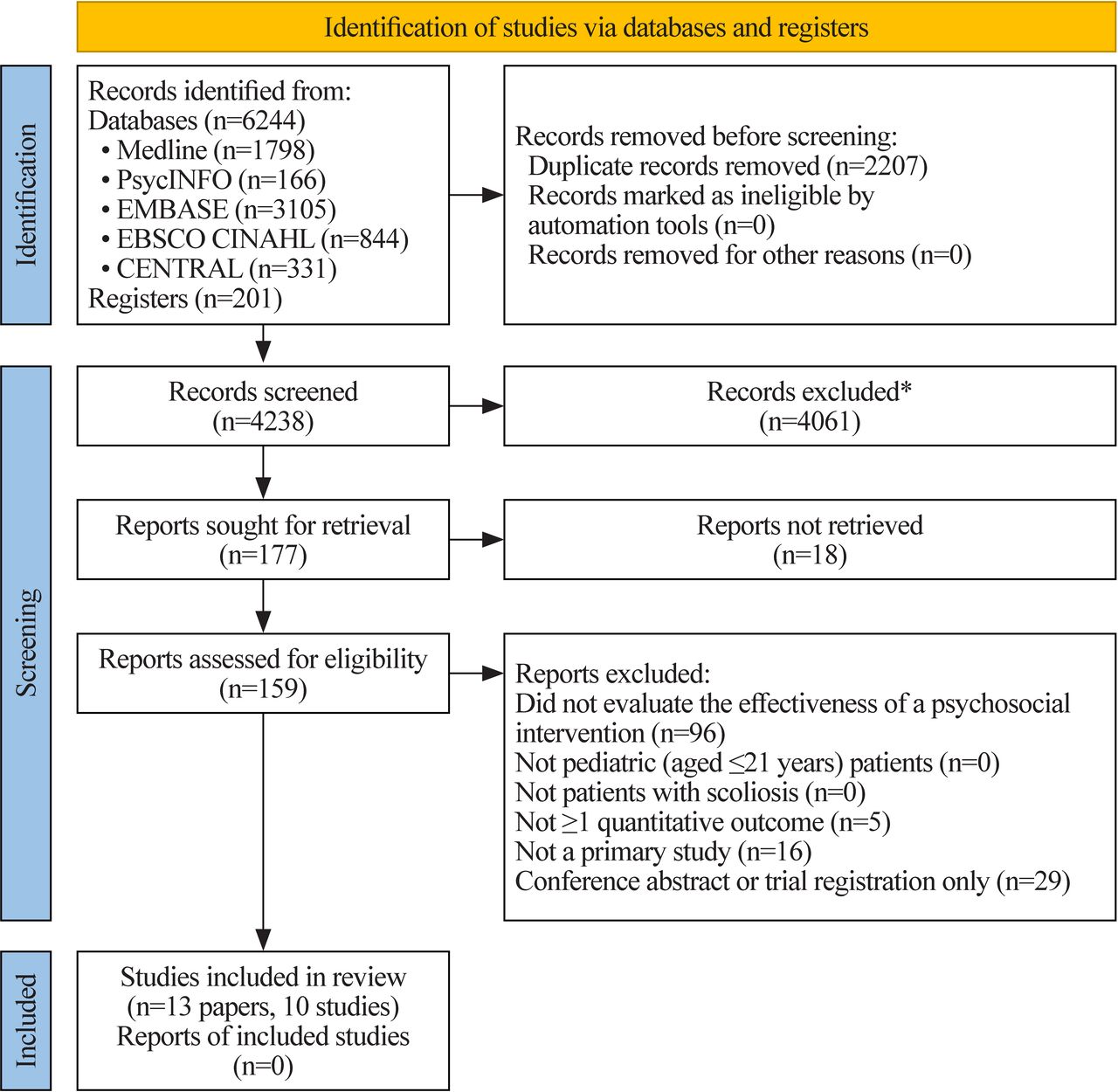
Totally, 6445 articles were identified through the electronic database and register searches. After removal of duplicates, 4238 titles and abstracts were screened, yielding 177 articles for full review. A total of 146 articles were excluded after reviewing the full paper, and 18 articles did not have full texts available for review. Ten studies (described in 13 papers) met the selection criteria, all of which focused on AIS (figure 1).23–35

{kind=link}
Systematic review flow chart (adapted from Page et al18). *Duplicates excluded via automation tool, Covidence. CENTRAL, Cochrane Central Register of Controlled Trial; EBSCO CINAHL, Cumulated Index to Nursing and Allied Health Literature.
We included six clinical trials,23 28–34 three cohort studies,24–27 and one cross-sectional study.35 The included studies analyzed relatively small sample sizes (mean (range) of analyzed sample sizes: 101 (28–237)). Studies were primarily comprised of female adolescents (mean age range: 12–16 years; percentage of female range: 64%–100%). Five studies were conducted in the United States,23 29–33 35 two in China,25 26 34 one in Japan,24 one in Malaysia,27 and one in Canada.28 Four studies were conducted in the past 5 years,25–27 32 34 with publication dates ranging from 1985 to 2021.
Interventions for patients undergoing bracing
Three studies (described in four papers) focused on patients with AIS undergoing bracing treatment (online supplemental table 1).23–26 The studies analyzed a total of 344 participants, with the vast majority of participants being female (82%–100%).23–26 Participants who wore thoracic lumbar sacral orthosis (TSLO) braces were included in two studies,23 24 Milwaukee braces in one study,24 and Chêneau braces in one study.25 26 Studies examined two main categories of interventions: (1) brace compliance monitoring and counseling23 25 26 and (2) mental health-informed treatment planning.24
Brace compliance monitoring and counseling
Two studies investigated the use of brace compliance monitoring and counseling in improving brace compliance.23 25 26 Both studies found evidence that this intervention significantly improved outcomes.23 25 26 Karol et al23 conducted an RCT and found that adolescents who received brace compliance reports and whose providers similarly received these reports and offered compliance counseling wore their TSLO braces significantly longer than those who did not. Zhu et al25 26 incorporated a mobile phone application for providers to offer real-time compliance monitoring and counseling. They similarly found a significant increase in brace compliance quantity and quality over time following this interaction.25 26 Almost all participants were very or somewhat satisfied with this form of monitoring.25 26
Mental health-informed treatment planning
Matsunaga et al24 conducted a prospective cohort study examining the efficacy of reducing patients’ emotional distress by tailoring bracing treatment plans based on patients’ mental well-being; for example, switching a patient from full-time bracing to part-time bracing if they demonstrated ongoing emotional distress. They found that, over time, there was a significant decrease in the percentage of individuals who were emotionally distressed.24 While it is possible that tailoring patients’ bracing therapy helped improve emotional outcomes, it could also be that patients’ emotional distress decreased over time for other reasons, such as getting used to wearing their brace.
Key takeaways
In patients undergoing bracing, we found prospective and trial evidence demonstrating that brace compliance monitoring and counseling can help improve brace compliance, and prospective evidence that tailoring brace treatment plans based on mental health outcomes may reduce emotional distress.
Interventions for patients undergoing spinal surgery
Six studies (described in eight papers) focused on patients with AIS undergoing spinal surgery (online supplemental table 2).27–34 The studies analyzed a total of 426 participants.27–34 Most were RCTs,28–34 and all but one study excluded patients with psychological, cognitive, and/or developmental conditions.27–31 33 34 Studies examined two main categories of interventions: (1) brief educational interventions28–30 32 33 and (2) intensive multidisciplinary care models.27 34
Brief educational interventions
Four of the six studies examined the efficacy of brief educational interventions for patients in managing postspinal surgery pain and/or anxiety.28–30 32 33 The interventions were heterogeneous, incorporating components such as guided imagery and relaxation training,28–32 concrete medical information teaching,29–31 33 and music therapy.32 In general, most studies did not report convincing evidence of brief educational interventions being more efficacious than routine medical care in improving outcomes.
Interestingly, Charette et al28 found that patients randomized to receive a short audiovisual intervention of guided imagery and relaxation exercises for postoperative pain management had significantly lower pain levels at discharge and 1 month postdischarge than those who received routine medical care. However, when LaMontagne et al29 30 conducted a similar trial comparing audiovisual interventions of coping and/or concrete medical information training with routine medical care, they did not report significant between-group differences in anxiety or pain levels, except in subgroup analyses (eg, patients under 14 years and highly anxious patients).
Although most studies compared interventions with routine medical care, one RCT by Nelson, Adamek, and Kleiber did not.32 In this trial, both study groups received postoperative music therapy, with one also receiving preoperative music-assisted relaxation training.32 Researchers reported significant within-group, but not between-group, differences in anxiety and pain levels, highlighting the need for research comparing music therapy with routine care alone.32
Intensive multidisciplinary care models
Two of the six studies examined the efficacy of intensive multidisciplinary care models for adolescents with scoliosis after spinal surgery.27 34 Both studies reported improvements in patient outcomes, with one focusing on mental health outcomes, pain levels, and satisfaction with care, and the other on length of hospital stay.27 34
The first study was an RCT conducted by Ying and Fu,34 which compared routine nursing care with Rosenthal effect based nursing, where nurses offered proactive mental healthcare post spinal surgery and provided mental health training for family members to monitor patients’ mental well-being.34 Researchers reported that the intervention was significantly more efficacious than routine medical care in improving depressive and anxiety symptoms, quality of life, pain levels, and satisfaction with nursing.34
The second study was a prospective cohort study conducted by Chan et al,27 which compared an accelerated recovery protocol for adolescents undergoing spinal fusion surgery (described further in online supplemental table 2) with an earlier audit of routine medical care, reporting reductions in length of hospital stay after implementation of the protocol.
Key takeaways
In patients undergoing spinal surgery, we found inconsistent trial evidence of the efficacy of brief educational interventions on reducing postsurgical anxiety or pain, but improvements in these outcomes (as well as depressive symptoms, quality of life, and satisfaction with care) via proactive mental healthcare delivery by nurses following spinal surgery. This shows the importance of intensive multidisciplinary care.
General interventions
Only one study included in this review broadly focused on patients with scoliosis (ie, not specifically bracing or spinal surgery) (online supplemental table 3).35 Hinrichsen, Revenson, and Shinn35 performed a cross-sectional study in 1985 comparing the psychological well-being of adolescents who attended a scoliosis self-help group with those who sought information about the group but did not yet attend. They found no significant between-group differences for most outcomes, including psychosomatic symptoms.35
Quality assessments
We summarize the results of our quality assessments in online supplemental tables 4 and 5.21 22 It was difficult to conduct quality assessments for many of the included studies due to limitations in their reporting quality, consequently also resulting in relatively low certainty in the body of evidence. For example, most RCTs did not clearly report their allocation concealment or outcome assessor blinding procedures, or lack thereof. Many non-randomized studies also did not clearly describe their sampling procedures, outcome assessor blinding procedures, or sample size calculations. Notably, several RCTs were deemed to have a high risk of bias for participant and clinician unblinding, incomplete outcome data, and selective outcome reporting.
Although not assessed by the quality assessment tools, it should be noted that a number of the studies were conducted more than 5 years ago, with one conducted in 1985 and several in the early 2000s.24 29–31 35 This may reduce their relevance and applicability to current clinical practice.24 29–31 35
Discussion
Main findings
This systematic review aimed to summarize evidence of the efficacy of psychosocial interventions on patient and health service outcomes (such as psychological symptoms, treatment compliance, healthcare utilization) among pediatric patients with scoliosis in any setting. Ten eligible studies (described in 13 articles) were identified, all focusing on patients with AIS. More specifically, three focused on those undergoing bracing, six on those undergoing spinal surgery, and one on patients broadly. Brace compliance monitoring and counseling were found to significantly improve brace compliance quality and quantity in adolescents with scoliosis. Proactive mental healthcare delivery by nurses after spinal surgery was also found to significantly improve mental and physical health outcomes for these patients. Several studies examined the efficacy of brief educational interventions on postsurgical anxiety and/or pain; most did not report clear evidence of interventions being more efficacious than comparator interventions.
Discussion of main findings
Bracing
Given the large body of literature highlighting poor brace compliance among pediatric patients with scoliosis and the importance of compliance for effective treatment outcomes, it is crucial that we find clinically effective and cost-effective mechanisms to improve brace compliance.5 Proactive brace compliance monitoring and counseling could be one such intervention,23 25 26 as it allows patients to receive timely, frequent, and individualized advice from providers, preventing them from ‘falling through the cracks’. Implementing this intervention via mobile apps may be particularly feasible because it would overcome barriers associated with inperson visits.25
Spinal surgery
Anxiety and pain management are key concerns for patients with scoliosis undergoing surgery.29 We found some evidence to support using brief audiovisual interventions to help manage pain in these patients.28 We also found that interventions should be tailored to specific patient populations; for example, teaching coping techniques may be particularly helpful for young adolescents.29 30 Given that these interventions are brief, they may offer a relatively easy way for surgical services to equip their patients with techniques to manage their anxiety and pain.29 That being said, intensive multidisciplinary interventions which are more resource-intensive are likely the most effective way of improving outcomes for these patients (eg, training providers to provide proactive preoperative and postoperative mental healthcare).34
Other relevant literature
To our knowledge, this is the first systematic review to examine the effectiveness of psychosocial interventions for pediatric patients with scoliosis. However, there are a number of additional relevant reviews worth noting.
Our review only included studies that reported quantitative data, as another recent review by Essex et al1 summarized relevant qualitative data. They highlighted the complex biopsychosocial needs of adolescents with scoliosis, including body image concerns and limitations in everyday activities.1 They also described several encouraging ‘simple’ interventions, including poetry writing and co-designing scoliosis braces, that may improve patient outcomes.1 However, reviewers also found that patients were often not adequately supported by providers, noting a need for improved information provision, ongoing emotional support (particularly to overcome barriers to brace compliance), and greater general attentiveness of clinical staff.1
Furthermore, our review only focused on pediatric patients with scoliosis because another review by Motyer et al3 summarized evidence on the experiences of parents of children with scoliosis, highlighting their information needs, treatment concerns, and psychological well-being. They found that parents often lacked treatment knowledge and consequently turned to the internet for information, which resulted in more confusion and distress.3 Therefore, they highlighted the importance of evidence-based resources for parents.3 Parents were also found to experience high levels of psychological distress and concern about their child’s treatments.3 Researchers have emphasized the important role that providers have in consistently supporting parents.3
Recommendations for future research and clinical practice
On completion of our review, we organized a consultation meeting, where we presented the review findings to a diverse group of scoliosis experts at our institution, including pediatric orthopedic surgeons, nurses, physical therapists, social workers, psychologists, researchers, and people with lived experience. After providing detailed descriptions of the included studies in the review, as well as the overall review results, we asked them to share their perceptions of integrating the interventions into clinical practice. Overall, group members were supportive of the proactive brace compliance monitoring and counseling intervention, but simultaneously cautioned against making patients feel ‘guilty’ when implementing this intervention. Group members also saw the value of intensive multidisciplinary interventions, such as training a provider to proactively deliver mental healthcare, as depicted in the study on Rosenthal effect-based nursing. Based on their clinical expertise, group members also recommended implementing structured support groups and one-on-one peer mentorship programs for patients and their caregivers, as well as developing evidence-based resources with practical information on living with scoliosis; these suggestions mirror those made in the two systematic reviews previously described.1 3 However, it should be noted that while peer support interventions have been shown to have potential value, limitations in the quality of the literature have prevented strong conclusions regarding their efficacy.36 37
We recommend that future clinical and research efforts be directed towards developing and implementing innovative models of care that integrate multiple interventions shown to have the most promise in the literature and clinical practice. One such model of care recommended by the World Health Organization (WHO) is case management (CM).38 CM often involves adding a new member to the care team, a case manager, to improve the coordination and delivery of holistic care.39 When appropriately implemented, CM has been found to have the potential to improve high-quality care for populations with diverse conditions.40 However, the efficacy of these types of complex, multidisciplinary models of care requires further investigation in pediatric patients with scoliosis. In addition, future research efforts should focus on other patient populations with scoliosis, such as those with neuromuscular scoliosis.
Strengths and limitations
This systematic review has several strengths which include: (1) using a comprehensive search strategy developed with an information specialist to find all relevant published literature; (2) not applying language or publication date restrictions; (3) minimizing selection bias by preregistering our protocol and using two independent reviewers for study selection; (4) minimizing reporting bias by using two independent reviewers for data extraction and quality assessments; (5) conducting rigorous quality assessments of all included studies; and (6) searching for gray literature.
This systematic review also has limitations which include the inclusion of: (1) a small number of studies, often with poor reporting quality; (2) non-randomized studies; (3) studies conducted more than five years ago, including one from 1985 and several from the early 2000s; (4) studies that almost exclusively focused on female adolescents with scoliosis, with little to no consideration for other populations, such as those with neuromuscular scoliosis; (5) studies that typically developed and tested brief one-off interventions, rather than intensive interventions or models of care likely to change overall care offered to those with scoliosis; and (6) studies that provided scant evidence of the efficacy of psychosocial interventions on physical health outcomes or long-term health outcomes. Other limitations of our review include: (1) our inability to conduct statistical analyses due to psychosocial intervention heterogeneity and (2) our gray literature search not retrieving any additional published literature for inclusion. However, we were encouraged to discover that a number of trials in this field are underway or have recently been completed, which will provide further insight into the effectiveness and potential of certain interventions.
Conclusions
Research on the efficacy of psychosocial interventions for pediatric patients with scoliosis is limited, with interventions involving frequent patient-provider interactions showing the most promise. Examples of such interventions include brace compliance monitoring and counseling, as well as proactive mental healthcare delivery by nurses after spinal surgery. Future clinical and research efforts should focus on developing and testing psychosocial interventions for this patient population, with emphasis on multidisciplinary teams delivering holistic care. Efforts should also be devoted to focusing on other patient populations with scoliosis aside from AIS, such as those with neuromuscular scoliosis.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Dr Anya Griffin, Dr Christian Klemt, Dorothy Fung, Jasmin Dinneen, Jennifer Adams, Dr Jim Policy, Lauren Roos, Dr Lawrence Rinsky, Dr Meghan Imrie, Michael Petersen, Mira Cheng, Mona Hussain, Shelby Oldenkamp, Tracy Adebiyi, and Xochitl Bryson for offering their scoliosis expertise to aid in the interpretation of the results of this systematic review. The views expressed in this paper are those of the authors and not necessarily those of the aforementioned individuals.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MvN: Study design, search strategy, study selection, data extraction, interpretation of findings, manuscript writing, manuscript edits, guarantor of study. AR: Study selection, data extraction, interpretation of findings, manuscript edits. JV: Study selection, interpretation of findings, manuscript edits. CW: Search strategy, manuscript edits. KT: Study design, search strategy, study selection, interpretation of findings, manuscript writing, manuscript edits, guarantor of study.
Funding This research was funded by Stanford University School of Medicine. The funder had no role in the study design, search strategy, study selection, data extraction, interpretation of findings, or manuscript writing.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.