Article Text

Abstract
Background Childhood neurosurgical conditions such as hydrocephalus and spina bifida represent a significant burden of death and disability worldwide, particularly in low and middle-income countries. However, there are limited data on the disease prevalence and delays in care for pediatric neurosurgical conditions in very low-resource settings. This study aims to characterize the delays in access to care for pediatric neurosurgical conditions in Somaliland.
Methods We performed a retrospective review of all children with congenital hydrocephalus and spina bifida admitted to the Edna University Hospital (EAUH) in Somaliland between 2011 and 2018. Patient demographics were analyzed with descriptive statistics and χ2 test statistics. We defined delays in care for each condition based on standard care in high-income settings. Univariate and multivariate logistic regression were performed to evaluate predictors of delay in care. Statistical significance was set at p<0.05.
Results A total of 344 children were admitted to EAUH with neurosurgical conditions from 2011 to 2018. The most common condition was congenital hydrocephalus (62%). Delays in care were found for 90% of patients and were associated with the type of diagnosis and region. The longest delay among children with spina bifida was 60 months, while the longest delay for children with congenital hydrocephalus was 36 months. Children with congenital hydrocephalus or spina bifida traveling from foreign countries had the highest waiting time to receive care, with a median delay of 8 months (IQR: 5–11 months) and 4 months (IQR: 3–7 months), respectively.
Conclusion We found significant delays in care for children with neurosurgical conditions in Somaliland. This country has an urgent need to scale up its surgical infrastructure, workforce, and referral pathways to address the needs of children with hydrocephalus and spina bifida.
- neurosurgery
- congenital abnormalities
- epidemiology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a notable lack of pediatric neurosurgical care for congenital anomalies around the world, especially in low and middle-income countries.
Delays in access to pediatric neurosurgical conditions lead to poor outcomes, lifelong disabilities, increased risks of mortality, and high rates of financial catastrophe for families.
The scarce data on epidemiology and delays in care for neurosurgical conditions have limited the ability for policymakers to strategically allocate resources in the poorest regions.
WHAT THIS STUDY ADDS
We found that over 90% of pediatric patients in our cohort experienced delays to access care for congenital hydrocephalus and spina bifida.
Rural residence and spina bifida diagnosis were identified as significant predictors of delayed neurosurgical care.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
With a high demand and extensive delays for pediatric neurosurgical care, Somaliland needs a comprehensive scale-up of its surgical system to achieve timely and high-quality surgical interventions that lead to improved outcomes.
We expect our results to inform next-step interventions aimed to scale pediatric neurosurgical care at a regional and national levels.
Introduction
With an epidemiological transition towards a high burden of non-communicable diseases in children, there is a notable lack of pediatric neurosurgical care around the world, especially in low and middle-income countries (LMICs).1 Access to timely, safe, and high-quality neurosurgical care remains challenging for children in many LMICs. Congenital anomalies, such as spina bifida and hydrocephalus, are more prevalent in LMICs compared with high-income countries (HICs).1 2 The reasons for the higher incidence of congenital conditions in LMICs are unclear, although it may be related to decreased use of prenatal folic acid intake and genetic and environmental factors.
Care for pediatric neurosurgical conditions in LMICs is often markedly delayed compared with high-income settings.3–6 Delays in access to pediatric neurosurgical conditions lead to poor outcomes, lifelong disabilities, increased risks of mortality, and high rates of financial catastrophe for families.7 8 Most existing studies suggest that less than 25% of the population in Sub-Saharan Africa has timely geographic access to neurosurgical services.9 However, the limited availability of data on disease burden as well as delays in care has limited the ability for policymakers to strategically allocate resources for neurosurgical care for children in the world’s poorest regions.10
Our goal was to define gaps in neurosurgical care for children in Somaliland, one of the poorest regions of the world.11 Our previous studies found a high burden of unmet surgical care for children as well as delays in receiving care for many congenital anomalies.6 12–18 Our current study aims to extend these observations to characterize the delays in care for pediatric neurosurgical conditions in Somaliland. Second, we aim to determine the predictors of delays in care for children with these conditions.
Methods
Setting
Somaliland is one of the world’s poorest regions in the world, with a gross domestic product of $675 per capita.11 ,19 The country has an under-five mortality rate of 117 per 1000 live births, infant mortality rate of 74 per 1000 live births, and neonatal mortality rate of 37 per 1000 live births.20 These rates fall far from global rates of 37 under-five deaths per 1000 live births,21 29 infant deaths per 1000 live births,22 and 17 neonatal deaths per 1000 live births.23 Somaliland includes six regions: Awdal, Maroodi Jeex, Sahil, Sanaag, Sool, and Togdheer. The Edna Adan University Hospital (EAUH) is the largest hospital in the country, and the primary site for the delivery of pediatric neurosurgical care in the country. The hospital has three operating rooms, five anesthesia machines, and three ventilators. The EAUH is located in the most densely populated region of Maroodi Jeex in capital city of Hargeisa. EAUH serves children from across the country as well as from neighboring countries of Ethiopia, Djibouti, and Somalia.
Data collection
This retrospective hospital-based study includes data on all pediatric patients up to 15 years old who were admitted with pediatric neurosurgical conditions to EAUH between 2011 and 2018. Data were extracted from medical records and surgical logbooks and included age, sex, year of admission, country, region of residence, diagnosis, condition type, management, and outcomes. Postoperative outcomes were defined as the status of the patient (alive with no complications, alive with complications, or died) up to a week after surgery. All data were collected by local health workers from EAUH.
Data analysis
Proxy set of neurosurgical conditions
Congenital hydrocephalus and spina bifida were chosen as proxy conditions for analyzing pediatric neurosurgical care, as these were the most common pediatric neurosurgical conditions and the date of onset of the condition can be defined as the date of birth, facilitating the determination of delays in care. We summarized data from all children admitted with these two conditions from January 2011 to December 2018 at EAUH (n=405). We excluded 19 children with other diagnoses, including encephalocele, subdural hematoma, brain tumor, or shunt complications. Hydrocephalus was defined as congenital if this information was stated as present at birth in the medical records or surgical logbooks. For patients with missing data regarding the type of hydrocephalus, only children up to 3 years of age were included under the assumption that they had congenital hydrocephalus. Children with acquired hydrocephalus (n=42) were excluded from the final sample size. Our final sample size included 344 children.
Calculation of delays to care
We defined the presence of delays in care for congenital hydrocephalus and spina bifida as receiving care beyond the expected period following diagnosis based on common international standards, specifically 1 month after birth for congenital hydrocephalus and 48 hours after birth for spina bifida.24 25 Otherwise, patients were considered as receiving timely care. For patients presenting with a diagnosis of both hydrocephalus and spina bifida, we used spina bifida as diagnosis for classification of delay. Delays in care were depicted by using a stratified box plot with sex and region as the first layer and type of diagnosis as a sublayer. The comparison of delay (medians in months) was performed with Kruskal-Wallis test with statistically significant comparisons defined as p<0.05.
Predictors of delayed care
Univariable and multivariable logistic regression analyses were performed to define the predictors of delays in care. Sex, year of admission, region, diagnosis, and condition type were assessed as exposure variables. Delay was assessed as a binary outcome variable (yes or no) as receiving care beyond the time periods described above. Only variables with a statistical significance of p<0.20 from the univariate models were included in the multivariate model. Statistical significance was set at p<0.05 for the multivariate model. Outlier analysis was performed to enhance model fitting. We decided to exclude one child with the largest outlier (hospital admission age: 180 months) in the data set because the differential percent change between the model with and without the outlier was only <2%. All analyses were performed with SAS V.9.4 (SAS Institute) and Tableau (2021.3).
Results
A final sample of 344 children admitted to EAUH with neurosurgical conditions were included in this study (table 1). Most children had congenital hydrocephalus (62.2%), 15.4% had spina bifida, and 22.4% had both hydrocephalus and spina bifida. Most patients traveled from the urban region of Madoori Jeex (39%) and other regions in Somaliland (38%). However, a significant number of patients (23%) traveled from neighboring countries, including Djibouti, Ethiopia, and Somalia. Patients from Maroodi Jeex presented at younger ages compared with other regions (30.6% vs 11.4% for <1 month, and 7.5% vs 15.2% for >1 year). Delays in care were found for 90.1% of the patients, with children from other regions in Somaliland concentrating the biggest proportion of delays (40.0%), followed by children from Maroodi Jeex (36.5%).
Characteristics of hydrocephalus and spina bifida patients from 2011 to 2018 at Edna Adan University Hospital stratified by region of residence and status of delay
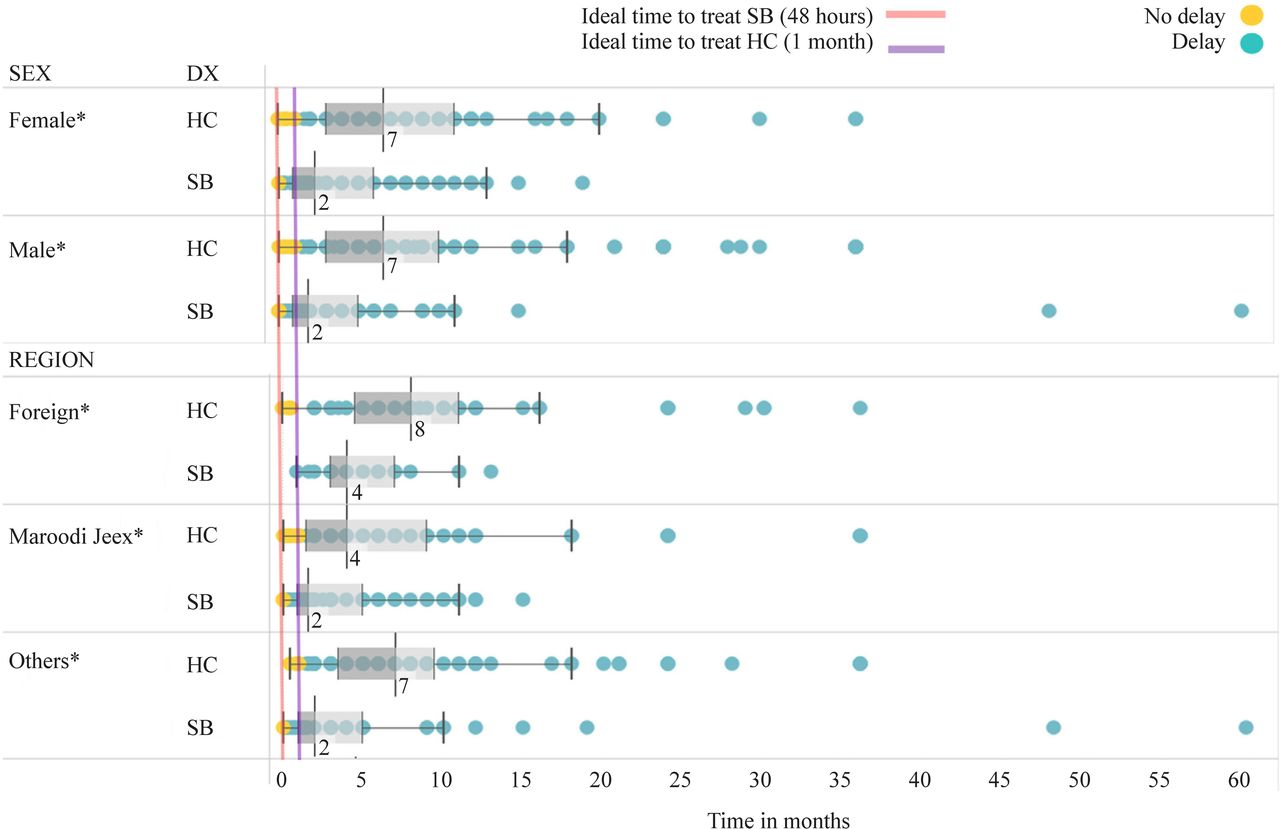
When stratified by sex and region, the median time of access to care reported for either congenital hydrocephalus or spina bifida was markedly delayed beyond the ideal treatment time (figure 1). The longest delay reported among children with spina bifida was 60 months, while the longest delay among children with congenital hydrocephalus was 36 months. Children with either hydrocephalus or spina bifida traveling from foreign countries had the highest waiting time to receive care, with a median delay of 8 months (IQR: 5–11 months) and 4 months (IQR: 3–7 months), respectively. No difference in delay was found between men and women.
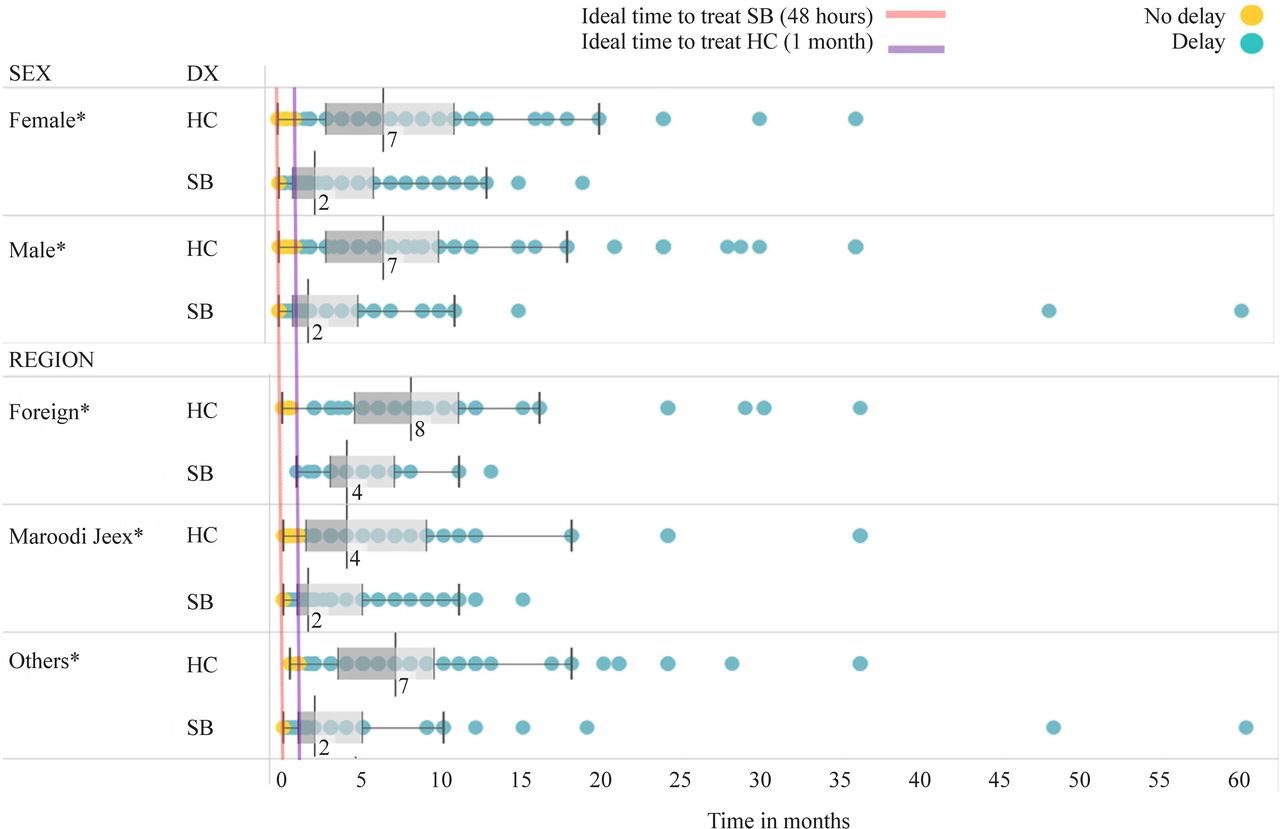
Stratified box plot of status of delay and diagnosis by patient sex and region. Box plots depict descriptive statistics including median, IQR, and outliers. Dots represent status of delay (months). Comparison of delays (median) was performed with Kruskal-Wallis test within the diagnoses stratum. Statistically significant comparisons at p<0.05 are depicted with an asterisk (*). HC, hydrocephalus; SB, spina bifida; DX, diagnosis.
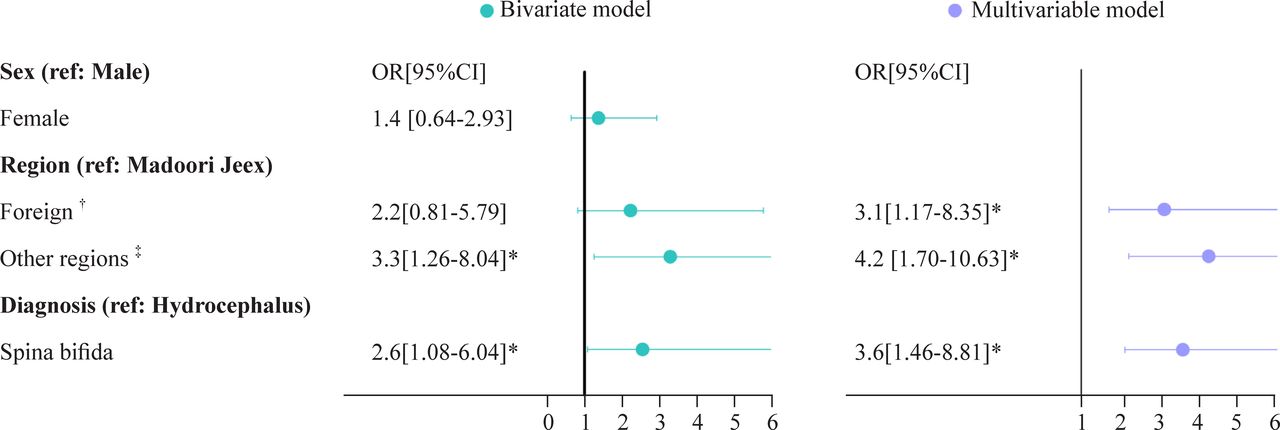
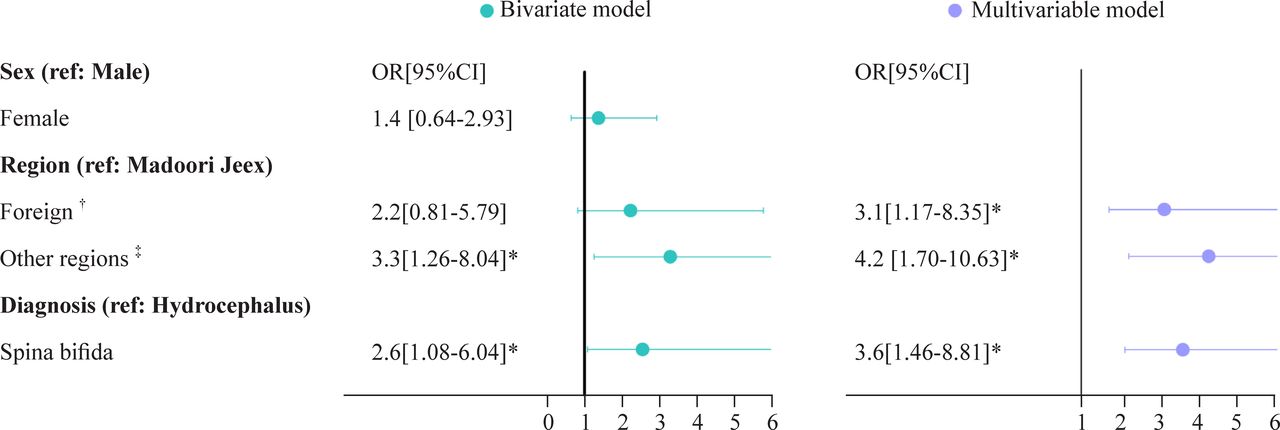
Delays in receiving care were associated with diagnosis and region (figure 2). Children from rural regions of Somaliland and foreign countries were 4.2 and 3.1 times more likely to experience delays in care compared with children living in Madoori Jeex. Children diagnosed with spina bifida were 3.6 times more likely to experience delays in care compared with children with a hydrocephalus diagnosis.
{kind=link}
{kind=link}
Univariate and multivariable logistic regression of likelihood to experience delays in care for patients with neurosurgical conditions (hydrocephalus and spina bifida). *Statistically significant values at p<0.05. †Foreign countries include Somalia, Ethiopia, and Djibouti. ‡Other regions in Somaliland include Sahil, Awdal, Sanaag, Sool, and Togdheer. CI, confidence interval.
Discussion
Neurosurgical care for congenital hydrocephalus and spina bifida remains a major challenge in Somaliland, with significant delays in care in over 90% of the patients with these conditions. Rural residence and spina bifida diagnosis were identified as significant predictors of delayed neurosurgical care. Timely and high-quality surgical intervention is essential for the care of neurosurgical conditions among children in Somaliland. We expect our results to inform next step interventions aimed to scale pediatric neurosurgical care at regional and national levels.
Untreated congenital hydrocephalus and spina bifida can lead to developmental delays, seizures, psychomotor retardation, dementia, gait difficulties, paralysis, incidence of febrile urinary tract infections, vesicoureteral reflux, hydronephrosis, psychological distress, and death.26–29 Delayed care also adds financial burden to families and public healthcare systems.30–32 With over 90% of pediatric neurosurgical patients having significant delays in care, it is no surprise that these children’s families face tremendous financial challenges and are frequently pulled into poverty.33 We identified rural residence and diagnosis of spina bifida as the main predictors for delays in care, similar to other studies in sub-Saharan Africa.6 8 13 34 35 Rural residence might be associated with financial constraints since travel distances and transportation are significant challenges in Somaliland.15 36 Other sources of delay reported in sub-Saharan Africa include misdiagnosis, incorrect management, and financing.36
Other reasons for delays in care frequently reported by caregivers to our team were related to awareness, cultural beliefs, and financial hardship. Families from rural areas of Somaliland often lack knowledge that hydrocephalus and spina bifida conditions can be successfully treated. These conditions are often seen as a death sentence, and many caregivers do not even try to seek treatment for their children. In other cases, families are not aware that treatment for these conditions is fully covered at the EAUH or are unaware that diagnostic capabilities are available during the prenatal period. Out-of-pocket expenses for treatment in other hospitals can range from $800 to $2500, pushing families to look for traditional healers as their first option. These healers burn the heads of children with metal and wood in a series of treatments that can last for several months. After all their resources are spent, families are unable to travel to the hospital in Hargeisa. Children who finally reach the hospital are admitted with significant delays and deteriorated health. Cultural beliefs also play a role in delays in seeking care. Some families hide their sick children because of the stigma around congenital diseases in general. Mothers are often blamed for having a misconduct when their children are born with these types of diseases, putting their families at risk of being cast out from society.
The recommended age of surgery for congenital hydrocephalus and spina bifida in most high-income settings is at 1 month of age and within the first 48 hours of life, respectively. However, hydrocephalus and spina bifida cases at EAUH were markedly delayed in care, with a median delay of 8 and 4 months, respectively. Our previous study identified that children with neurosurgical conditions had one of the greatest burdens of attributable delayed disability-adjusted life years compared with children diagnosed with other congenital anomalies.6 Our result in this multiyear cross-sectional study follows this pattern and depicts a landscape where extreme cases of children with neurosurgical conditions face up to 5 years of delay in treatment.
Timely, affordable, and high-quality access to surgical care remains a significant challenge in many of the world’s lowest income settings.7 Neurosurgical care requires a multidisciplinary team, specialized surgical and anesthesia workforce, special environments, and trained postoperative care.37 The unique needs of pediatric surgical patients increase these challenges. In LMICs, only 6% of neurosurgeons care for 34% of the global population.38 In sub-Saharan Africa, there is only one neurosurgeon per 7 million people, and in East Africa, there is only one neurosurgeon per 9 million people. In Somaliland, surgical systems for children are limited, even more, for children with special neurological needs, with only one pediatric surgeon and a total surgical workforce density of 1.2 per 100000 population.14 39
The way forward
Improving timely access to neurosurgical care for children requires both, policy initiatives and public health interventions. From a policy standpoint, training neurosurgeons and other human resources and expanding the surgical infrastructure for children are fundamental steps in improving access to safe and timely neurosurgical care. This includes including surgical care for children in national health plans and recognizing the importance of children’s surgical care in attaining the United Nation’s Sustainable Development Goals.31 40 41 Telemedicine has been found to be a promising intervention in accelerating neurosurgical diagnosis and patient transfer in other resource constrained contexts.42–44 This intervention may be adaptable to Somaliland, allowing healthcare professionals from rural settings to make remote consultation to enhance diagnosis and timely referral to higher level hospitals. From a public health standpoint, preventive interventions such as folic acid fortification have proven cost-effective in both HICs and LMICs, but many women in LMICs like Somaliland do not seek or don’t have access to this preventive care during the prenatal period. Inadequate financing and outreach programs, lack of awareness among the population and the healthcare workers, cultural beliefs, and misconceptions remain significant barriers to successful micronutrient interventions in Somaliland.45 Further research on behavioral and health systems interventions is needed to effectively approach these specific challenges.
Limitations
Our study offers foundational data to understand the high burden of delays in neurosurgical care for children in Somaliland. However, some limitations warrant discussion. First, the retrospective nature of this study limits our ability to discern causality. Second, this is a hospital-based study at a single center, and it might be prone to selection bias. However, it is important to note that the EAUH is the largest hospital in the country and the primary referral site for delivery of pediatric neurosurgical care for all regions in Somaliland. EAUH also receives a significant number of patients from neighboring countries such as Ethiopia, Djibouti, and Somalia. Finally, we had a significant amount of missing data on postoperative and follow-up outcomes, limiting our understanding of quality of care and important indicators such as mortality rate and case fatality rates. Reporting outcome data is an essential component of surgical monitoring.46 However, the availability of these data is still a limitation, especially in LMICs. Further epidemiological surveillance is needed to fill this gap in knowledge.
Conclusions
We found significant delays in care for pediatric patients with neurosurgical conditions in Somaliland. With a high demand for pediatric neurosurgical care, Somaliland has an urgent need to scale up its surgical system in terms of infrastructure, workforce, referral pathways, and preventive care in order to better satisfy the needs of children with hydrocephalus and spina bifida conditions.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Institutional review board (IRB) approval was granted from Duke University and the Edna University Hospital (EAUH) Review Board.
References
Footnotes
SD and CC-C are joint first authors.
ES and EAI are joint senior authors.
Contributors SD were involved in data collection, study conceptualization, data interpretation, and manuscript writing. CC-C conceptualized the study and were involved in all data analyses and manuscript writing. AG was involved in data analyses and manuscript writing. MM were involved in data collection, study conceptualization, data interpretation, and manuscript writing. HR conceptualized the study and were involved in all data analyses and manuscript writing. ES conceptualized the study and were involved in all data analyses and manuscript writing. EAI were involved in data collection, study conceptualization, data interpretation, and manuscript writing. ES is the guarantor of this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.