Article Text

Abstract
Objective With few studies investigating the effectiveness of telemedicine (TM) in pediatric otolaryngology (ear, nose, and throat; ENT), its role in clinical practice is unclear. The objective of this study was to investigate provider perspectives regarding utility of TM in pediatric ENT practice.
Methods A survey gauging the relative merits of TM visits for common pediatric ENT chief complaints and postoperative visits was distributed to all pediatric ENT providers at a tertiary care, free-standing children’s hospital. Respondents were asked to assess the effectiveness of TM visits compared with in-person visits for completing the following tasks: history collection, physical examination, medical decision-making, and patient counseling.
Results Providers rated TM visits as less useful than in-person visits for completing the most predefined tasks but did identify advantages in history taking via TM for the majority of complaints. Compared with providers with ≥10 years of experience, those with <10 years of experience found TM to be more effective than the in-person appointment for making clinical decisions for patients presenting with recurrent/chronic pharyngitis, neck masses, and stridor/noisy breathing. Opinions regarding the utility of TM for postoperative visits were mixed, with adenoidectomy, tonsillectomy and superficial procedures being most frequently deemed appropriate for TM.
Conclusions The introduction of TM to pediatric ENT faces limitations in detailed examination of areas not accessible without specialized instrumentation. Due to its strength in history taking, results suggest an asynchronous, ‘store and forward’ encounter followed by an in-person physical examination to confirm the diagnosis and treatment plan could be beneficial.
- COVID-19
- Pediatrics
- Otorhinolaryngologic Diseases
- Health Services
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prior to the COVID-19 pandemic, little was known about the utility of telehealth in pediatric ear, nose, and throat (ENT).
WHAT THIS STUDY ADDS
By collating and analyzing the perceptions of pediatric ENT providers, hospital systems can move forward with telehealth by using it in ways that are perceived to be more effective.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Using these data, more centers can compare their perceptions and experience with telehealth and continue to use this method to make healthcare more cost-effective and accessible.
Introduction
Telemedicine is a technology created to assist with the remote care of patients. In 2002, a review of the literature talked about early advancements that allowed telemedicine to be used in pediatric otolaryngology (ear, nose, and throat; ENT).1 At this time, there were still advancements to be made to make telemedicine more practical for widespread use. Prior to the COVID-19 pandemic, research on the use of telemedicine by pediatric specialists was rare and not widely used by ENT providers at our institution.2 In an effort to reduce viral transmission and in response to the changing needs of patients during the COVID-19 pandemic, pediatric healthcare providers turned to telemedicine as a method to provide care for their patients.3–7 This led to a shift in clinic procedures due to larger volumes of clinic visits being done online. While the majority of practice has returned to in-person care, the use of telemedicine in pediatric ENT care delivery during this time has raised awareness for the potential of telemedicine as a part of pediatric ENT practice.
The transition to telemedicine provides added challenges for ENT providers who often use specialized tools to complete a comprehensive examination.3 Despite challenges brought on by an incomplete physical examination, studies have shown that telemedicine can provide benefits for patients presenting for ENT care through decreases in time lost to commute, decreases in lost wages, and decreases in lost school time.8–12 It can also decrease geographic barriers to second opinions, allowing more patients to access specialized care.12 Additional studies have reported few or no missed diagnoses when using telemedicine to evaluate ENT patients, supporting the potential for telemedicine to deliver healthcare for this patient population.9 13 In 2018, Seim and colleagues found that both patient satisfaction and the provider’s ability to diagnose common conditions were comparable between telemedicine and in-person clinic visits.9 While mostly positively perceived, common complaints for patients using telemedicine included technology issues.8 Kokesh and colleagues found that tympanostomy tube placement follow-up can be just as effective in a telemedicine format, indicating a potential use in other postoperative visits.14 The application of telemedicine has also demonstrated utility in other surgical specialties as an effective alternative to in-person postoperative follow-up.15
A study also aimed at assessing the usefulness of telemedicine in pediatric ENT during the pandemic looked at patient satisfaction.16 McCoy and colleagues focused on satisfaction 6 weeks prior to telemedicine utilization and 6 weeks after implementation. This study found that there were problems with satisfaction from caregivers, specifically when surgical intervention was not recommended for patients. This indicates that quality of patient counseling and communication could possibly be hindered in telemedicine formats. Overall, however, the study found that patients were similarly satisfied with telemedicine as they were with in-clinic visits.
The aim of this study was to explore the perspective of ENT providers on their ability to effectively carry out necessary components of an appointment in the context of the recent increase in use in telemedicine. Additionally, we aimed to evaluate whether perspectives on telemedicine varied based on clinician experience during the beginning of the pandemic.
Methods
Study design
We performed a cross-sectional observational cohort study to examine the perspective of ENT providers in using telemedicine to evaluate and treat pediatric patients presenting to an outpatient clinic. Additional interest was given to differences in perspective based on time in practice (<10 years, ≥10 years). Practice was defined as time as an attending physician for surgeons and years of practice in ENT as a nurse practitioner. Age was used to examine potential generational differences between native technology users and non-native users. Years of practice were examined to note the impact of ingrained practice patterns and likelihood of adopting changes in medical practice. The survey was designed by our group to meet the aim of the study and is available for review in online supplemental appendix A. The study was reviewed by our local Institutional Review Board and deemed exempt as the study did not meet the criteria for research on human subjects.
Supplemental material
Survey creation
A survey was created by the authors (KJ and PW) and reviewed by the entire ENT group to measure provider opinions on the utility of telemedicine for multiple chief complaints and in postoperative follow-up for procedures commonly seen in pediatric ENT. For each chief complaint, respondents were asked to assess the effectiveness of using telemedicine visit compared with in-person visit to complete the four tasks related to a typical visit: history, physical examination, medical decision-making, and patient counseling. The first section of the survey focused on chief complaints and how telemedicine was viewed to impact each of the four domains mentioned above. The entire survey was designed such that providers only answered questions related to chief complaints that they had managed with telemedicine visits. On a scale of 0–100, the provider was asked to rate telemedicine effectiveness relative to in-person clinic visits, with 50 being equivalent to in-person clinic visits, 100 being clearly superior to in-person clinic visits and 0 being useless. In addition to rating the effectiveness of telemedicine for each chief complaint, providers were also queried regarding the utility of telemedicine for new patient visits or follow-up visits for each chief complaint. The provider was asked if they would recommend the use of telemedicine going forward for new patients as well as for follow-up visits. A 75% positive response rate was held as a threshold for acceptance of the telemedicine platform. Typical survey response rates can vary widely but are frequently below 50% and the ideal desired response rate with any given survey is 100%. Given the size of our sample, it was determined that as complete a response as possible would be desired, taking into account a subset that would not respond regardless of reminder requests. As such, the mean of the anticipated and desired response rates was used as a reasonably achievable end point.
The second section of the survey asked providers to identify postoperative follow-up appointments following various procedures that would be appropriate for telemedicine. For each procedure, the providers were asked to check a box if they believed that telemedicine could be appropriate for more than 50% of patients who would like to undergo that particular procedure. For example, if a provider had seen patients with recurrent otitis but not hearing loss, they would only answer survey instrument questions related to recurrent otitis media.
Survey distribution
The survey was distributed by email to all advanced practice providers and surgeons within the Department of Pediatric ENT and our institution who care for pediatric patients. This consisted of 11 pediatric otolaryngologists, 1 neurotologist whose practice is 50% based at our institution, and 5 pediatric ENT nurse practitioners. Survey responses were input directly into the Research Electronic Data Capture (REDCap) portal by respondents and housed on a secure network at our institution.17
Data analysis
Counts and frequencies were computed for categorical variables while medians and IQRs were computed for continuous variables. Wilcoxon-Mann-Whitney tests were used to test for differences in provider perception of telehealth usage on chief complaints for each task by years of experience, age range and gender (self-described). Fisher’s exact tests were used to test for association of provider perception of telehealth for each chief complaint by years of experience, age range and gender. Significance for the data was set at p<0.05. All statistical tests were done using the SAS Enterprise V.8.1.
Results
Response rate and participant characteristics
The overall survey response rate was 87.5% and was completed by 91.7% of surgeons and 60% of nurse practitioners who comprised 78.6% and 21.4% of the cohort, respectively. In total, 14 participants completed the survey, among which all had provided telemedicine services to patients presenting with at least one of the predetermined chief complaints. The majority of respondents were male (78.6%, n=11) and most (71.4%, n=10) reported less than 10 years of clinical experience. Demographics of respondents and their telemedicine utilization are outlined in table 1.
Breakdown of demographic factors as well as assessment of telephone and video telehealth visits by years of experience
New referrals
The perceived effectiveness of using telemedicine to complete the predefined components of a clinic visit did not vary based on provider experience for most diagnoses (table 1). Compared with providers with more clinical experience, providers with less than 10 years of experience reported higher perceived levels of effectiveness when using telemedicine to apply clinical decision-making to patients with recurrent/chronic pharyngitis (p=0.0163), a neck mass (p=0.0367), or stridor/noisy breathing (p=0.0368) (table 2, online supplemental table 1).
Supplemental material
Perceived effectiveness on use of telemedicine based on years of experience
Figure 1 outlines the summarized ratings for each complaint based on whether the provider would recommend telemedicine for new or return patients. Overall, providers were supportive of telemedicine as a platform for meaningful patient assessment in most situations (online supplemental table 2). There were no significant differences found for return or new patients based on the provider’s years of experience (online supplemental table 3).

Mean source of all domains among all respondents for each complaint. On a scale of 0–100, the provider was asked to rate telemedicine effectiveness relative to in-person clinic visits, with 50 being equivalent to in-person clinic visits, 100 being clearly superior, and 0 being useless. OSA, obstructive sleep apnea.
History taking
Survey respondents generally rated the telehealth utility of history gathering as equivalent to in-office visits. The median rating for all chief complaints was 50, all with IQR of approximately 50–60 with the exception of hearing loss (IQR 49–50), cerumen impaction (IQR 26.5–50), lip or tongue tie (IQR 32–61), and neonatal swallowing or feeding difficulties not related to tongue or lip tie (IQR 42–50). Chief complaints with IQR higher than 60 consisted of acute otitis media (IQR 50–63), snoring, sleep disordered breathing or obstructive sleep (IQR 50–62), and lip or tongue tie (IQR 32–61) (online supplemental table 2).
Physical examination
Median scores for physical examination fell below 50 for all chief complaints. The lowest rating was observed for chronic otitis media (median=1, IQR 0–7), followed by acute otitis media (median=3, IQR 0–15) and cerumen impaction (median=4.5, IQR 1.5–15.5). The highest ratings for the physical examination were observed for nasal injury or fracture (median=43, IQR 30–50), followed by recurrent or chronic pharyngitis (median=40, IQR 30–50), lip or tongue tie and neck mass (both showing median=36, IQR 30–50) (online supplemental table 2).
Medical decision-making
Median scores for the medical decision-making were more varied among each chief complaint. The highest ratings were observed for recurrent or chronic pharyngitis and neck mass (both showing median=50, IQR 40–50). The lowest ratings were observed for cerumen impaction (median=11, IQR 2–22.5) and hearing loss (median=27.5, IQR 21–40) (online supplemental table 2).
Patient counseling
Median ratings for patient counseling for each chief complaint fell mostly approximately 50 with the exception of cerumen impaction (median=10.5, IQR 8.5–37.5) and neck mass (median=41, IQR 34–50) (online supplemental table 2).
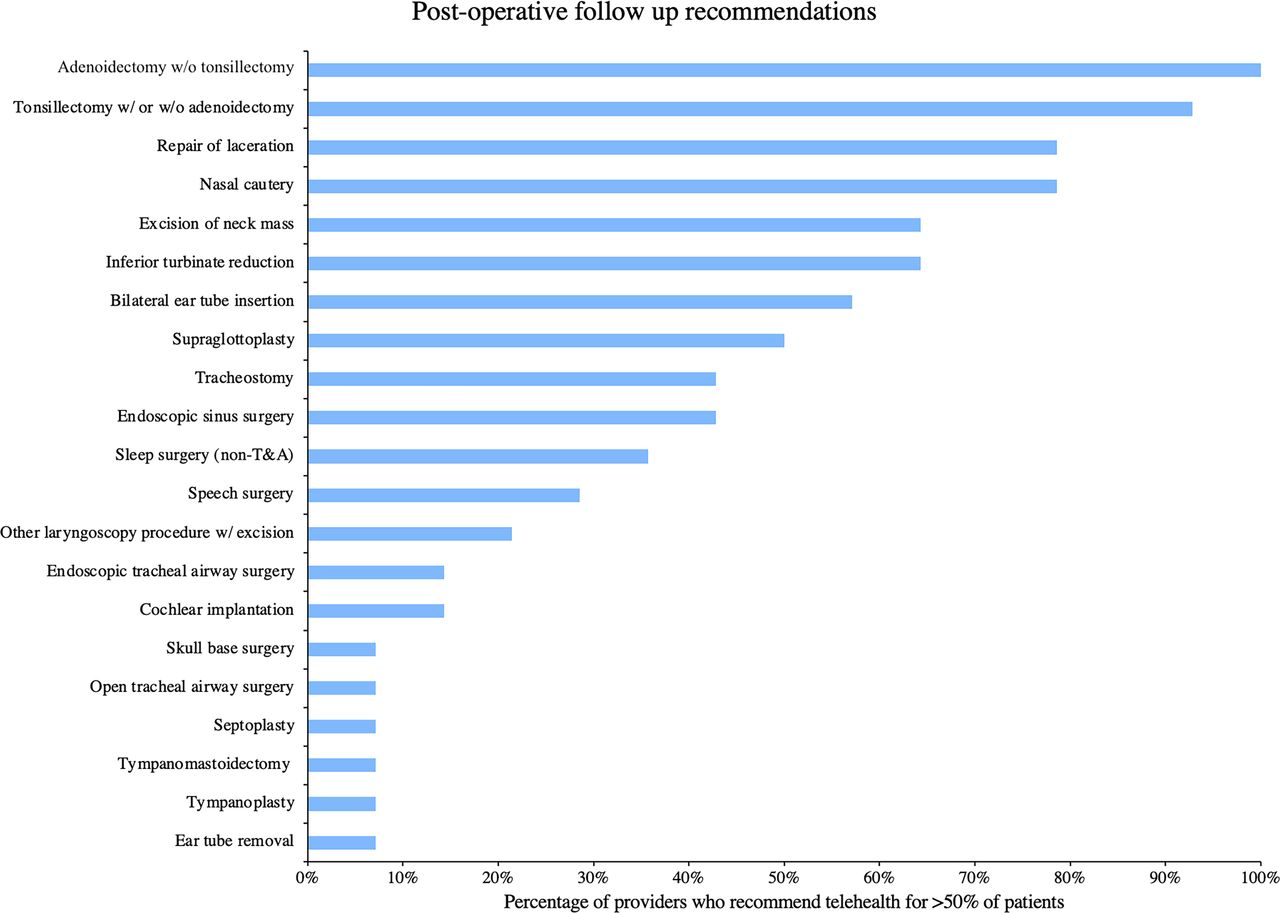
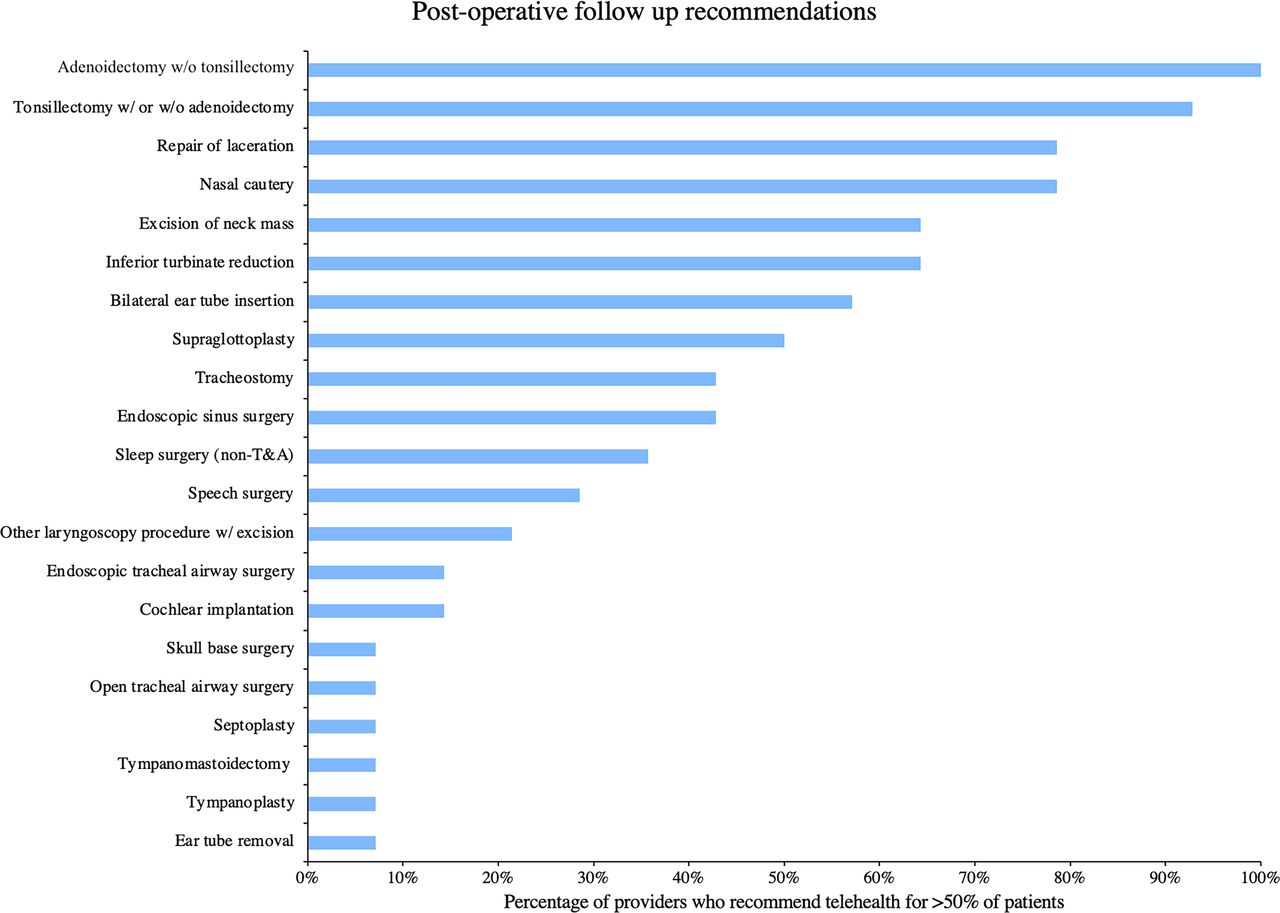
Postoperative follow-up
Respondents were in favor of using telehealth for follow-up visits among most chief complaints. High agreement was seen in complaints related to mouth or throat as well as airway with 100% agreement that telehealth was favorable for follow-up visits for the majority of patients with those conditions (figure 2). Disagreement was observed for nasal complaints, with the largest level of disagreement observed for cerumen impaction (50% in favor, 50% against), nasal congestion (70% in favor, 30% against), and head and neck mass (66.67% in favor, 33.33% against) (online supplemental table 2).
{kind=link}
{kind=link}
Telemedicine postoperative recommendation by intervention. Bars represent the percentage of survey respondents indicating they would use telemedicine for postoperative follow-up for the majority of patients undergoing the indicated intervention. T&A, tonsillectomy and adenoidectomy.
Discussion
The use of telemedicine offers the promise of mitigating barriers to care and minimizing the drawbacks of in-person visits for patients while improving clinic flow and potentially efficiency for providers. While the COVID-19 pandemic has thrust telemedicine into the spotlight, as we return to a system where in-person visits are an option, the application of telemedicine visits to an appropriately selected population will ensure that telemedicine is delivered to patients who will benefit most from this model. The pediatric ENT patient population represents a unique population in whom physical examination of the recesses of the ears, nose, and oropharynx is imperative for accurate diagnosis and management. As such, the current investigation sought to draw on the collective experience of the pediatric ENT providers to help understand which aspects of pediatric ENT are most amenable to telemedicine.
Out of all four of the domains, the physical examination was consistently rated unfavorably compared with the other domains. This is likely due to the lack of physical interaction as well as limitations to what a family member can describe or what can be visualized on the camera. Complaints that rely on general visual examination, such as nasal injuries or fractures, are more suited to a telemedicine physical examination, but these types of complaints are less frequently encountered in pediatric ENT.
The other three domains were generally rated higher, likely because these are carried out very similarly in the clinic as they are in telemedicine. The collection of an accurate history can be obtained over any protected health information virtual platform with equal efficacy compared with in-person visits, as the technology does not present barriers to effective communication between provider and patient apart from potential connectivity issues. While medical decision-making was perceived as less effective via telehealth than in-person visits, the authors suspect that this decrement relates to incomplete data acquisition from impaired physical examination. However, the current instrument was not designed to elucidate this hypothesis. Of note, the known limitations in attainment of a thorough physical examination can also serve to improve history taking as the provider needs a more thorough history in order to make informed decisions. Aside from demonstrating how to administer a medicine on the patients themselves, patient counseling can be done well via telehealth as the provider can communicate and demonstrate on themselves and engage in teach-back by having the caregiver or patient demonstrate back to confirm understanding.
Overall, our findings are consistent with existing literature about the utility of telehealth within surgical specialties.5 15 Our study found positive opinions in general about the effectiveness of postoperative evaluation using videoconferencing software, a finding also seen in the review by Asiri and colleagues examining surgical specialties and Belcher and colleagues with pediatric ENT specifically. Maurrasse and colleagues also found that telemedicine is very well suited to visits where counseling is a large portion of the visit, similar to our findings.3 Also of note, providers believed that patient counseling was similar to in-person visits. It could be of further interest to assess both provider opinions as well as the patient/caregiver opinions of the same visit, as patient satisfaction was affected in telemedicine settings surrounding counseling.16
Some strengths of the survey were the high response rate from providers, including a complete sample of pediatric ENT providers at Nationwide Children’s Hospital as well as the large range of both chief complaints and postoperative follow-up visits included. Another strength is the comparison to in-person clinic. Because telemedicine was sparingly used before hospitals chose to go virtual, providers were able to reflect on recent memory of how visits were conducted in person and compare to the new guidelines using telemedicine.
Some limitations of the current investigation include the small sample size of participants, the opinion-based nature of the survey, and the limited telemedicine knowledge of the providers given the novelty of the platform. Participants were also selected by convenience as opposed to random selection, although this would have significantly decreased the sample size at our institution. By expanding this kind of investigation to other sites, a more significant data set could be collected to draw broader conclusions. Additionally, the limited size of the population surveyed leads to limited statistical significance. Despite these limitations, the results of the current investigation provide an overview of how telemedicine can be used in pediatric ENT in the future.
In conclusion, while many telemedicine visits in pediatric ENT are hindered by limitations in physical examination, the majority of providers favorably rated the use of telemedicine in certain aspects of practice. Implementation of telemedicine practices that focus on increasing the yield of both telemedicine and in-person encounters can lower patient travel and time burdens and improve the allocation of telemedicine and in-clinic time to optimize efficiency in pediatric ENT practices. Should further assessment of telemedicine utility in pediatric ENT continue to demonstrate poor utility of telemedicine for physical examination, one potential avenue could be implemented using telemedicine’s strengths in history taking to decrease office visit time and to improve clinic flow by taking history through telemedicine before the visit so the time allotted can be used for physical examination and patient counseling.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
IRB review deemed approval not necessary for this study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CG and PW contributed to study conception and design, acquisition of data, analysis and Interpretation of data and drafting of Manuscript. KJ contributed to acquisition of data and drafting of Manuscript. TB contributed to analysis and Interpretation of data. GM contributed to drafting of Manuscript. PW fullfills the role of the guarantor. All the authors contributed to critical revision and final approval of the manuscript.
Funding Funding for this project was supported by The Ohio State University College of Medicine Roessler Medical Student Research Scholarship.
Competing interests There are no competing interests to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.