Article Text

Abstract
Background Congenital diaphragmatic hernia (CDH) is a cause of significant morbidity. CDH is the most common neonatal diagnosis requiring extracorporeal membrane oxygenation (ECMO).
Methods We compared the different characteristics of ECMO and non-ECMO patients with CDH in a case-control study. Data were extracted from the Kids’ Inpatient Database. Records from 2006 to 2016 were used. Patients <28 days of age were selected. CDH infants (n=9217) were stratified based on whether they were treated with ECMO (n=348) or not (n=8869). Demographic data and hospital characteristics were collected. Categorical variables were analyzed using χ2 tests to determine associations between the ECMO-treated and non-ECMO-treated infants on demographic and clinical characteristics. Differences in hospitalization costs were analyzed using t-test. Multivariable logistic regression analyses were stratified by clinical and demographic characteristics to identify factors associated with ECMO. Significant variables were included in the model to determine predictors for ECMO.
Results The proportion of infants treated with ECMO was higher in White infants, and lower in Hispanics. The cost of hospitalization was higher with ECMO (p<0.0001). ECMO patients were more likely to be treated in their birth hospital (p<0.001), at an urban location (p<0.001) and more likely to have private insurance (p=0.011). After adjusting for confounders, odds of ECMO treatment remained lower in Hispanics (p=0.001) and self-payers (p=0.004).
Conclusion There was a decrease in the proportion of CDH infants needing ECMO use in the USA from 2006 to 2016. Disparities exist in ECMO use and mortality between different ethnic groups and regions of the USA.
- neonatology
- congenital abnormalities
- extracorporeal membrane oxygenation
- mortality
- health care costs
Data availability statement
Data are available in a public, open access repository. https://www.hcup-us.ahrq.gov/db/nation/kid/kiddbdocumentation.jsp (accessed 8 February 2022).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Congenital diaphragmatic hernia (CDH) is the most common neonatal diagnosis requiring extracorporeal membrane oxygenation (ECMO).
CDH has the lowest survival rate compared with other conditions requiring neonatal ECMO.
Both CDH and ECMO have many associated morbidities and high risk of mortality.
What this study adds
The proportion of infants with CDH requiring ECMO has decreased from 2006 to 2016.
During this period, the proportion of ECMO utilization for CDH was lowest among patients of Hispanic ethnicity and highest among patients identified as White.
The difference between the average cost of hospitalization between patients with CDH requiring ECMO and those not requiring it was US$623 748.
How this study might affect research, practice and/or policy
These updated data on ECMO utilization may aid in counseling parents of infants of CDH.
Our study provides newer data on regional differences in CDH patient outcomes in the USA.
Introduction
Congenital diaphragmatic hernia (CDH) complicates 2.61–3.19 per 10 000 live births.1 2 It is an uncommon congenital defect of the diaphragm that is associated with abnormal lung development, which is characterized by pulmonary hypoplasia and altered function of the pulmonary vasculature. As a result, persistent pulmonary hypertension of the newborn (PPHN) is a frequent complication of CDH.
Extracorporeal membrane oxygenation (ECMO) is a stronghold of rescue support for neonates with severe PPHN.3 The main purpose of ECMO in critically ill newborns with CDH is to bridge them to later definitive surgical repair.4 ECMO is a highly invasive therapy that requires specialized care provided by neonatal ECMO centers. CDH is the most common neonatal diagnosis requiring extracorporeal life support (32% of all neonatal ECMO cases).5 At the same time, CDH has the lowest survival rate compared with other conditions requiring neonatal ECMO.5 Moreover, the Extracorporeal Life Support Organization (ELSO) reported in 2012 that the survival of neonates with CDH decreased from 53.4% to 45.4% from 1990 to 2011.6 The 2016 ELSO registry report showed an improved survival rate of 50%, which is still below that of the last decade of the 20th century.5
Besides the high mortality rates associated with ECMO, it also carries an increased risk for morbidities, such as poorer neurodevelopmental outcomes,7–9 hearing loss,7 hemorrhagic and thrombotic complications,10 sacrifice of a common carotid artery,11 renal impairment,12 infections13 and growth failure.14 Given such burden, it is essential to understand national trends in ECMO use, to understand costs and to reevaluate the risk factors for ECMO use in neonates with CDH.
This study aimed to determine the trends of ECMO use in neonates with CDH among different census regions of the USA and over time, and to determine the risk factors for neonatal CDH requiring ECMO. We tested the hypothesis that the proportion of neonatal ECMO cases among infants with CDH has decreased in recent decades.
Methods
Study design
Data were extracted from a retrospective cohort database, the ‘Healthcare Cost and Utilization Project Kids’ Inpatient Database (KID)’ sponsored by the Agency for Healthcare Research and Quality.15 This database uses public and private statewide data organizations to collect hospital discharge records every 3–4 years.
The KID uses systematic random sampling to select 10% of all reported uncomplicated in-hospital births and 80% of all reported complicated in-hospital births from approximately 4000 short-term non-federal, general and specialty hospitals in 38 participating US states as of 2006 (increased to 47 by the year 2016). We analyzed data from 2006 to 2016. In 2016, there were total of 4200 hospitals participating. Among them, there were 73 freestanding children’s hospitals.
Study population
Hospitalization records for infants <28 days old with an International Classification of Diseases (ICD) diagnosis code for CDH (ICD, 9th Revision, Clinical Modification (ICD-9-CM) codes 756.6 or V13.67, or ICD, 10th Revision, CM (ICD-10-CM) codes Q79 or Z87.738) listed as any 1 of the 15 diagnoses on the discharge record were selected for inclusion. Only the patients <28 days of age on admission were included in order to select for initial postnatal hospitalizations. Afterwards, those infants who were transferred to another institution were excluded to eliminate double counting of infants who were born at one institution and then transferred out for a higher level of care. Infants with CDH then were classified based on whether they were treated with extracorporeal membrane oxygenation (ICD-9-CM codes 39.65 or V15.87, or ICD-10-CM codes 5A15223 or Z92.8) or not. Patient demographics, such as year of birth, birth weight category, gender, race/ethnicity, payer type and mortality, were collected as categorical variables. ‘In-hospital birth’ was defined as infants receiving ECMO care in the same hospital as where the neonate was born, as opposed to infants who were transferred after birth for higher level of care. The total cost of initial neonatal intensive care unit (NICU) hospitalization was included as a linear variable. Hospital characteristics included hospital US census region (Northeast, Midwest, South or West)16 (figure 1), hospital location (urban vs rural), teaching or non-teaching status and bed size. The urban/rural designation was determined by the Core Based Statistical Area (CBSA).17 Hospitals residing in counties with a CBSA type of ‘metropolitan’ were considered urban, whereas hospitals with a CBSA type of ‘micropolitan’ or non-core were classified as rural. A hospital is considered a teaching hospital if it has one or more Accreditation Council for Graduate Medical Education-approved residency programs, is a member of the Council of Teaching Hospitals18 or has a ratio of full-time equivalent interns and residents to beds of 0.25 or higher. Bedsize categories are based on the number of hospital beds and are specific to the hospital’s location and teaching status. Bedsize assesses the number of short-term acute care beds set up and staffed in a hospital. Hospital information was obtained from the American Hospital Association Annual Survey of Hospitals.19 We collected information on the clinical risk factor of pneumothorax. (ICD-9-CM 512.81 or ICD-10-CM J93.9). Due to data use retractions or incompleteness of hospitalization records, some variables had missing information.
Kids’ Inpatient Database states, by the US Census Bureau regions. Source: https://www.hcup-us.ahrq.gov/db/nation/kid/KID_2019_Introduction.pdf (accessed 24 February 2022).
Data analysis
Categorical variables were analyzed using χ2 testing to determine associations between the ECMO-treated and non-ECMO-treated CDH infants with the considered demographic and clinical characteristics. Differences in the cost of NICU hospitalization were analyzed using t-tests. Multivariable logistic regression analyses were stratified by clinical and demographic characteristics to identify factors associated with ECMO treatment. All significant independent variables were included in the multivariable model to determine predictors for ECMO treatment. A final multivariable regression model for ECMO treatment as a separate outcome was adjusted for race, in-hospital birth (vs transferred in), hospital region, insurance type, history of pneumothorax and survivorship. Missing values were not included in the analyses. All analyses were performed with a type I error of p<0.05, using Stata/SE V.14.2 (StataCorp, College Station, Texas, USA).
Results
Demographic characteristics for infants diagnosed with CDH
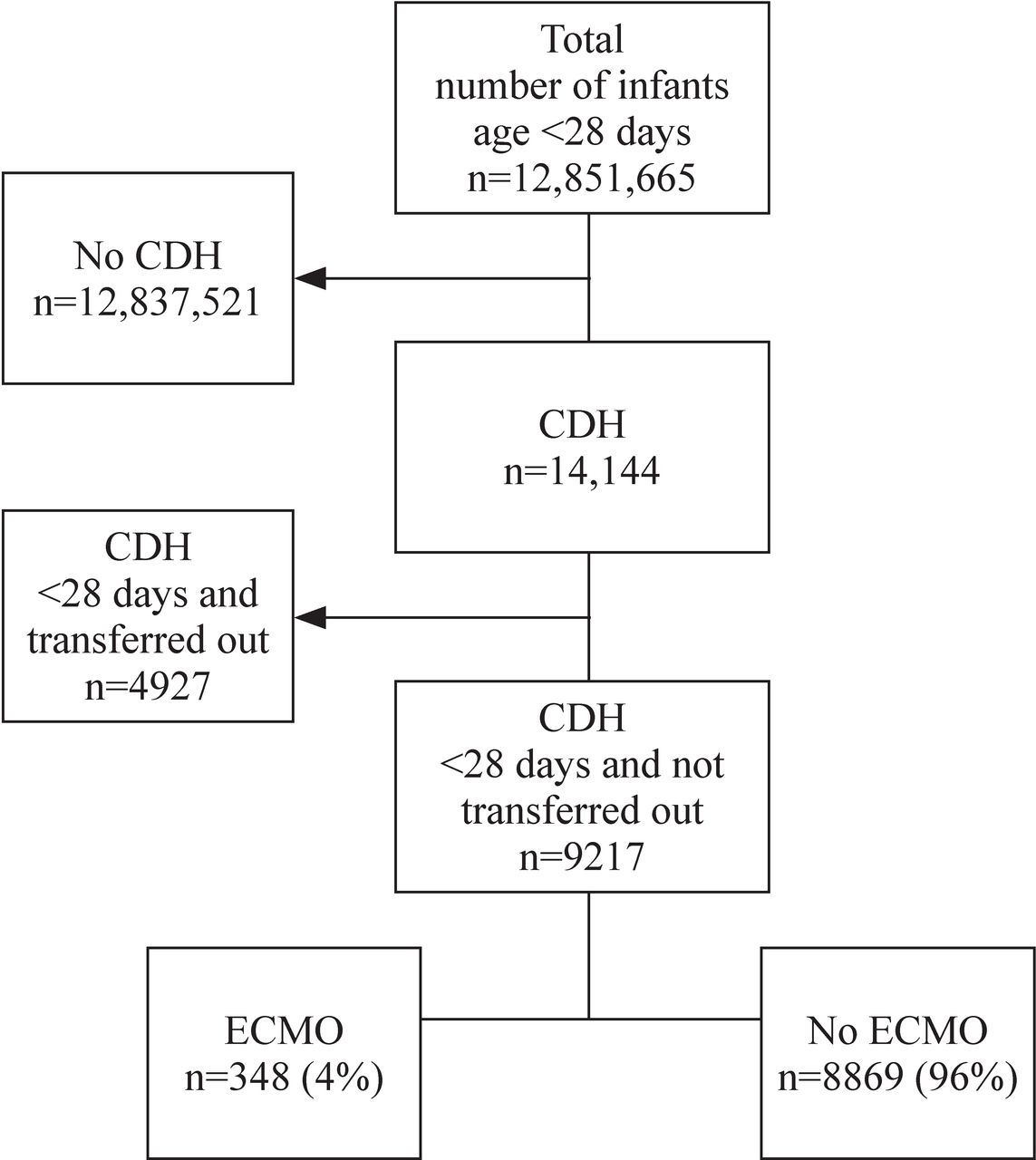
From 2006 to 2016, there were 9217 infants with a diagnosis of CDH identified among infants <28 days of age who were not transferred to another hospital for higher level of care (figure 2). Among all infants with a diagnosis of CDH in the study population, 51.1% of infants were White, 11.2% were Black, 26.2% were Hispanic and 11.5% were of other races; 57.1% of infants were female and 42.9% were male. The most common insurance type was government-issued insurance (52.3%). Most infants with CDH were hospitalized at their birth hospitals, which in this cohort was typically a large teaching facility located in an urban setting (table 1).
Characteristics of study infants

Flow chart of the study population. CDH, congenital diaphragmatic hernia; ECMO, extracorporeal membrane oxygenation.
Regions and years
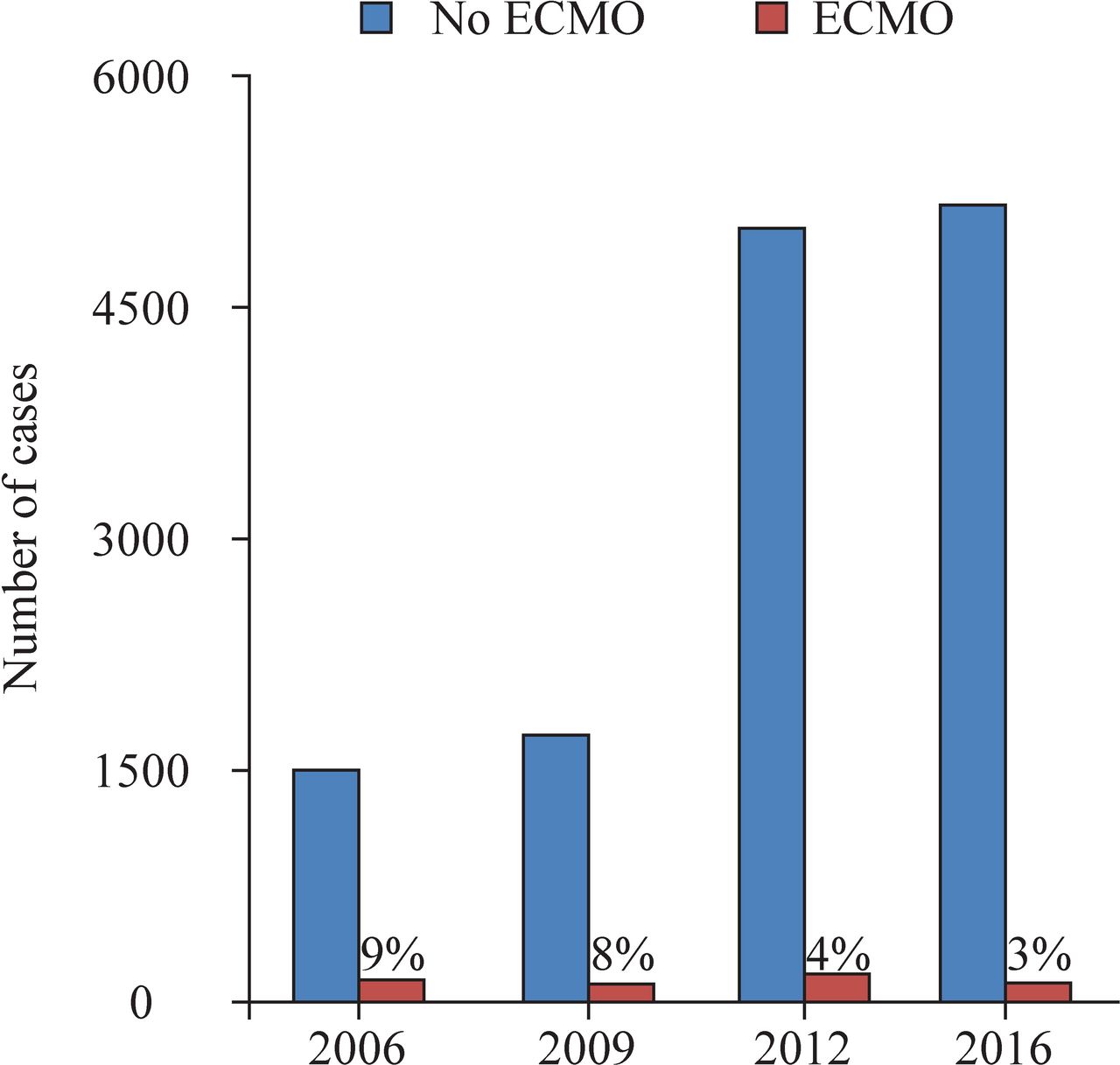
The increased number of CDH diagnoses in 2012 is reflective of the inclusion of 22 additional US states in the database. Despite this increase, the proportion of infants with CDH who were treated with ECMO decreased from 9% in 2006 to 3% in 2016 (figure 3). In this cohort, 13.8% of infants with CDH were cared for in the Northeast, 26.1% in the Midwest, 29.5% in the South and 30.6% in the West region of the USA. The proportion of infants treated with ECMO was significantly higher in the South (p<0.001) (table 1, figure 4). The mortality rate was also significantly higher in the South (p<0.001) (table 1).

Per cent of extracorporeal membrane oxygenation (ECMO) use for congenital diaphragmatic hernia (CDH) decreased from 2006 to 2016.
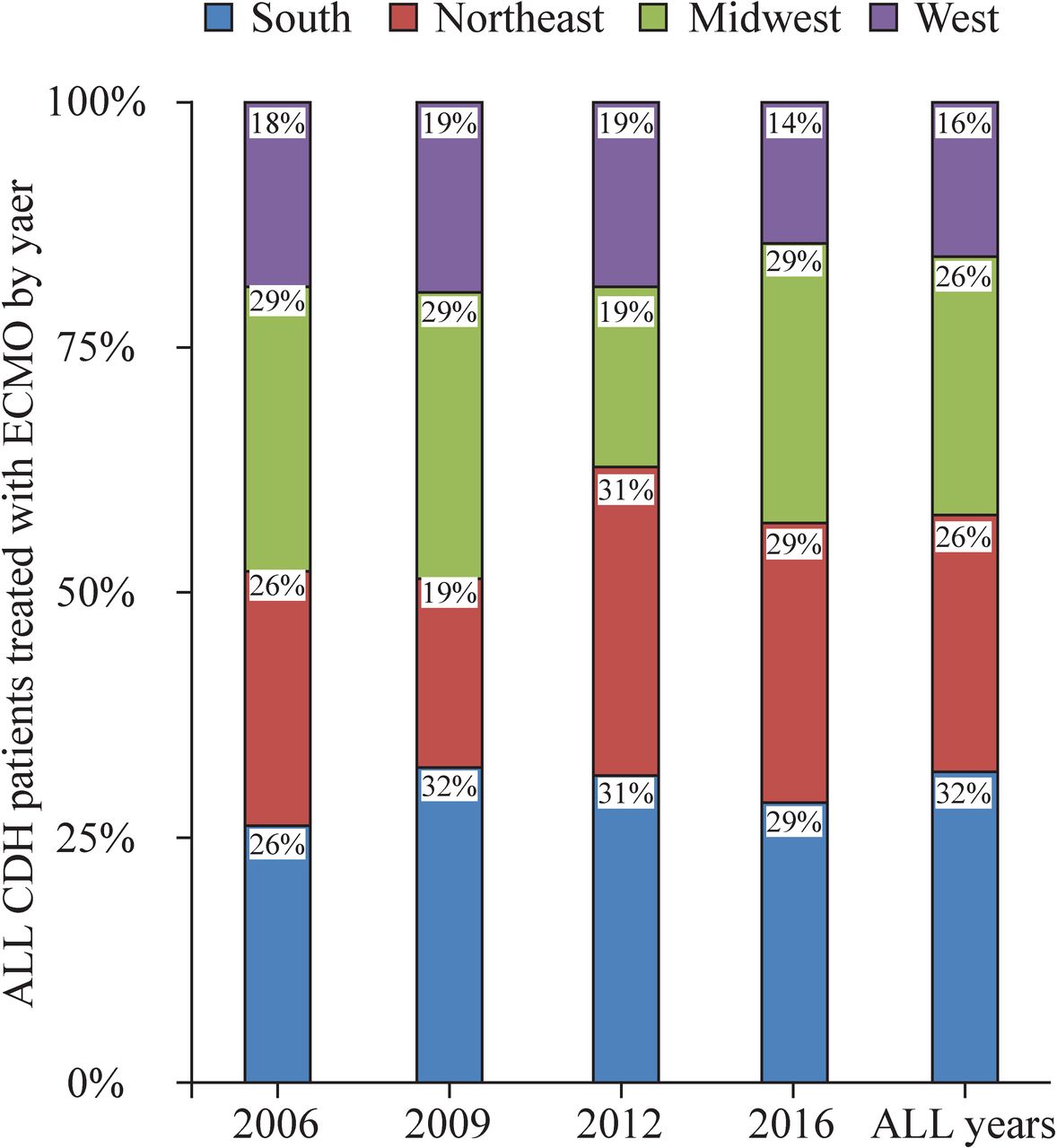
Proportion of extracorporeal membrane oxygenation (ECMO) use for congenital diaphragmatic hernia (CDH) by the US Census Bureau regions (2006–2016).
Extracorporeal membrane oxygenation
In the entire cohort, only 4% of infants with CDH required ECMO treatment (figure 2). The average cost of NICU hospitalization was significantly higher with ECMO use (US$718 210, 95% CI 635 411 to 801 010 vs US$94 462, 95% CI 89 524 to 99 401; p<0.0001; figure 5). The proportion of infants with CDH treated with ECMO was significantly higher in White infants and lower in Hispanic infants (p=0.002) (table 1). Other characteristics associated with ECMO treatment included in-hospital birth (vs transferred in) (p<0.001), urban location (p<0.001), private insurance (p=0.011), history of pneumothorax (p<0.001) and survivorship (p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cost of initial neonatal intensive care unit (NICU) hospitalization of infants with congenital diaphragmatic hernia (CDH). ECMO, extracorporeal membrane oxygenation.
After adjusting for confounders (race, in-hospital birth status, region, insurance, presence of pneumothorax and survivorship), the odds of receiving ECMO treatment remained significantly lower in Hispanic infants (OR 0.6; 95% CI 0.5 to 0.8; p=0.001) and self-payers (OR 0.3; 95% CI 0.1 to 0.7; p=0.004) (table 2). Clinically, the odds of treating with ECMO remained significantly higher in infants identified to have a pneumothorax (OR 4.0; 95% CI 2.3 to 7.2; p<0.001).
Risk factors for ECMO use among CDH infants (multivariable analysis)
Mortality
The overall mortality rate among infants with CDH was 5.1%. The mortality rate increased to 43.6% for infants requiring treatment with ECMO (table 1). Rates of death were significantly higher in CDH infants born in the South region of the USA (p<0.001). The lowest mortality rate was seen in the Northeast region of the USA (p<0.001) (table 3).
Survivors and non-survivors by US census regions
Discussion
We conducted a retrospective study to investigate the risk factors for ECMO among the infants with CDH and to determine the regional and healthcare cost differences in infants with CDH. The number of infants reported having CDH increased from 2006 to 2016 in this database, while the number of those CDH infants requiring ECMO remained relatively constant, overall leading to a decreasing proportion of infants with CDH who required ECMO. Similarly, Morini et al reported a decrease in the use of ECMO in CDH infants during the years 2007–2013 when compared with the previous decade.20 This downward trend in ECMO utilization may be attributed to the development and implementation of improved postnatal medical management. Such improvements include, but are not limited to, broader use of inhaled nitric oxide, sildenafil, prenatal steroids as well as the gentler ventilation strategies.20–22 Furthermore, the increasing implementation of standardized, risk-adjusted management protocols may have impacted the outcomes of infants with CDH.23 24 Advancements in prenatal diagnostic evaluations, such as lung-to-head ratio (LHR) and observed-to-expected total lung volume (o/e TLV), also may have lowered ECMO utilization in the neonatal CDH population. Advancements in fetal diagnosis and assessment of lung volumes by ultrasound and fetal MRI in CDH infants allows for improved prepartum and peripartum planning, such as an arrangement of delivery at a tertiary or quaternary center, and for better preparation of healthcare teams and resource mobilization.25–28
In our study, utilization of ECMO in CDH infants was significantly different between racial groups, inborn versus outborn status, hospital type and hospital region. The highest proportion of ECMO use was noted in infants categorized as Black or ‘other’ race, those infants who were inborn, those treated in urban teaching hospitals and in the Northeast. Our study found a lower proportion of ECMO utilization for CDH among Hispanics and a higher proportion among the patients of White race. The opposite was reported in a study by Oyetunji et al.29 That study examined the older data from a smaller sample (n=827) and only from a single center. Our cohort also had a higher proportion of Hispanic patients (26.2% vs 8.2%). The KID database study by Sola et al of CDH infants at <8 days of age for 10 years before 2006 identified Black and other non-Hispanic minorities to have the highest mortality rates. One decade later, our observations in the CDH infants requiring ECMO remain unchanged.30
As expected, a higher proportion of CDH infants requiring ECMO treatment was seen in the urban teaching hospital setting. The missions of teaching hospitals differ from non-teaching institutions. Furthermore, financial considerations differ between these groups of healthcare institutions. Rural hospitals are typically smaller in size and provide fewer specialty services. Accordingly, urban teaching hospitals serve as referral centers for high-risk newborns who need higher levels of care and/or specialty care, including those with the diagnosis of CDH. More ECMO in the inborn population in these hospitals likely indicates the high prevalence of prenatal identification of CDH and appropriate referral to specialized centers. On the other hand, we did not find that hospital bed size is significantly associated with ECMO use for CDH. In addition, there might be considerable differences in practice patterns, patient mix, illness severity and services available between freestanding children’s and other hospitals.15
A previous study by Cameron et al identified neonatal CDH as the pediatric surgical condition with the highest cost burden.31 ECMO use has previously been reported to be the largest contributing factor to the economic burden in CDH care.32 In our cohort, infants who were subject to ECMO had more than a sevenfold increase in the average cost of hospitalization compared with infants who did not receive ECMO. The increased cost in the ECMO group is attributed to the complexity of performing the ECMO which includes the use of advanced medical equipment, the need for more procedures, medications and increased staffing. Interestingly, higher odds of receiving ECMO in privately insured infants have not previously been reported to the best of our knowledge. Previous studies that used earlier data from the KID database had inconsistent conclusions regarding the association of private insurance and higher survival in CDH infants.30 33
We report variability in the proportion of ECMO use for CDH infants in different census regions of the USA. In particular, infants cared for in the South had the highest risk of requiring ECMO. To our knowledge, this inconsistency between different regions has not previously been reported.
In our cohort, ECMO infants were more likely to have had a pneumothorax which is likely related to the severity of the disease itself. The presence of pneumothoraces inherently increases the severity of the patients’ overall condition. More severe CDH leads to more significant pulmonary hypoplasia, which in turn increases the risk of postnatal pneumothorax. Similarly, Usui et al reported a significant increase in mortality when pneumothorax was associated with >25% diaphragmatic defect, as reported by the surgeon intraoperatively.34
The limitations of our study include the retrospective nature and the reliance on the KID database, whose composition will affect our results and the degree to which our findings are generalizable. Moreover, the KID database information is composed of ICD data, and thus is susceptible to the inherent variability of coding practices across different institutions as well as coding errors. Because it largely focused on administrative data, the KID database lacks clinical features specific to the diagnosis of CDH and ECMO, limiting our ability to query this database for other potentially clinically relevant questions. For example, ICD codes for CDH do not account for disease severity. Factors such as the liver position and lung-to-head ratio are not available in the KID database. Also, there is no record of the diagnosis timing (prenatal vs postnatal). Generally, prenatally diagnosed CDH tends to be more severe than cases of postnatally diagnosed CDH; information regarding timing of diagnosis may have lent insight into the severity of cases both for risk stratification as well as for more insight into the cohort described by the KID. Moreover, the study period included the moment of transition from ICD-9 to ICD-10. The study population in the KID had lower ECMO rates than some other cohorts reported worldwide, and so the generalizability of our study findings may be limited to neonates with less severe CDH.35
In conclusion, there has been a decrease in the proportion of CDH infants that needed ECMO use in the USA from 2006 to 2016. This reduction in ECMO use can possibly be attributed to better patient selection by way of prenatal diagnosis and evaluation as well as novel postnatal care strategies. A disparity exists in ECMO use and mortality between different ethnic groups and different regions of the USA. Investigation into the underlying reasons for such variations in ECMO use is essential to make a positive impact on management and outcome of neonates with CDH. The findings in this study regarding the regional differences in ECMO use and mortality can lead to more targeted efforts to further investigate and address the reasons for these differences with the goal in mind of eliminating these disparities in care and overall reducing the burden of need for ECMO and mortality in CDH infants.
Data availability statement
Data are available in a public, open access repository. https://www.hcup-us.ahrq.gov/db/nation/kid/kiddbdocumentation.jsp (accessed 8 February 2022).
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Institutional Review Board of the University of California Los Angeles. The need for informed consent was waived due to the anonymity of the research data.
References
Footnotes
Contributors AK conceived of the presented idea. CL performed the statistical analyses. MG and HJ contributed to the design and implementation of the research and aided in interpreting the results. AK and CL wrote the manuscript with input from all authors. AK designed the figures. CL designed the tables. AC supervised this project, provided critical feedback and helped shape the research, analysis and manuscript. AK is responsible for the overall content as guarantor. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.