Article Text

Abstract
Background We aim to describe a modified Dega osteotomy technique in detail, emphasizing its eventual advantages in comparison to the original Dega osteotomy and ‘San Diego’ modification. We also present our related literature review on various osteotomy techniques.
Methods We reviewed the radiological indices of 27 dysplastic hips in 25 children with cerebral palsy and developmental dislocation of the hips (9 boys, 16 girls; mean age, 5 years) who underwent a modified Dega osteotomy according to Paley.
Results Comparing the radiological indices results between our patients and those reported by the various authors in the literature, the data are almost identical.
Conclusions The modified Dega osteotomy is the only technique wherein all two limbs of the triradiate cartilage are true, which becomes a single hinge where the osteotomy turns. Despite the similar results in the radiological indices between our patients and those in the literature, we still consider that the entire triradiate cartilage is a better hinge point for the iliac osteotomy. The difference between the osteotomy adopted in our institution and the modality described by most authors in the literature is that the latter mostly ignore or miss the ischial limb of the triradiate cartilage.
- bone diseases
- orthopedics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Many different types of acetabular osteotomies to treat dysplasia have been published over the years.
The classical Dega osteotomy, like the Pemberton, belongs to a group of osteotomies which are periacetabular.
Different modifications of the classical Dega osteotomy are described in the literature, the ‘San Diego’ type is one of the well-known.
The new findings in our technique
We present a new periacetabular osteotomy, different from the classical Dega, the Pemberton or the ‘San Diego’.
The osteotomy is hinging on the triradiate cartilage, never penetrating the iliac medial wall.
Our literature research discovers that most authors elect for either the classical Dega osteotomy or the ‘San Diego’ type.
Impact on clinical practice in the foreseeable future
Since the osteotomy is hinging on the soft triradiate cartilage, the outer iliac table is easily turned down, allowing an achievement of a good acetabular coverage.
The fact that the acetabulum is freed only through the outer cortical iliac bone and intervening cancellous bone, makes this periacetabular osteotomy more stable.
Introduction
The well-known Pemberton and Dega osteotomy techniques are constantly being reshaped and modified to establish the optimal treatment method of dysplastic hips in children. The Pemberton osteotomy is probably hinged at the triradiate cartilage, but theoretically, it may also be hinged at the symphysis pubis.1–3 The Pembersal osteotomy, as described by Perlik et al,4 is similar to the Pemberton osteotomy, which theoretically hinges at the triradiate cartilage, symphysis pubis and ischial osteotomy site.
Dega’s initial osteotomy was first briefly mentioned in a 1964 German publication.5 However, it was not until 1969, in a Polish publication,6 that the initial osteotomy was referred to as a supra-acetabular, semicircular or an incomplete transiliac osteotomy. The theoretical location of the hinge of the osteotomy can involve, to varying degrees, the sciatic notch, the posterior portion of the inner pelvic cortex, the horizontal limb of the triradiate cartilage and the symphysis pubis (figure 1).
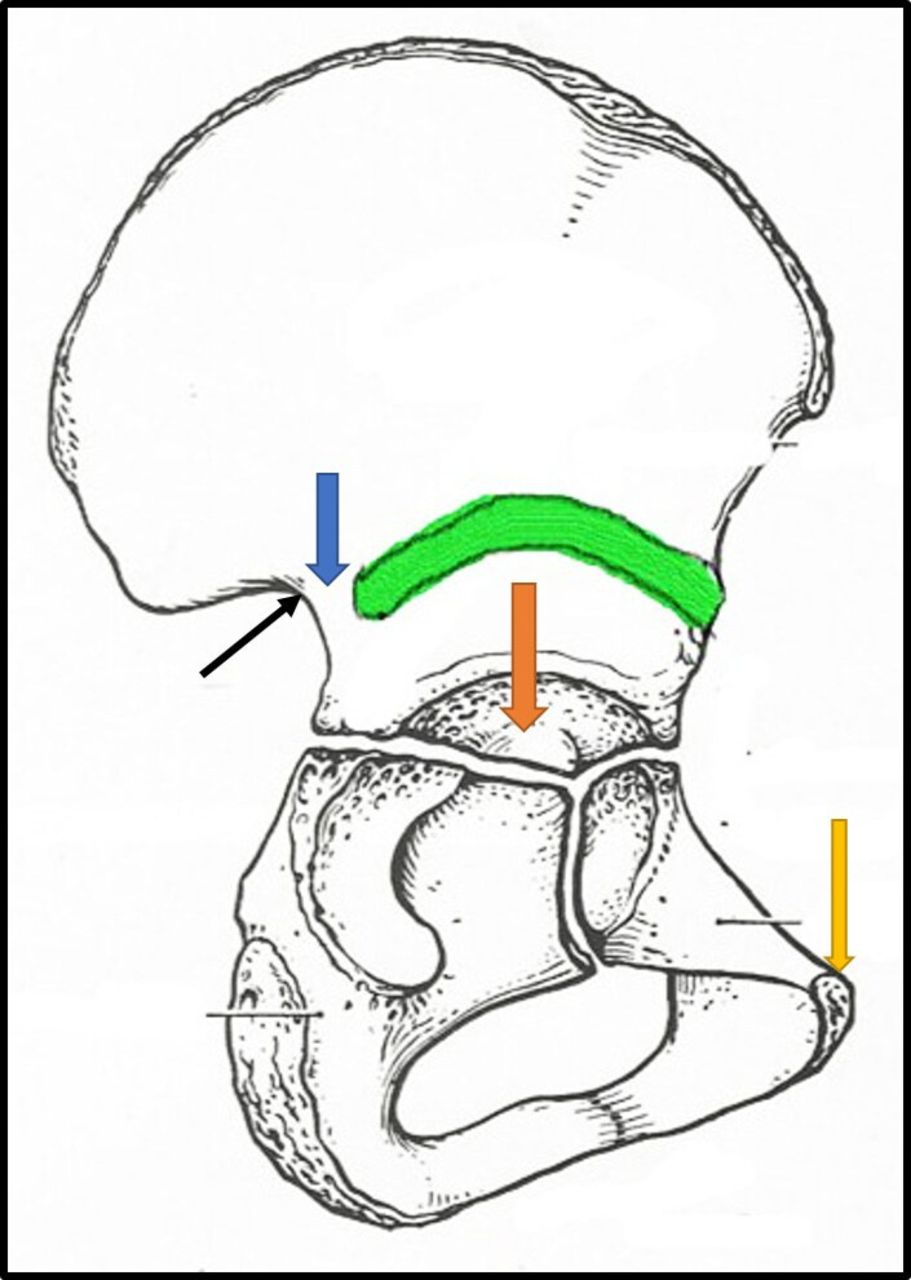
The classic Dega osteotomy (black arrow—the sciatic notch, blue arrow—the posterior portion of the inner pelvic cortex, orange arrow—the horizontal limb of the triradiate cartilage, yellow arrow—the symphysis pubis). (Illustration by the senior author Noam Bor).
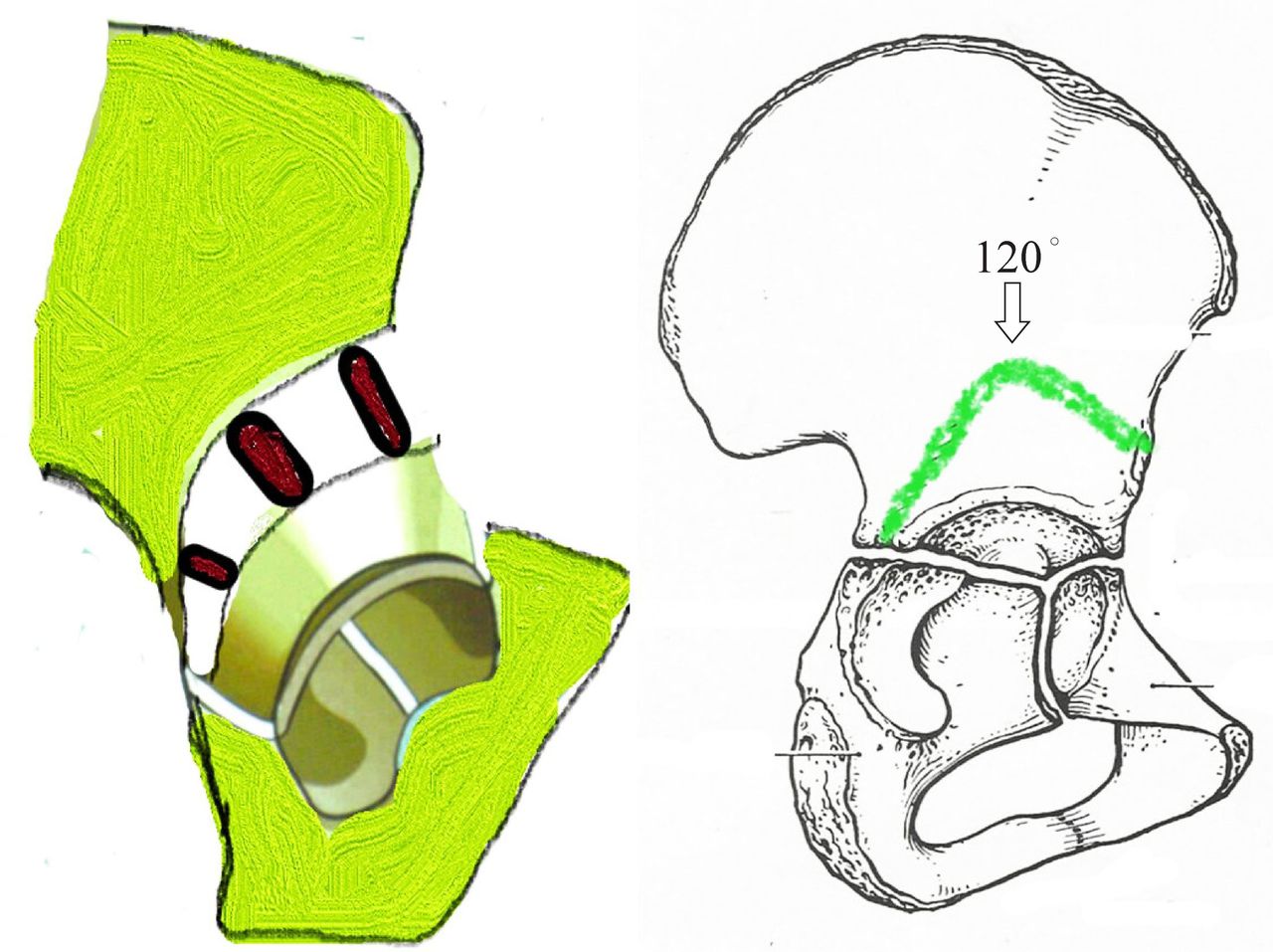
To make the osteotomy more applicable to spastic dislocated hips, Mubarak et al7 introduced their modified Dega’s osteotomy, also called ‘San Diego’, in 1992.7 The osteotomy is bicortical at the posterior and anterior corners (the sciatic notch and the anterior inferior iliac spine) of the iliac bone, and unicortical in between, extending down and hinging on the remaining triradiate cartilage, virtually missing the ischial segment of the cartilage (figure 2). Paley first mentioned his modification to the Dega osteotomy in a publication from 1998, although referring to it as a Dega osteotomy8; however, he further elaborated and rectified on this method with specific mention of the ischial extension, the ‘Dega-Paley osteotomy’, with illustrations in a book chapter published in 2007,9 and as a ‘Paley osteotomy’ in more recent publications.10 11 In 2005, Roposch and Wedge12 described their modified Dega’s osteotomy (the ‘Wedge osteotomy’), where the line of the osteotomy was directed toward the two rami of the triradiate cartilage, ilium/ischium and ilium/pubis. Both Paley and Wedge osteotomies allow its hinging on the entire soft triradiate cartilage only, achieving good and easier coverage of the femoral head and the most desirable acetabular index (figure 3). We aimed to present the modified technique in detail, emphasizing its eventual advantages in comparison to the original Dega osteotomy and ‘San Diego’ modification. We also discussed our related literature review on various osteotomy techniques.
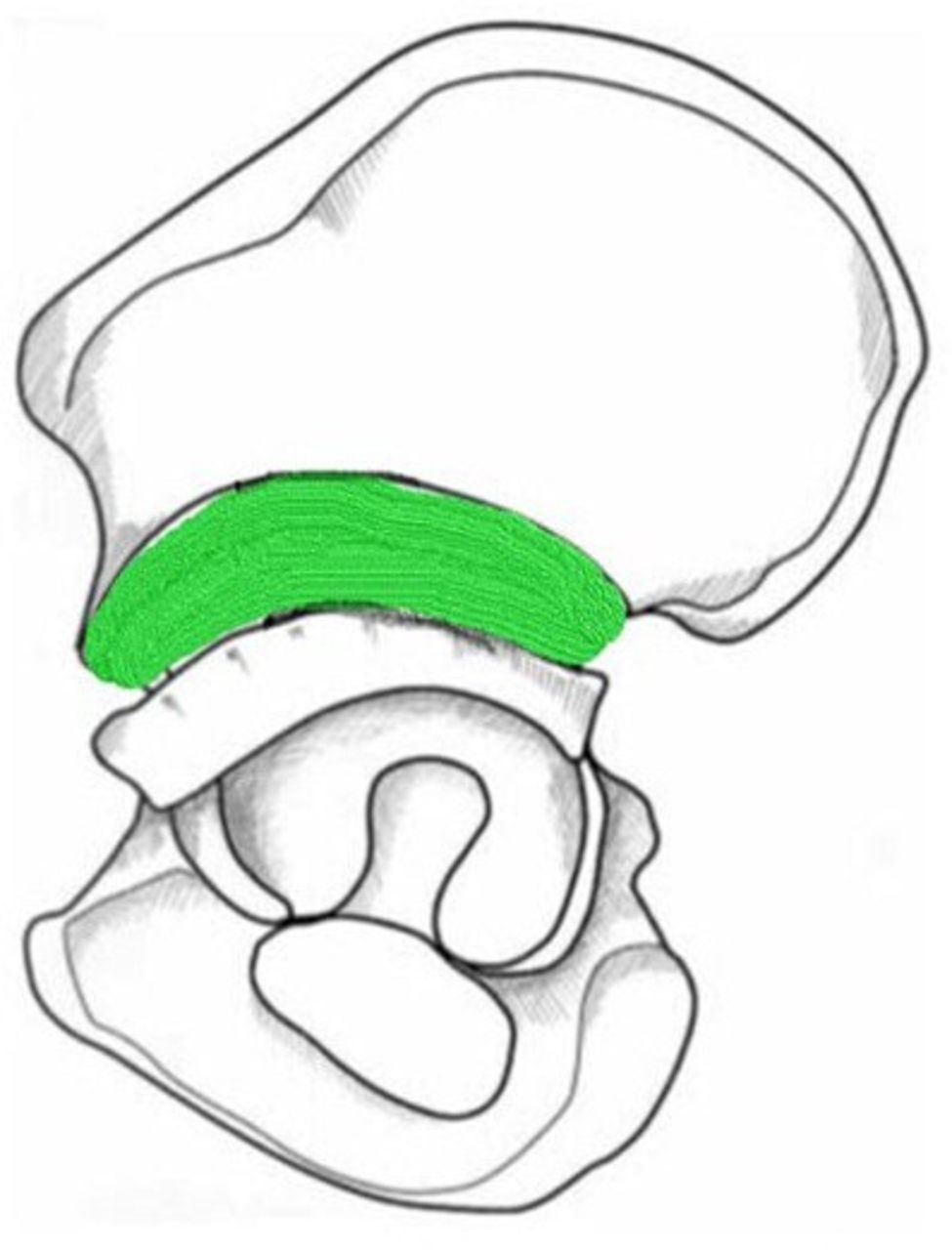
The San Diego Dega’s modification. Green represent the osteotomy. (Illustration by the senior author Noam Bor).

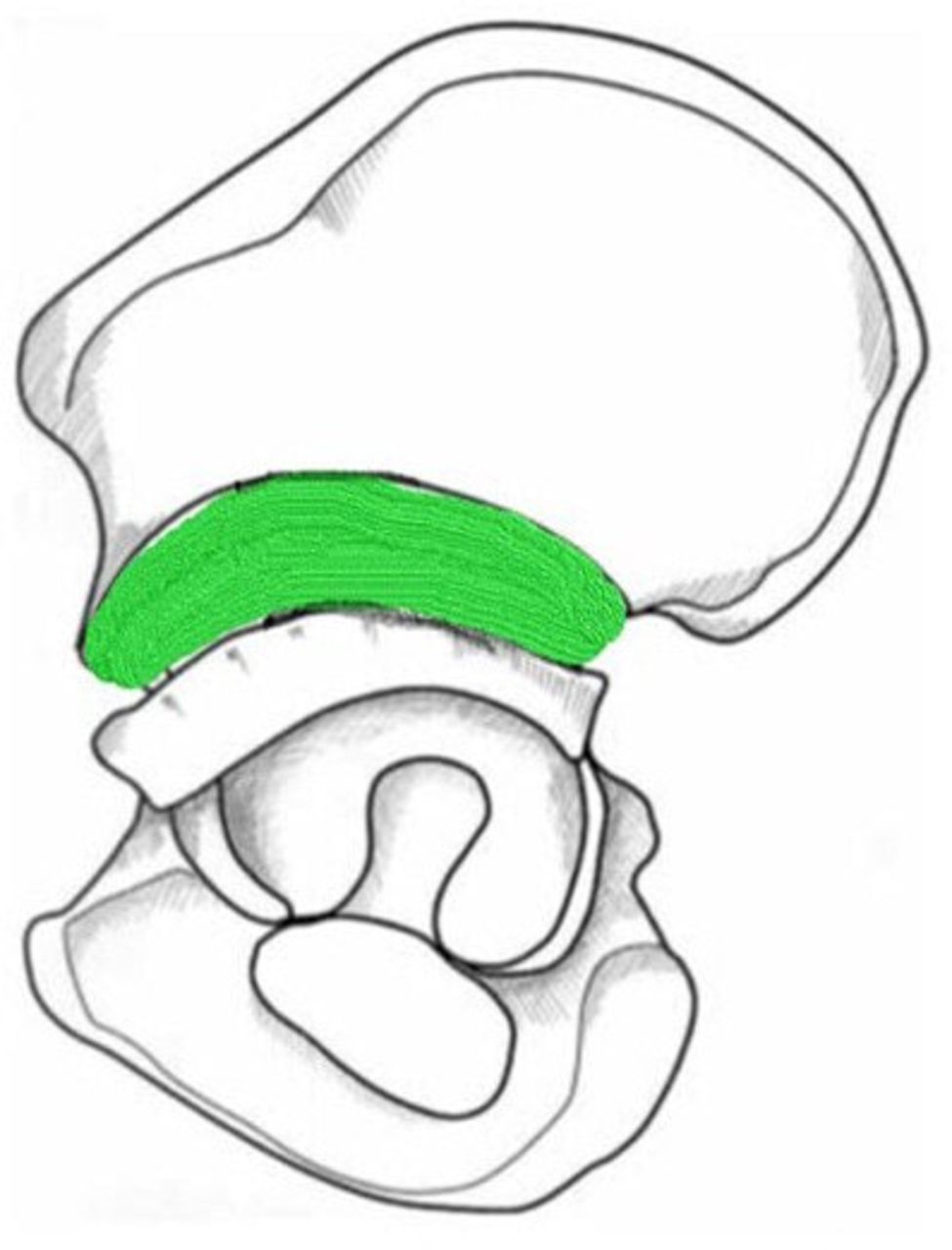
Paley’s modification of Dega osteotomy turned by 120° toward the ischial physis. (Illustration by the senior author Noam Bor).
Methods
Patients
After obtaining approval from the institutional review board, a retrospective chart review and radiographic analysis were performed on 25 patients (27 dysplastic hips) who since 2003, underwent modified Dega osteotomy described by Paley.12 We included patients aged >15 months with the diagnosis of either developmental dislocation of the hips (DDH) or cerebral palsy (CP). Exclusion criteria were patients with diagnoses of genetic syndromes. We analyzed anteroposterior X-rays of the pelvis taken before the procedure and in the early and late postprocedure periods. The X-rays were analyzed by an experienced pediatric orthopedist from our institute who was familiar with the parameters evaluated but was blinded to the images and the study. The images were randomly distributed before the evaluation. The parameters evaluated in all the X-rays were the acetabular index and center-edge angle.
Surgical technique
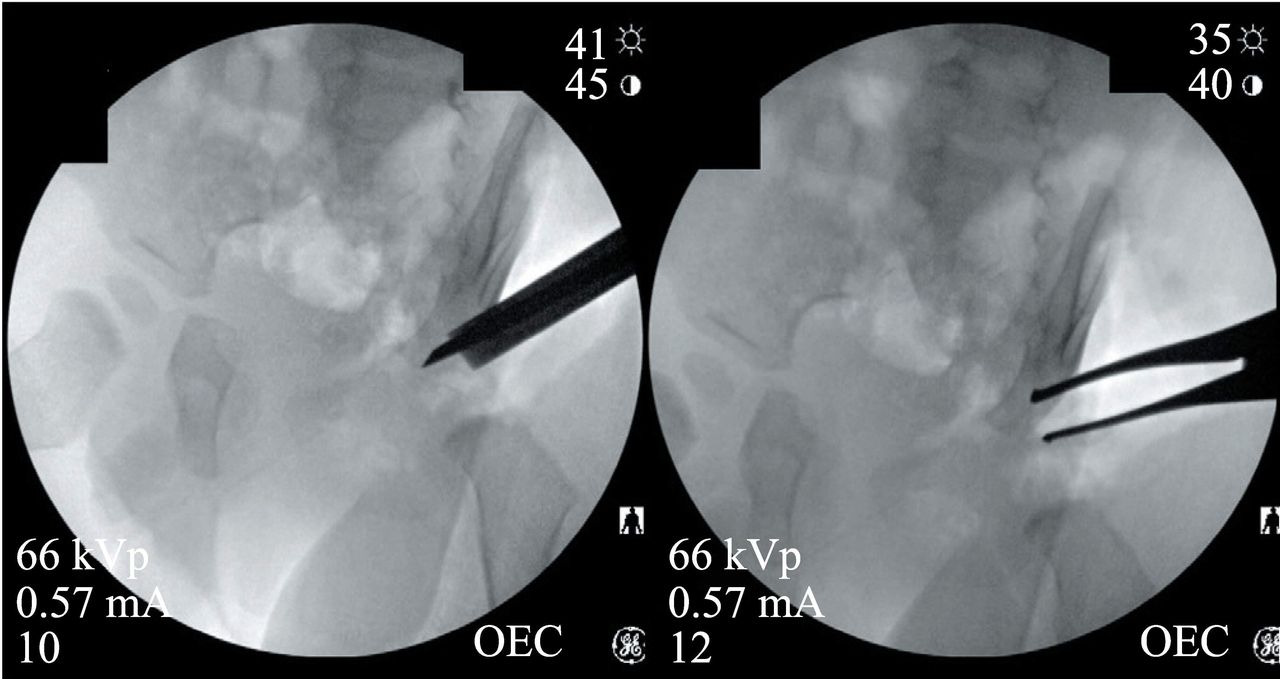
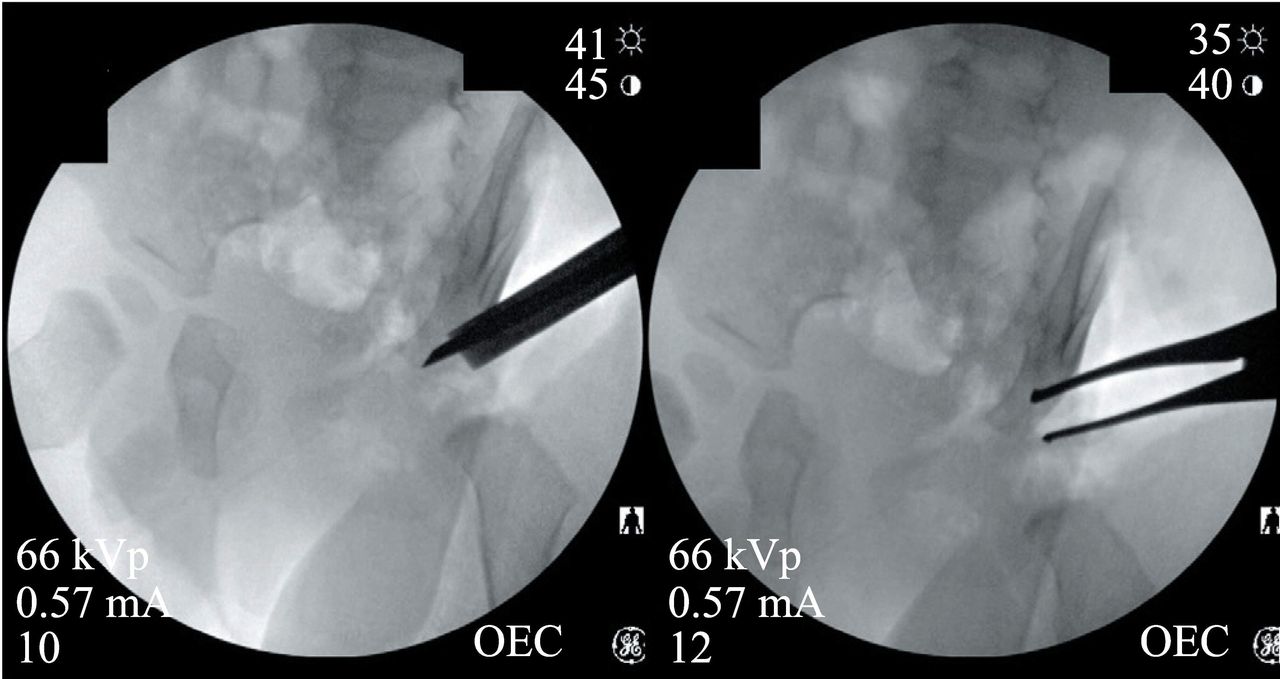
Using the image intensifier, a guide wire is drilled approximately 2 cm proximal to the lateral edge of the acetabulum toward the triradiate cartilage medially. With a 1.2 cm curved flat osteotome, only the lateral wall of the ilium is cut in the supraacetabular region. Starting at 1 cm proximal to the anterior inferior iliac spine, it continues on toward the triradiate cartilage at the pubic eminence, which is where the triradiate connects to the pubis. The unicortical osteotomy is a curved line, all the way perpendicular to the triradiate cartilage, that extends proximally to the level of the guide wire, separating the ilium from the pubis and the ischium. In the frontal plane, the osteotomy is inclined from proximal to distal and parallel to the guide wire. Then it runs parallel to the anterior wall of the sciatic notch. Posteriorly, the curve is cut to make a 120-degree turn, heading towards the ilioischial limb of the triradiate cartilage. At the most posterior distal part of the osteotomy, it is important to stay very near to the sciatic notch to avoid entering the hip joint inadvertently. The osteotomy ends at the triradiate cartilage medially. A laminar spreader is introduced into the ilium at the most lateral point of the ilium. Teeth of the spreader are inserted 2 cm into the osteotomy. The spreader is opened under direct vision and, with the use of the image intensifier, the amount of the correction of the acetabular index is evaluated. The vertical limb of the osteotomy extending down to the triradiate cartilage at the ischium allows for greater bending and greater posterior coverage. A bone graft from the iliac crest is inserted into the gap with its major part placed either posteriorly, laterally or anteriorly, depending on the major localization of the acetabular defect. The bone graft then is impacted with a punch. After withdrawal of the laminar spreader, the osteotomy is stable, and the biconcave or oval-shaped acetabulum is contoured to the reduced femoral head (figures 3 and 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
120-Degree osteotomy turning towards the ischial limb. Widely opening with the laminar spreader.
Results
The results of our study are summarized in table 1. We notice that better improved radiological indices are achieved in patients suffering from DDH in comparison to the patients with CP which is composed of older age patients’ group. The osteotomy is above the triradiate coverage, the deficient posterior wall is below the triradiate, and therefore lesser posterior acetabular coverage is achieved in those patients.
Clinical data of patients who underwent modified Dega osteotomy
The entire soft triradiate cartilage makes the outer iliac table to easily turn down, presented with major improvement in the preoperative acetabular indexes and the center-edge angles, with comparison to the postoperative data. Growth arrest events did not occur in any of our patients.
Discussion
A thorough review of the English literatures (table 2) showed that some authors elected for the original Dega osteotomy technique,13 whereas others preferred the ‘San Diego’ modification as described by Mubarak et al.7 Major modifications of the original Dega osteotomy by some authors were reported as well.
Literature review on various osteotomy techniques
The Pemberton osteotomy starts approximately 10–15 mm above the anterior inferior iliac spine, curves gently posteriorly and ends at the level of the ilioischial limb of the triradiate cartilage halfway between the sciatic notch and the posterior part of the acetabular rim. The osteotomy probably hinges at the triradiate cartilage, but theoretically, it may also hinge at the symphysis pubis.1–3 The Pembersal osteotomy described by Perlik et al4 originates from a serendipitous variation on the Pemberton osteotomy and is similar to the Pemberton osteotomy, except for the posterior extent, which continues more caudally to cross the ilioischial limb of the triradiate cartilage, extending into the body of the ischium. Theoretically, this osteotomy hinges at the triradiate cartilage, symphysis pubis and ischial osteotomy site, providing both acetabular redirection and reshaping.4 Given the inadequate exposure of the ischial region caudal to the sciatic notch, it is difficult for the surgeon to know whether, or where, the osteotomy actually crosses the ilioischial triradiate limb, thereby raising a question as to whether a Pemberton or a Pembersal procedure is actually being performed. Furthermore, because the caudal extension of the Pembersal osteotomy crosses the triradiate growth cartilage, there is a potential for damage to the triradiate cartilage.
The original acetabular osteotomy described by Dega6 was clearly presented by Grudziak and Ward.13 The osteotomy starts just above the anterior inferior iliac spine, curving upward and posteriorly, reaching a point approximately 1–1.5 cm in front of the sciatic notch. The osteotomy exits through the inner cortex just above the iliopubic and ilioischial limbs of the triradiate cartilage, and the posterior one-third of the inner cortex is left intact.13 In this study on 24 hips, the acetabular index improved, with the following specific findings: preoperatively, it averaged 33°, with a range of 20°–46°, and postoperatively, it averaged 12°, with a range of 6°–23°. The preoperative center edge (CE) angle (range, <−30° to 18°), was positive and improved in all the hips at the time of follow-up to an average of 31°−32°.
The theoretical location of the hinge in the Dega osteotomy can involve, to varying degrees, the sciatic notch, posterior portion of the inner pelvic cortex, horizontal limb of the triradiate cartilage and symphysis pubis. The hinge point is variable and is not confined solely to the triradiate cartilage. In a younger child with a wide-open triradiate cartilage, most of the hinging occurs at the sciatic notch and the triradiate cartilage. As the child gets closer to skeletal maturity, more hinging probably occurs at the sciatic notch and the symphysis pubis. Some authors believed that the procedure did not sufficiently increase coverage of the femoral head because the posteromedial cortex of the ilium and the greater sciatic notch were not cut.12–14
Mubarak et al7 described the modified Dega osteotomy (‘San Diego’), in which bicortical cuts were made in the anterior inferior iliac spine and the greater sciatic notch (figure 2). With this modified procedure, the posterior coverage of the femoral head is increased by placing a larger bone graft in the posterior part of the osteotomy. The San Diego osteotomy is not completely hinging on the triradiate cartilage because it extends toward the sciatic notch, virtually missing the ischial segment of the cartilage.
The radiological results of 18 hips in the study by Mubarak et al were as follows: the mean acetabular index preoperatively was 30°, with 8 of the 18 hips having an index of >30°. At the latest follow-up, the mean index was 14°. At the latest follow-up, the mean CE angle was 33°.8
In patients with either DDH or CP, most authors uses the above-mentioned procedure7 15–24 or the original Dega osteotomy13 25–34 (table 2). Paley,8 11 Paley and Standard,9 Eidelman et al,10 Roposch and Wedge12 have independently come up with similar osteotomies that differ greatly from the Dega, Pemberton or ‘San Diego’ types. Both the Paley and the Wedge osteotomies incline down to exit at the triradiate instead of the medial cortex. In contrast to the Paley osteotomy, which is a unicortical all the way and continues also towards the triradiate cartilage at the pubic eminence (where the triradiate connects to the pubis), the Wedge osteotomy exits at the medial cortex, although only at the very short segment of the ilium wing, where it hinges anteriorly on bone instead of continuing on toward the pubic eminence triradiate cartilage and hinging there.
In effect, all these osteotomies are a progression from the horizontal cut of the Pemberton to the more inclined cut of the Dega, to mostly unicortical cut of the Wedge and to the completely unicortical cut of the Paley. The Paley and Wedge modifications of the periacetabular osteotomy are the only techniques that approach the triradiate cartilage, which becomes a single hinge; there is true hinging in a three-dimensional way on the triradiate. The triradiate cartilage turning point makes the osteotomy procedure easier, more amenable and results with good coverage especially in very dysplastic hips characteristic of patients born with congenital femoral deficiencies.8–11 In the original study by Roposch and Wedge on 32 patients (41 hips), the acetabular index improved from 32° (49° sharp angle) preoperatively to 17° (35° sharp angle) postoperatively.12
Our osteotomy is following the Paley technique. The first author (NB) personally learned the method from Dr Paley since 1998, demonstrating the technique during his frequent ‘visiting professor’ to Afula, year after year.
The Dega, Pemberton or Mubarak (‘San Diego’) osteotomies are all bicortical and exit on the medial side of the iliac bone; whereas in Paley’s osteotomy the entire inner cortical wall is preserved. It frees the acetabulum only through the outer cortical iliac bone and intervening cancellous bone. Therefore, we think this modified periacetabular osteotomy is more stable, and the acetabular fragment is still sufficiently mobile to achieve good correction posteriorly and laterally.
Gordon et al1 reported on the use of the Pemberton pelvic osteotomy to treat patients with neuromuscular hip dysplasia. They concluded that the osteotomy substantially improved the anterolateral coverage, but care had to be taken when performing this in dislocated hips of neuromuscular cause; once the teardrop was substantially widened preoperatively, adequate coverage was difficult to attain. Compared with the Pemberton osteotomy, the method we presented in the current study is applicable to subluxated and dislocated hips. The cut, which extends into the ischium, provides a longer acetabular roof, thereby enhancing coverage.
Some different modifications to the original technique described by Dega are reported in the literature. In the procedure by Raichel and Hein, the medioposterior cortical corner remains intact, representing the rotation center, the point where the acetabular roof is deflected to the lateral and anterior sides.14
Ming-Hua et al30 described their modified technique, also known as ‘the high Dega osteotomy’, in children with DDH aged between 1.5 and 6 years. The osteotomy cut at a higher level is similar to the Salter pelvic osteotomy. The opening and rotation of the higher osteotomy site are retrieved and corrected by the inherent flexibility of the symphysis pubis and triradiate cartilage. According to the authors, the high osteotomy avoids injury to the triradiate cartilage and the risk of premature physeal closure.
In 2006, Robb and Brunner35 reported their experience of 52 hips in non-walking patients with severe CP and proved that the osteotomy technique, very similar to the one adopted by us, was applicable also after the closure of the triradiate cartilage in adolescents. The unicortical iliac cut is made through the outer table of the ilium, around the acetabulum, and down into the posterior column.
The study by El-Sayed et al,27 involving mostly patients with DDH younger than 4 years, reported unfavorable final clinical outcomes following the classical Dega osteotomy. In the opinion of the authors, this might be attributed to the thin and small size of the ilium at that age, which made the osteotomy more technically demanding. The degree of correction and inclination of the outer table of the ilium after the osteotomy also was restricted, as indexed by the postoperative acetabular inclination values.
Controversies exist in regard to the volume of the acetabulum following the classic Dega osteotomy. Ozgur et al31 used MRI to visualize the cartilaginous part of the joint and showed increased acetabular volume. Chung et al25 performed a similar study and showed a statistically significant increase of 68% in the acetabular volume following the classic Dega osteotomy on 17 hips.
In our study with the described osteotomy, patients with CP achieved inferior results in comparison to the patients with DDH. This is most probably related to the older age group of these patients and continues abnormal muscular spasticity and forces across the hip joints. It also might be explained by a better superior-lateral coverage and anterior coverage, which can be obtained. Because the osteotomy is still above the triradiate coverage and the posterior wall is below the triradiate, lesser posterior acetabular coverage is achieved, mostly defective in patients with CP. Therefore, in cases which require changing the acetabular version or specifically increasing posterior coverage, especially in patients suffering from CP, the triple osteotomy would be better.
In conclusion, the only similarity between the Paley and Wedge osteotomies and the original Dega is that the former, which incline downward toward the triradiate, are the only techniques in which the limbs of the triradiate cartilage are true and become a single hinge where the osteotomy turns. The entire soft triradiate cartilage makes the outer iliac table to easily turn down, allowing the achievement of a good acetabular coverage. However, when comparing the various preoperative and postoperative radiographic indices between previous studies and our study, the results seem to be almost comparable. That said, we still consider the entire triradiate cartilage as a better hinge point for the iliac osteotomy. The difference between the osteotomy adopted in our institution according to Paley and the modalities described in the literature by most authors is that the latter mostly ignore or miss the ischial limb of the triradiate cartilage.
References
Footnotes
Contributors BN contributed to conceptualization, and conducted all procedures, including data curation, formal analysis, investigation, writing the original draft and revised manuscript. DE was responsible for data curation, formal analysis and investigation. RN carried out data curation, formal analysis and investigation. RG performed data curation, formal analysis, investigation and wrote the revised manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The retrospective study was approved by the local ethical committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.