Article Text

Abstract
Introduction Numerous meta-analyses done on adults suggest superiority of continuous mass closure technique, but any such study does not exist for the pediatric age group. The results in adults cannot be applied to pediatrics because of numerous physiologic and anatomic differences.
Methods This is a single-blinded, randomized controlled trial, 1:1 parallel groups, that compares the frequency of dehiscence between the interrupted and continuous mass closure techniques for transverse incisions in pediatric patients. The age range was from birth to 12 years. We sampled 350 patients undergoing emergency or elective exploratory laparotomies in our pediatric surgery unit. Blocked randomization was used and only the patients remained blinded during the intervention. One group was closed with interrupted mass closure (group A) and the other group with continuous mass closure technique (group B). We had to drop 50 patients for not meeting the inclusion criteria.
Results The wound dehiscence rate for group A was 1.34% (4 patients) and for group B was 3.0% (9 patients). Significance was calculated using χ2 (p<0.156). The global wound dehiscence rate was 4.34% (13 patients). The maximum number of patients dehisced on the fifth postoperative day, while the range was 4–11 days. The only statistically significant confounding factor was wound classification (p<0.002).
Discussion Statistically there is no significant difference between interrupted and continuous mass closures techniques in terms of wound dehiscence. The dirty wounds are at a maximum risk of developing wound dehiscence irrespective of the technique used. We need to strictly adhere to the basic principles of closure especially when dealing with dirty wounds.
Trial registration number TCTR20150318001.
- pediatric mass abdominal closure
- pediatric abdominal wound dehiscence
- pediatric interrupted mass abdominal closure
- pediatric continuous abdominal mass closure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- pediatric mass abdominal closure
- pediatric abdominal wound dehiscence
- pediatric interrupted mass abdominal closure
- pediatric continuous abdominal mass closure
Introduction
There are numerous techniques available for closure of the abdomen. Modern closure methods such as continuous and interrupted suturing techniques have their pros and cons. The rate of dehiscence for interrupted suturing technique is 0%–3.98%,1 2 while for continuous suturing technique 0%–14.8%.3 4
The adult literature recommends continuous mass closure technique in routine midline laparotomies.5 The pediatric surgical texts favor the same based on adult literature.6 The literature lacks a randomized controlled trial comparing continuous versus interrupted mass closure techniques in transverse incisions in children. The results in the adult population cannot be applied to pediatric population because of major anatomic and physiologic differences between the two age groups. Transverse incision is preferred in children as compared with midline because the abdomen of neonates, infants, and small children is ellipsoid-shaped, low-lying umbilicus, small pelvis, intra-abdominal urinary bladder, and proportionally large liver.7 Postoperatively additional risk factors exist, leading to increased intra-abdominal pressure because of the intra-abdominal urinary bladder and the proportionally large liver. These pose additional risk for dehiscence.8 9 Therefore, there is a need to study the outcomes of closure method in a study designed for children.
A study of this type will provide evidence for optimum closure technique in children. It will solve the controversy regarding the optimum laparotomy closure technique in children. This randomized trial is an attempt to solve this question in pediatric population. There are various local and systemic risk factors associated with increased risk of wound disruption.10–12 However, the factors amenable to the surgeon are incision type, closure technique, and suture type.13 In this study we are going to focus on closure technique. We will close laparotomy wounds with either interrupted or continuous mass closure technique and measure dehiscence in each closure group as our outcome. We will study the difference between the rate of dehiscence in the two closure groups.
Methods
After ethical approval from our institution, we applied for the registration of our trial. Participants were individually randomized prospectively to one of two “parallel” groups in 1:1 allocation ratio throughout the study consecutively.
Eligibility criteria
All patients from newborns to 12 years who underwent exploratory laparotomy via transverse incision at the Department of Pediatric Surgery, The Children’s Hospital and The Institute of Child Health, Lahore, Pakistan, from April 2013 to November 2013 were included in the study. Both emergency and elective patients were included in the study after informed consent from parents.
The maximum reported wound dehiscence day reported in the literature is 31 days; thus, we excluded cases that died before 31 days after surgery.
Intervention
To remove bias, patients’ preoperative and postoperative treatment were standardized. Surgeons, from consultants up to postgraduate trainees, were involved in this study. All were instructed about the standard procedure to be adopted preoperatively, intraoperatively, and postoperatively. We adopted all standard measures such as: control the primary injury and source of intra-abdominal infection before closing, drains and stomas were inserted through a separate incision, the edges of wounds were checked for good vascularity, tension-free closure, the suture length to wound length ratio was at least 4:1 in all of our closures; postoperative cough, if present, was managed aggressively; abdominal distension, if present, was prevented by nasogastric aspiration and the skin of all dirty wounds was closed by delayed primary closure. The method for both continuous and interrupted mass closures was standardized. The fascia and the peritoneum were closed as a single mass layer. Only absorbable sutures (polyglactin) were used. However the size of the sutures used was determined on a case-by-case basis due to the huge diversity in the age of patients, but was kept similar for each age group.
In the interrupted group (group A), a single anchoring suture was placed at both ends of the incision. Further sutures were placed from the edge to the middle direction from both sides alternatively; once the midpoint was reached, the sutures were overlapped toward the opposite edge for at least one stitch count. Each suture was tied with at least four knots.
In the continuous group (group B), the first stitch was anchored at one end of the incision, and after reaching the other end of the incision in simple continuous manner it was tied with at least four counter-rotating knots.
The patients were monitored in or out of hospital for 31 days.
Outcome
Wound dehiscence was our primary outcome. We defined it as “when all layers of the abdominal wall have burst apart with or without associated evisceration, within 31 days after the operation.” We also studied wound classification, age, bilirubin, and weight of patient as confounding variables.10 11 14–17
Sample size
With a two-sided significance level of alpha=0.05 and a power of 85%, a sample size of 150 patients per group was calculated using the maximum percentage of dehiscence in both groups, that is, 3.98% in the interrupted closure group2 vs 14.8% in the continuous closure group,4 after exploratory laparotomy.
Randomization and blinding
Randomly varying blocked randomization numbers were generated using software.18 They were put inside sealed envelopes by the principal investigator and were opened only before closure of the abdomen. The patient or the parent was not made aware of the allocated group, while the surgeon only knew at the time of opening the envelope.
Statistical methods
For the primary outcome we used χ2 statistic to calculate the p value between the two groups. Confounding variables were analyzed by binary logistic regression analysis.
Results
The wound dehiscence rate for the interrupted closure group (group A) was 1.34% (4 patients) and for the continuous closure group (group B) was 3.0% (9 patients). The significance was p<0.156, calculated using χ2. The global wound dehiscence rate was 4.34% (13 patients). The maximum patients dehisced on the fifth postoperative day, while the range was 4–11 days.
We excluded 50 patients from the analysis because they could not meet the eligibility criteria for the study. These patients had lethal genetic and metabolic disorders and could not survive 31 days after laparotomy.
Figure 1 show participant flow. Table 1 shows baseline data.
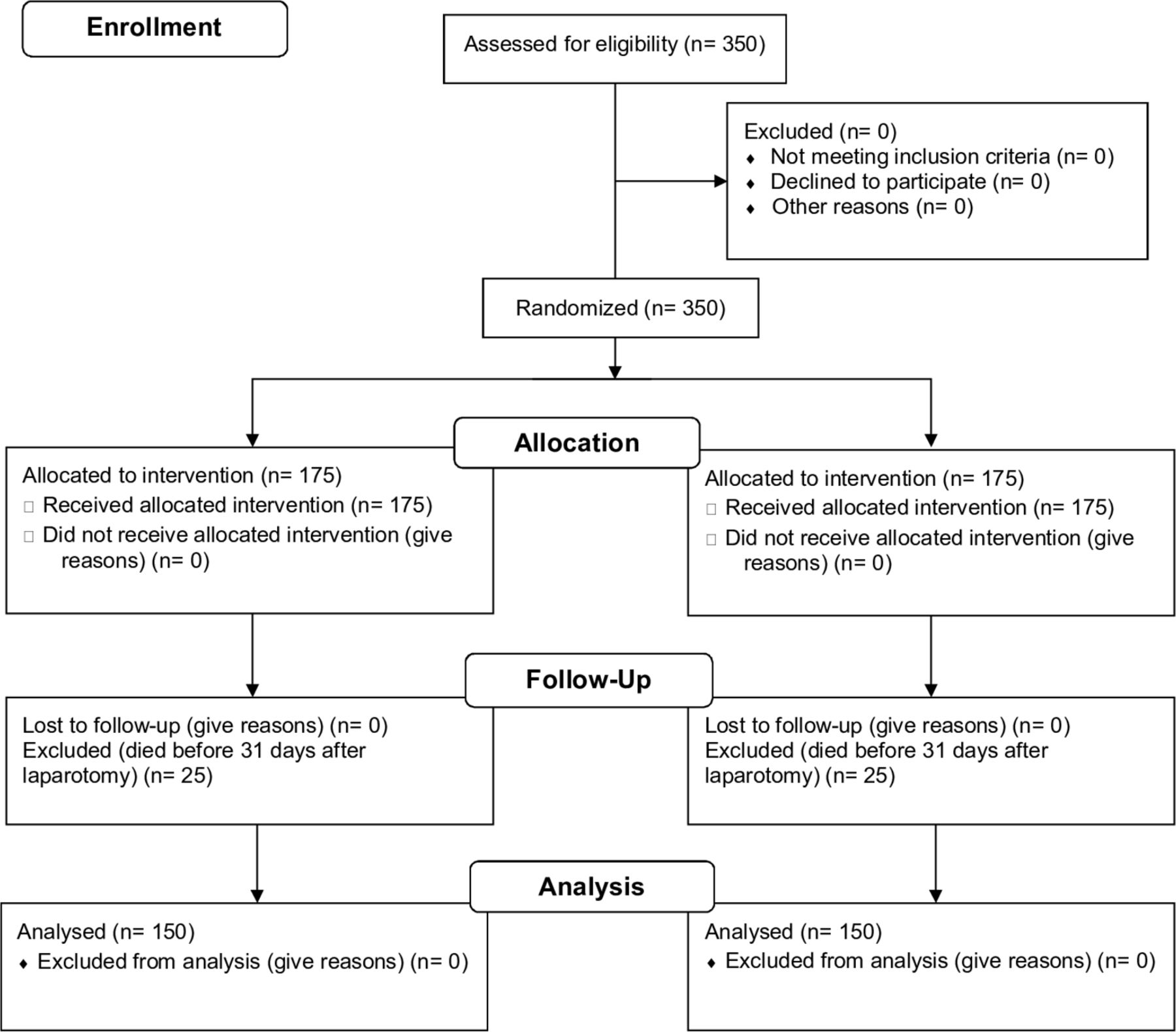
{kind=link}
Randomized trial to compare dehiscence withcontinuous versus interrupted mass closure of transverseincisions in children with absorbable suture flow diagram.
Baseline demographic characteristics
To study the influence of potential covariates on wound dehiscence, we calculated the p values for each confounding factor using binary logistic regression analysis, as shown in table 2.
Binary logistic regression analysis showing the influence of potential risk factors on the development of wound dehiscence
Discussion
We found wound classification as the sole significant indicator of the risk of dehiscence. All patients with clean wounds developed no dehiscence with either of the techniques. Nine cases of dehiscence occurred with dirty wounds, while there were three cases in contaminated wound and only one with clean-contaminated wound. We calculated another p value, this time only using the dehiscence in dirty wounds. We analyzed all dirty cases (see table 1) which developed wound dehiscence to see any significant difference in the rates of dehiscence versus the closure technique used. Thirty-one were closed with interrupted technique and 45 by continuous, while dehiscence developed in 3 and 6 cases, respectively. The result was p<0.627. This reiterates the null hypothesis of our study that there is no difference between the techniques used when it comes to developing wound dehiscence.
If we look at the study by just percentages, the interrupted group only had four dehiscences, while the continuous group had nine dehiscences. This also goes with traditional teaching that interrupted closure is the preferred method for dirty and contaminated wounds. Continuous suture technique distributes tension equally throughout the wound, allows the wound to adjust to the stresses and strains of the postoperative period, and takes significantly less time to complete the closure as compared with interrupted mass closure method. However if a single suture breaks down, then the whole wound disrupts. The interrupted technique can hold even if one or two sutures give away, but it is time-consuming and it isolates tension to each individual stitch. However our study clearly shows it is not the technique that has any impact on the final outcome in terms on wound dehiscence. The above pros and cons for each technique, each having its own mechanism, have statistically insignificant role in causing wound dehiscence.
Age was found to be non-significant (p<0.063). Weight has not been found as a risk factor for wound dehiscence in recent literature.11 The same was the case in our study (p=0.601). We even had 33 low birthweight newborns and 1 very low birthweight newborn. None of them developed any wound dehiscence. With good medical management nowadays, our two cases with bilirubin more than 6 mg/dL did not develop dehiscence, and this variable was also not a significant predictor of wound dehiscence in our study.
We had a total of 13 dehiscences. In each case after dehiscence, retention closure was done and no further intervention was required with regard to wound management during the duration of our study. The mortality rate due to dehiscence was 0%. We excluded 50 cases from the study after randomization; they did not meet the eligibility criteria because they did not live up to 31 days after the life-saving laparotomies done for them. Thus their outcome was not analyzed in the final analysis. None of them died because of dehiscence, but they died due to multiple genetic and metabolic problems.
We did encounter limitations in our study, due to the increased number of patients in our hospital, increased workload, and limited number of staff available to conduct the study. Both postgraduate trainees and experienced surgeons closed the abdomen. Although we demonstrated standard technique to all, strict compliance was variable. The extent to which this affects our results is unknown. It is universally accepted that interrupted closure takes more time as compared with continuous closure. In adults the mean time is 45 min, while for continuous mass closure it is 15 min.11 17 However we did not record closure times. We have a total duration of surgery, but we do not have the total time taken to close the abdomen. Although this factor is more valid for postoperative intensivist, how much it affected our final outcome was not measured. We also have no record of the size of sutures used to close the abdomen. We always used absorbable polyglactin, but due to wide variation in age the size had to be selected accordingly. Our study was limited to only one outcome, which was wound dehiscence. Incisional hernia is another outcome which can be used to determine the efficacy of abdominal closure, but it needs a follow-up of at least 3 years. We had limited time to complete this study and this outcome was not included in our study.
Our study showed almost double the number of dehiscence in the continuous closure group, but still the p value was insignificant. We think that inclusion of incisional hernias as the outcome in future studies would give us more answers.
Our results can be generalizable to any institution based on these facts:
Wide age group, which is representative of the pediatric population presenting to any institute around the world.
Wide array of diseases selected and randomized for the study.
The materials and methods are described in detail, allowing any institution to execute and confirm the results.
Conclusion
The closure method for the transverse incisions in the pediatric age group between interrupted or mass closure techniques is neither superior nor inferior to each other in terms of developing wound dehiscence. We need to be careful in dirty cases as they pose a significant risk of developing wound dehiscence. Probably another randomized controlled trial can be designed to determine the significance of the two techniques in developing incisional hernia.
Footnotes
Contributors All authors had substantial contribution to the conception and design of the work, including acquisition, analysis, and interpretation of data. Drafting the work was done by SK, while revising it critically for important intellectual content was done by MS and NT. Final approval of this version was given by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The corresponding author was working at the Department of Pediatric Surgery, The Children’s Hospital and The Institute of Child Health during the conduct of the study. Now he has moved to the Department of Pediatric Surgery, Armed Forces Hospital Southern Region, Kingdom of Saudi Arabia.