Article Text

Abstract
Objective To assess the results and complications of dorsal vertical island flap (DVIF) urethroplasty.
Methods A total of 175 children were operated on for hypospadias. Out of these, 41 with proximal hypospadias with severe chordee required two-stage urethroplasty. In 18 babies with glanular hypospadias, a meatal advancement and glanuloplasty procedure was done. In 25 babies with mid-penile and distal penile hypospadias, tubularized incised urethral plate (TIP) urethroplasty was the option. 16 babies with unhealthy urethral plate and chordee were chosen for dorsal vertical tube urethroplasty after excision of the urethral plate. The rest of the 75 babies with proximal, mid-penile or distal penile hypospadias with no or minimal chordee after degloving and poor urethral plate were chosen for DVIF urethroplasty. These 75 babies with DVIF were followed up from 3 months to 5 years to assess complications such as urethrocutaneous fistula, meatal stenosis, glans dehiscence, megalourethra or urethral diverticulum, stricture, and penile torsion/rotation.
Results A total of 75 patients with proximal, mid-penile, or distal penile hypospadias in whom DVIF was used during the study period were included. The mean age was 3.7 years, ranging from 8 months to 14 years. Fourteen patients developed complications (18.6%). The most common complication was urethrocutaneous fistula, which was seen in seven (9.3%) patients. Glans dehiscence was seen in five patients (6.6%), and one had meatal stenosis with diverticulum formation. Skin necrosis was observed in one patient. In 61 patients, stream was good, with no torsion, and good cosmetic appearance was observed.
Conclusions DVIF is a good alternative to TIP in mid-penile and distal penile hypospadias. Our early experience with DVIF urethroplasty showed an acceptable rate of complications and good cosmetic results.
- hypospadias
- chordee
- dorsal
- vertical
- urethroplasty
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Hypospadias has been reported to occur approximately in 1 out of 100–300 live male births.1 The great majority (87%) are anterior hypospadias (mid, coronal and glanular), with posterior hypospadias constituting only 13%.2 Neourethra may be created by tubularization of the native urethral plate, especially if there is deep glanular groove,3 or by various flaps if the urethral plate is unhealthy. The concept of flaps was introduced by Hodgson4 and Asopa et al 5 in the early 1970s. This was further developed by Standuli6 7 in 1979 and widely popularized by Duckett8 in 1980. The main disadvantage of these preputial flaps is torsion or rotation of the penis, and sometimes outer skin necrosis. Dorsal vertical island flap (DVIF) was introduced by Scuderi and Campus9 to overcome these problems, and was popularized by Perović and Vukadinović10 in 1994 and Santulli et al 11 in 2001. We present our experience with DVIF.
Methods
One hundred and seventy-five children were operated on for hypospadias in the Medical College Hospital during the period between June 2012 and July 2017. Out of 175 children, 21 with penoscrotal and 20 with proximal penile hypospadias with severe chordee required two-stage urethroplasty. In 18 babies with glanular or coronal hypospadias, a meatal advancement and glanuloplasty procedure was done. In 25 babies with mid-penile and distal penile hypospadias with healthy urethral plate and good spongiosum, and with no chordee, tubularized incised urethral plate (TIP) urethroplasty was the option. Sixteen babies with mid-penile or distal penile hypospadias with unhealthy urethral plate or requiring urethral plate excision due to chordee were chosen for dorsal vertical tube urethroplasty. The rest of the 75 babies with proximal, mid-penile or distal penile hypospadias with no or minimal chordee after degloving and with poor urethral plate which is very thin and not suitable for tubularization were chosen for DVIF urethroplasty. These 75 babies with DVIF were followed up from 3 months to 5 years to assess complications such as urethrocutaneous fistula, meatal stenosis, glans dehiscence, megalourethra or urethral diverticulum, stricture, and penile torsion/rotation.
Surgical technique
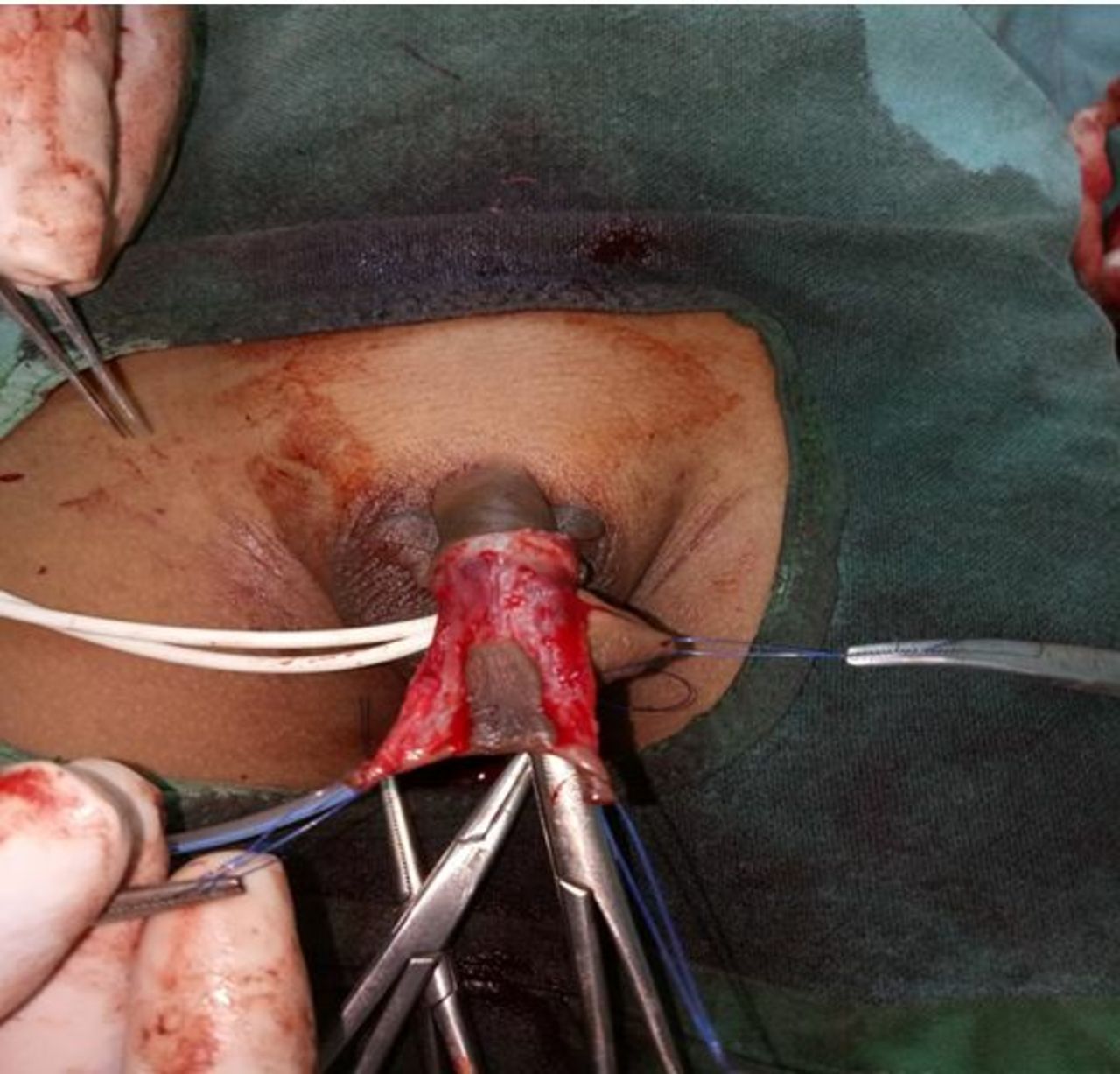
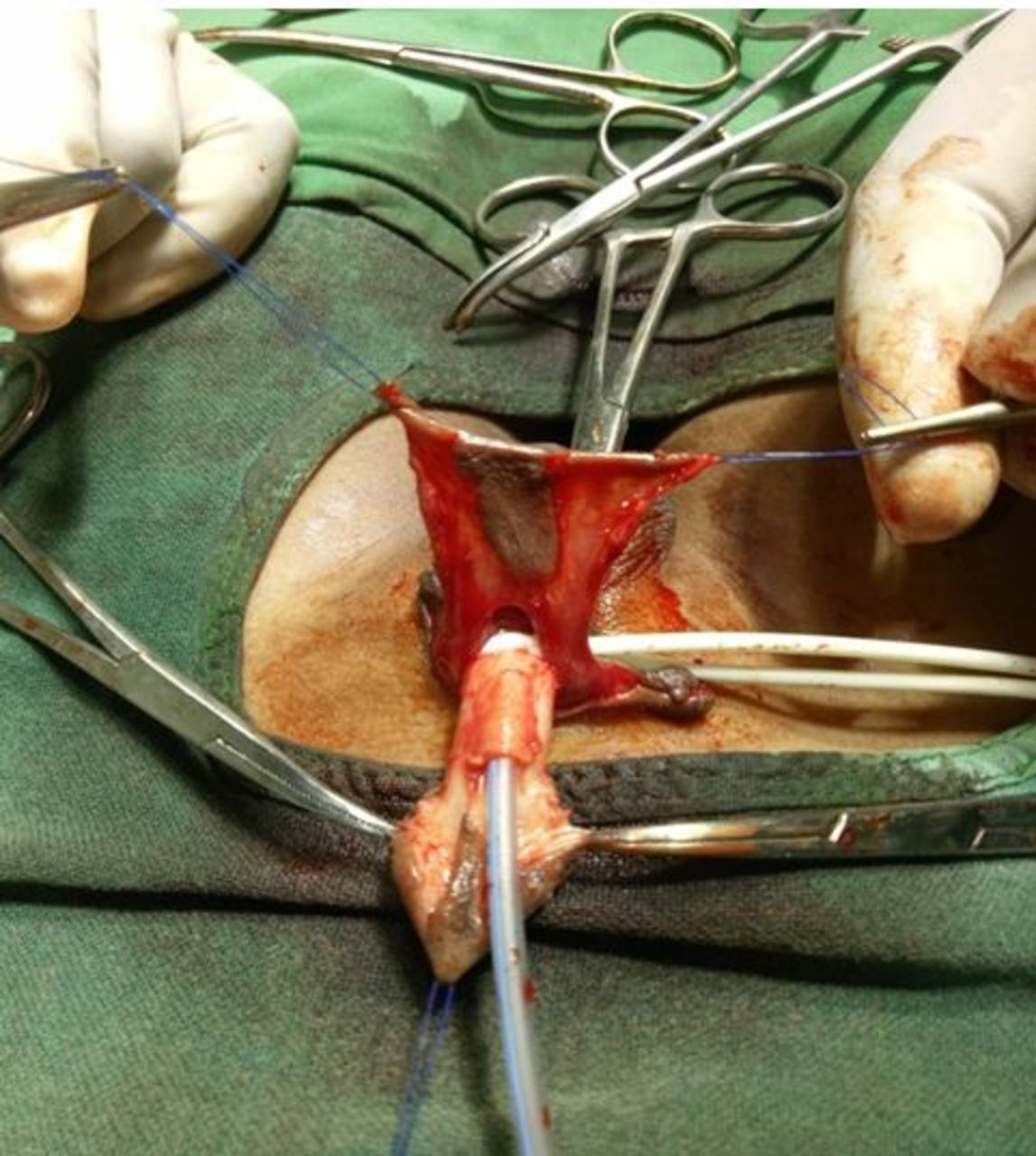
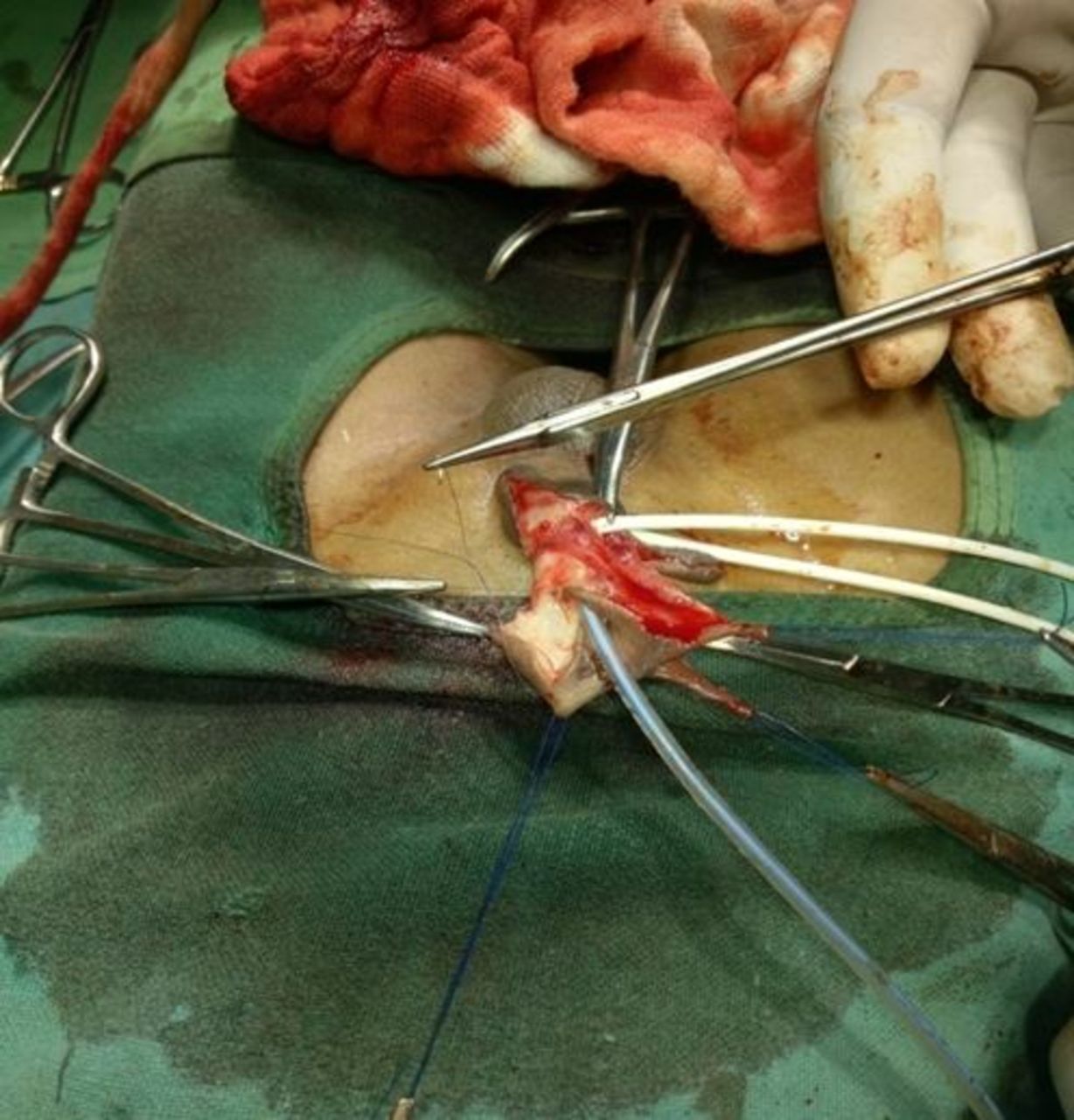
The DVIF procedure has already been described by Perović and Vukadinović in 1994.10 Briefly, after stitching the glans, the urethral plate is marked (6 mm) and penile degloving is done, preserving the native urethral plate and a collar 10 mm of the inner preputial layer around the corona (figure 1). Chordee correction was tested by injecting saline into the corpora. The urethral meatus was spatulated, and the vertical island flap was marked over the dorsal outer preputial and the distal penile skin vertically (figure 2). The width of the flap is usually reconstructed in a such a way that the neourethra should allow 7–9 Fr in infants and 10–12 Fr in older children. After marking the flap, the island flap is carefully dissected on the vascular pedicle (figure 3). Two lateral flaps were dissected from the island flap without compromising blood supply. These lateral flaps would be used to cover the ventral aspect of the penis if necessary. The island flap (DVIF) is transposed ventrally by buttonholing the center of the mesentery at its base (figures 4 and 5). The transposed flap lies perfectly in the position of the urethral plate without rotation or torsion of the penis. Now the flap is sutured to the urethral plate using 6–0 vicryl, with continuous running suture (figure 6). The suture lines are covered with the mesentery of the flap, with some interrupted sutures of 6–0 vicryl. Glanuloplasty was completed using 5–0 vicryl. The excess of the distal flap is excised and sutured to the glans to create a wide meatus. Preputial flaps were fashioned. The ventral cover is provided by rotating lateral flaps. Feeding tube was left for 1 week. These children were followed up after 1 week, 1 month, and 1 year after discharge.

Mid-penile hypospadias.

Vertical island flap marked over the dorsal skin.

Island flap dissected over the vascular pedicle.

Buttonhole is made in the mesentery of the flap.
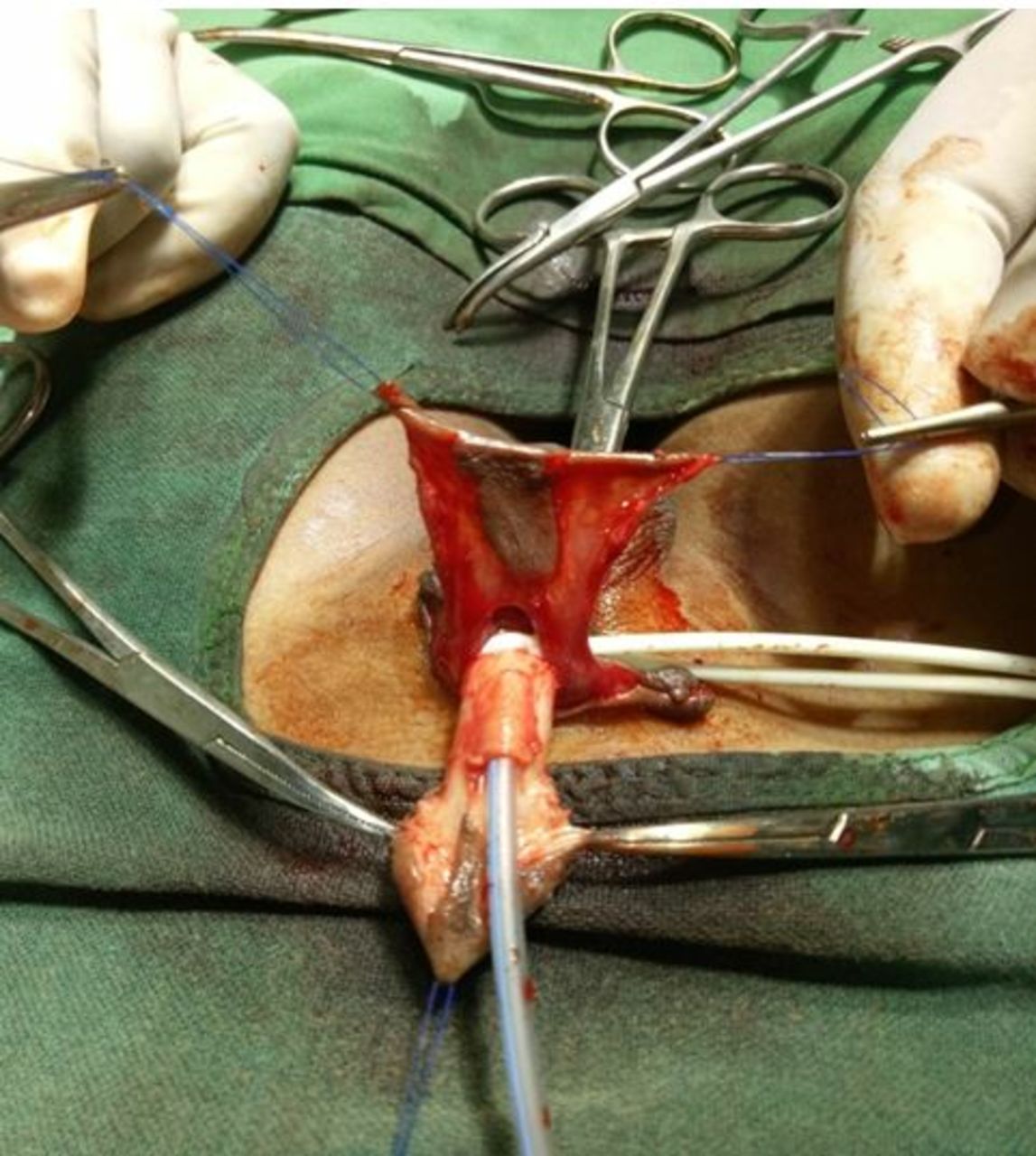
Island flap transposed ventrally.

Urethroplasty carried out by suturing the flap to the native urethral plate.
Results
A total of 75 patients with proximal, mid-penile, or distal penile hypospadias in whom DVIF was used during the study period were included. The mean age was 3.7 years, ranging from 8 months to 14 years. All patients were followed up for a minimum of 3 months to a maximum of 5 years. Fourteen patients developed complications (18.6%). The most common complication was urethrocutaneous fistula, which was seen in seven (9.33%) patients. Five of the seven patients who developed fistula were with proximal penile hypospadias in whom DVIF urethroplasty was done. The other two patients were with mid-penile hypospadias. Glans dehiscence was seen in five patients (6.6%). All five patients with glans dehiscence had relatively small-sized penis and underdeveloped glans. One child had meatal stenosis with diverticulum formation, and this child was a case of proximal penile hypospadias who required a long flap. We used transverse preputial pedicle flap in this case, which was brought ventrally by buttonholing the pedicle. Skin necrosis was observed in one patient. In 61 patients, there was no torsion, and good cosmetic appearance was observed (figure 7) and with good stream (figure 8).

Postoperative appearance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Urinary stream after 1 month.
Discussion
Many techniques have been described in the literature using vascularized flaps to reconstruct neourethra in patients with hypospadias.4–8 The dorsal vertical flap technique was first described by Scuderi and Campus9 in 1983, and later popularized by Perović and Vukadinović10 and others.11 We report our experience in using this technique. The main advantage of this technique is using the dorsal vascularized flap which is brought down ventrally by buttonholing the mesentery, causing no torsion/rotation of the penis, which is a common problem after island flaps.5 8 None of our patients had this problem. Another advantage of this technique is that it does not require cover with vascularized tissue as in TIP because the mesentery itself acts as a cover. We used this technique in 75 of our children with proximal, mid-penile, or distal penile hypospadias. The risk factors for hypospadias repair are proximal meatus, glans width less than 14 mm, and repairs without flap interposition. A total of 14 (18.6%) patients developed complications, which is comparable with other series of mid-penile or distal penile hypospadias repaired using various techniques including TIP.12–15
The most common complication in our series was urethrocutaneous fistula, occurring in 7 (9.3%) of 75 children. Meatus at the proximal shaft of the penis is a consistent risk factor of urethroplasty. We observed fistulas more commonly in children with proximal hypospadias where a long flap was used with long suture line. Our fistula rate of 9.3% is favorably comparable with other reports12 using preputial flaps, which have reported a fistula rate of 18% in their patients. Most of our fistulas were seen only at the proximal end of the anastomosis, which can be closed easily later on. Glans dehiscence occurred in five patients. Glans dehiscence is commonly observed in children with small penis with a stretched penile length of less than 3 cm and underdeveloped glans with a glans width less than 14 mm at the base. High incidence of glans dehiscence was reported by some authors.16 We raise glans wings liberally so we can close without tension. This decreased dehiscence in our series.
Meatal stenosis is a difficult problem to treat after urethroplasty. The incidence of meatal stenosis after various urethroplasties is 3%, and diverticulum formation in patients with tubularized or onlay preputial flaps is 12%.17 One of our patients developed meatal stenosis and diverticulum formation after urethroplasty. This child was a case of proximal penile hypospadias requiring long flap, and we used transverse inner preputial layer raised on the vascular pedicle transposed ventrally by buttonholing the pedicle. Excision of the diverticulum and redo-urethroplasty was done. Skin cover is not a major problem because two lateral flaps are well vascularized due to axial blood supply, and we rotate them to cover the ventral aspect of the penis especially in cases of proximal penile hypospadias. Uroflowmetry was done during the later part of our study, and most of the children had normal flow rates with bell-shaped curve.
Conclusions
DVIF is a good alternative to TIP in mid-penile and distal penile hypospadias, where the urethral plate is unhealthy due to deficiency of the corpus spongiosum. Our early experience with DVIF showed an acceptable rate of complications and good cosmetic results.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.