Article Text

Abstract
Background This study evaluates the validity of Alvarado Score in predicting disease severity and the development of postoperative complications in pediatric appendicitis.
Methods This is a retrospective, bicentered study on pediatric patients with emergency appendicectomy performed from 2006 to 2016. The relationship of Alvarado Score (low: 1–4, medium: 5–6, high: 7–10) and operative findings/complications was analyzed.
Results A total of 316 patients were included and the median age on admission was 10.8 years. The overall median score was 8.0. 13.3%, 20.2%, and 66.5% of patients had low, medium, and high risk scores, respectively. 36.1% of patients had complicated appendicitis and the median score was comparable with that of the uncomplicated cases (7.0 vs 7.4, p=0.21). More complicated cases were found in the medium-risk group (high vs medium vs low=29.7% vs 61.4% vs 31.0%, p=0.01). Rebound tenderness had the highest positive predictive value (65%) for complicated appendicitis. Postoperative complications were found in 16.5% of patients with a higher median score (7.87 vs 5.8, p=0.01).
Conclusion Alvarado Score does not predict disease severity but postoperative complication. Patients with medium risk score should also be treated promptly for the risk of having complicated disease. Rebound tenderness may be a signal for complicated appendicitis and should be properly examined.
- appendicits
- alvarado
- complications
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Appendicitis is a common cause of abdominal pain in children, with a lifetime risk of approximately 8%.1 Yet the diagnosis is sometimes difficult especially in young children who cannot report their symptoms accurately. A delayed diagnosis will increase the risk of disease-related complications such as perforation and intra-abdominal abscess formation. To assist in the diagnosis of appendicitis in children, different scoring systems have been proposed. The most frequently studied scoring systems are the Pediatric Appendicitis Score (PAS) and the Alvarado Score.2 While the PAS is applicable to children and adolescents only, the Alvarado Score could be used in both pediatric and adult patients. A meta-analysis published in the recent year suggested that the Alvarado Score has a higher clinical value in predicting the likelihood of appendicitis.3 It is a 10-point scoring system based on laboratory and clinical assessments. High sensitivity, specificity, and positive and negative predictive values for the diagnosis of appendicitis have been reported.4 5 However, whether this scoring system can also differentiate between mild and severe disease remains undetermined. In addition, whether the Alvarado Score can also predict the likelihood of postoperative complication has not been evaluated. The objective of this study is to evaluate its validity in predicting disease severity and the occurrence of postoperative complication in pediatric acute appendicitis.
Methods
This is a retrospective study conducted in two sister pediatric surgical units (Queen Mary Hospital in Hong Kong, and The University of Hong Kong-Shenzhen Hospital in Shenzhen) which share the same management algorithm for pediatric acute appendicitis. All the operations were performed by residents or consultants in pediatric surgery.
In this study, the medical records and admission notes of all pediatric patients (age ≤18 years) with emergency appendicectomy performed for acute appendicitis between 2006 and 2016 were reviewed. The diagnosis of appendicitis was made based on clinical features (right lower quadrant pain and tenderness, fever, and leukocytosis) with or without imaging. Ultrasound and CT scan were arranged if the clinical features were equivocal or appendiceal mass was suspected. All the resected specimens were subjected to histologic analysis to confirm the diagnosis. Patients with incidental appendicectomy, interval appendicectomy for appendiceal mass, and normal appendix after histologic examination were excluded from this study.
The Alvarado Score (table 1) of the included subjects was retrospectively calculated based on the findings documented on the admission notes, and was classified into low risk (L=1–4), medium risk (M=5–6), and high risk (H=7– 10). The operative findings were classified into uncomplicated appendicitis and complicated appendicitis when there was evidence of perforation, gangrenous change, or abscess formation noticed during the operation. The occurrence of surgical complication (Clavien-Dindo grade IIIb or above) was recorded. The relationships between Alvarado Score and operative findings as well as operative morbidities were analyzed.
Alvarado Score assessment used in the current study
The data were analyzed with standard statistical package (Windows V.21.0). Continuous variables were expressed as medians (ranges) and compared using the Mann-Whitney U test. Categorical variables were compared using the χ2 test. A p value of less than 0.05 was considered to be statistically significant.
Results
The medical records of 364 patients with appendicectomy performed during the study period were reviewed. Forty-two patients who met the exclusion criteria (incidental appendicectomy [n=5], interval appendicectomy for appendiceal mass [n=34], and normal appendix after histologic confirmation [n=3]) were excluded from this study. Another six patients were also excluded due to incomplete data. Of the remaining 316 patients, the median age on admission was 10.8 years (range: 3–18 years). The overall median Alvarado Score was 8.0 (range: 2–10). The percentage of patients having low, medium, and high risk scores was 13.3% (n=42), 20.2% (n=64), and 66.5% (n=210), respectively. Radiologic confirmation of the disease by ultrasound or CT was arranged in 64.2% of the patients (n=203), and there was no significant difference in the utilization rate between the three groups (L vs M vs H=59.5% vs 62.5% vs 65.7%, p=0.59) (table 2).
Summary of patients (N=316) with emergency appendicectomy performed for acute appendicitis between 2006 and 2016
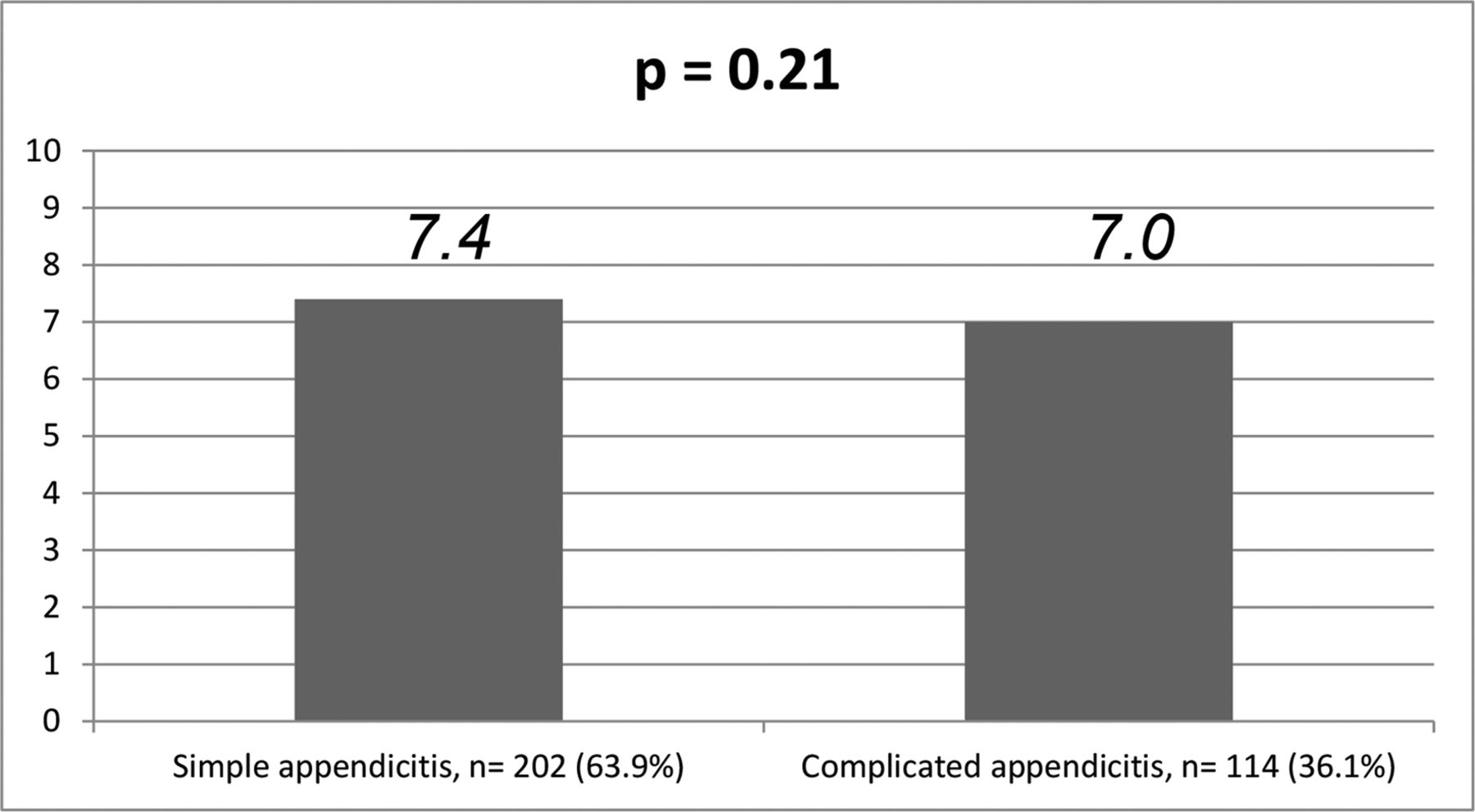
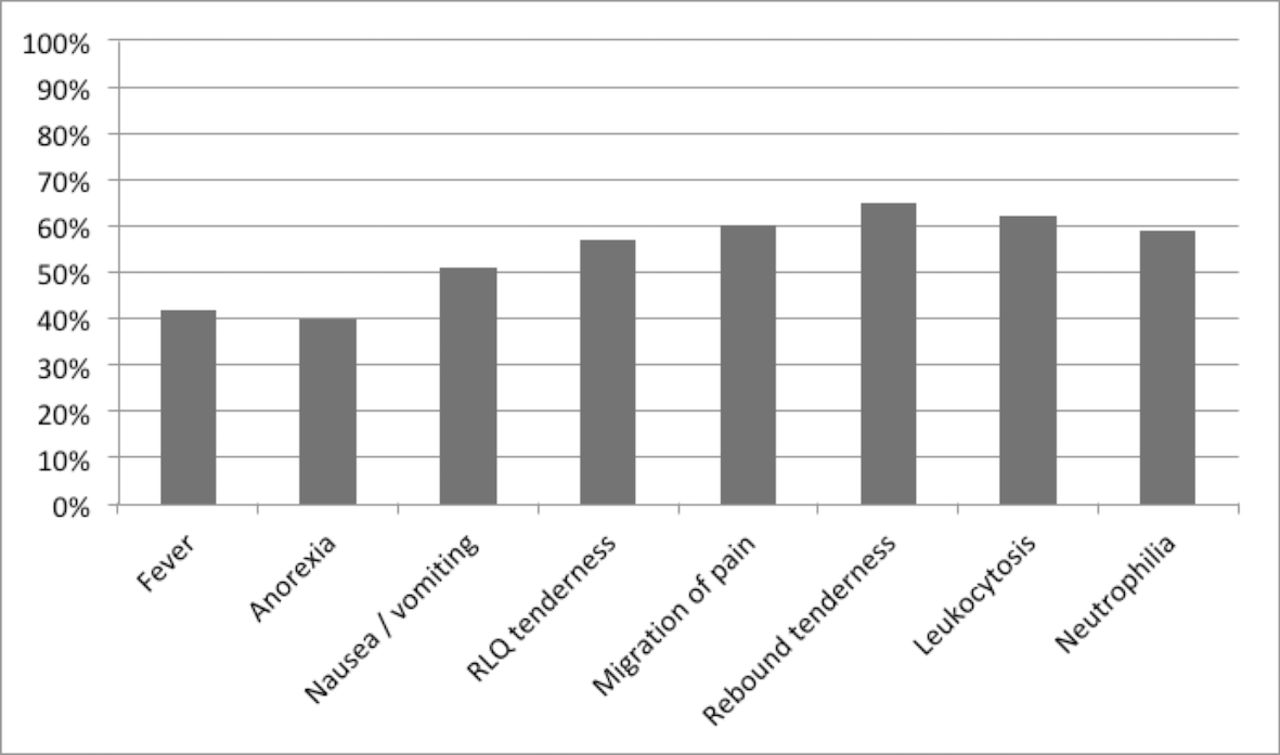
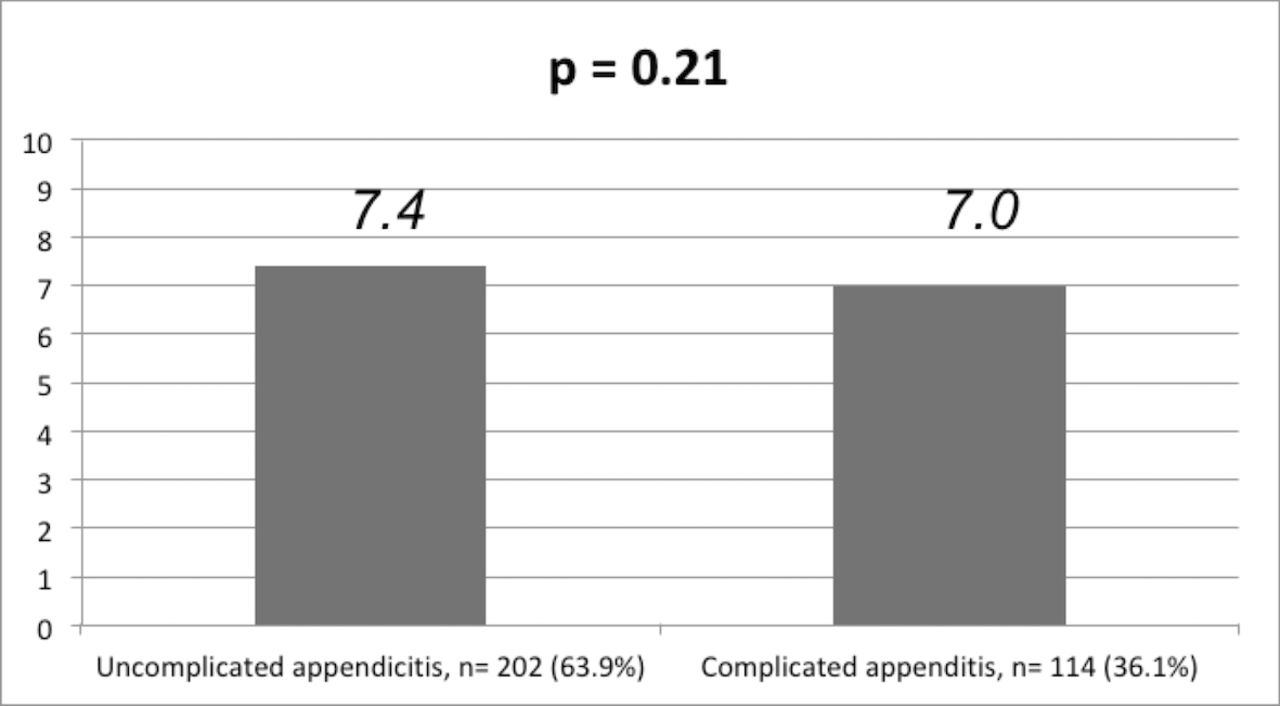
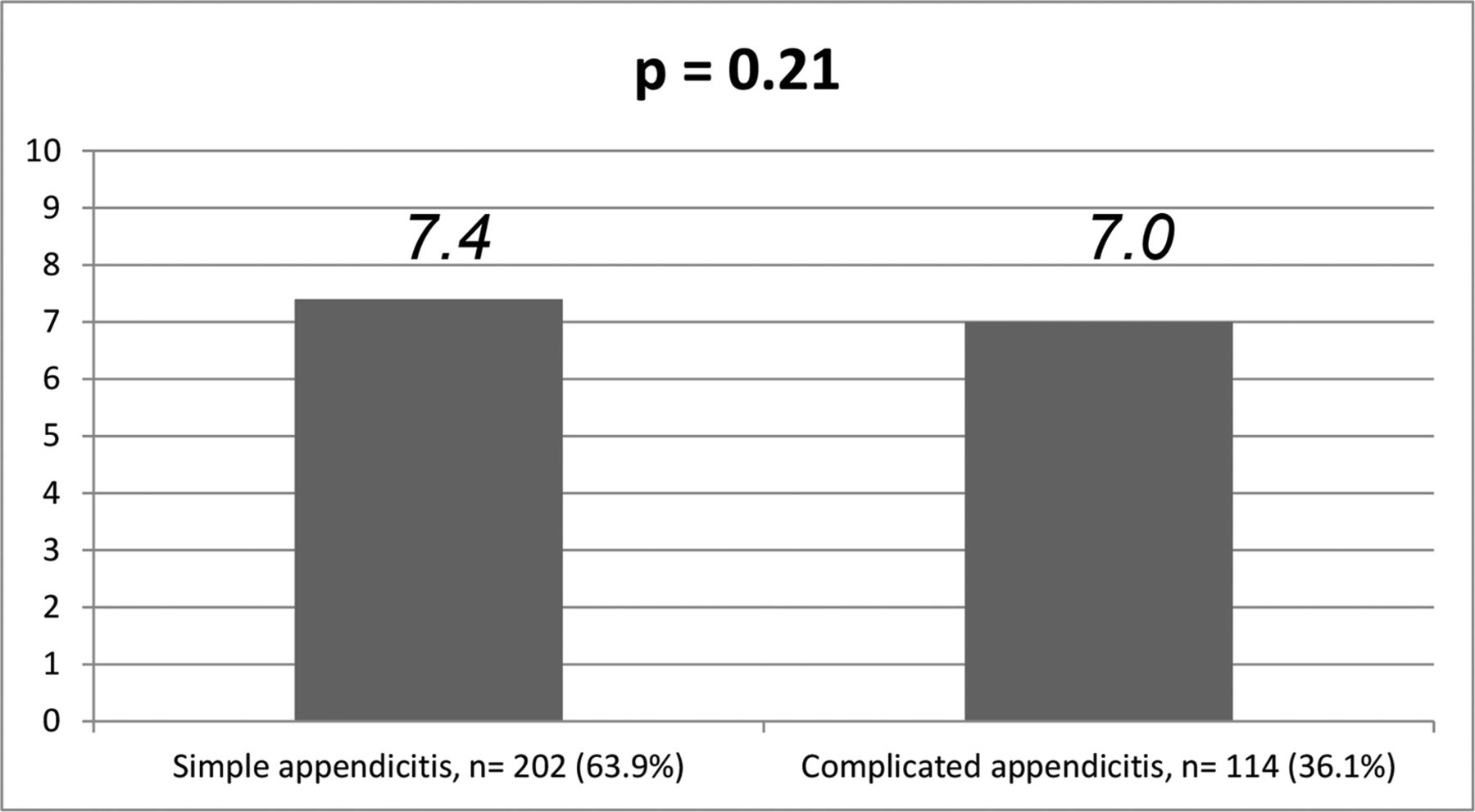
Regarding disease severity, 36.1% of patients (n=114) had complicated appendicitis, and the highest percentage of complicated cases was found in the medium-risk group (H vs M vs L=29.7% vs 61.4% vs 31.0%, p=0.01) (figure 1). The median score was comparable with that of the uncomplicated cases (7.0, range=2–10 vs 7.4, range=3–10, p=0.21) (figure 2). The eight items in the scoring system were analyzed for their sensitivities in predicting complicated appendicitis. Fever, right lower quadrant tenderness, and neutrophilia were found to be the three most sensitive markers (88.6%, 82.3%, and 79.7%) (figure 3). On the other hand, rebound tenderness was found to have the highest positive predictive value (65%) among the eight items to predict cases which have turned complicated (figure 4). The overall postoperative complication rate was 16.5% (n=52), and a higher percentage was found in patients with complicated appendicitis (29.8%, n=34) compared with uncomplicated appendicitis (8.9%, n=18). Regarding the relationship of complication rate and Alvarado Score, a higher median score was found in patients who suffered from postoperative complications (7.7, range=4–10 vs 5.8, range=2–8, p=0.01) (figure 5).

Percentage of patients with complicated disease in low-risk, medium-risk, and high-risk groups.
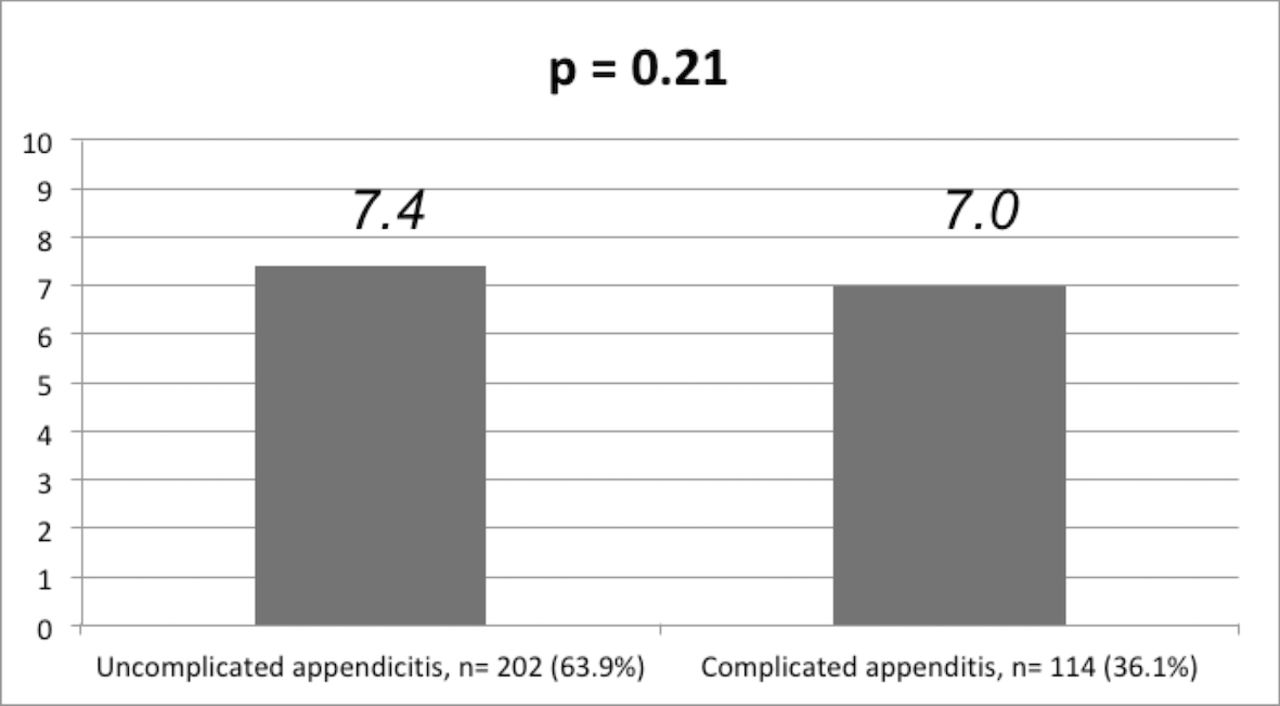
Median Alvarado Score (vertical axis) of patients with uncomplicated versus complicated appendicitis.
Sensitivity of different markers in predicting complicated appendicitis. RLQ, right lower quadrant.
Positive predict value of different markers in predicting complicated appendicitis. RLQ, right lower quadrant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median Alvarado Score (vertical axis) of patients with and without postoperative complications (Clavien-Dindo grade IIIB or above).
Discussion
Although appendicitis is the most common surgical emergency, making the correct diagnosis is sometimes difficult especially in children whose history is sometimes non-specific. The diagnosis is sometimes mistaken as gastroenteritis and results in disease progression. While CT has been widely used in some countries to lower the incidence of normal appendicectomy, its application is associated with radiation and has raised the concern for cancer risk of approximately 20 and 26 per 100 000 men and women.6 7 To solve the problem of diagnostic uncertainty, the Alvarado Score has been developed to assist in the diagnosis of acute appendicitis. This scoring system consists of eight clinical and laboratory assessment items. Previous studies have reported a high sensitivity as well as positive predictive value for diagnosis. However, whether this scoring system can also predict the disease severity and the occurrence of postoperative complication remains undetermined. An accurate prediction of the disease severity allows the surgeon to have a better anticipation for the difficulty of the operation. In addition, this may also give the parents a psychological preparation for the potential problems in the postoperative period.
From the results of this study, only 13.3% of patients with proven appendicitis were classified to have low risk score, and the overall median value for all patients was 8. These two findings suggested that the Alvarado Score should be quite accurate in the diagnosis of appendicitis especially when the score is above 4 (medium or high risk score). Similar finding has also been reported in other studies.2 8–10 However, there are two findings in this study which may suggest that Alvarado Score cannot predict disease severity. First, there was no significant difference in the overall score between patients with complicated and uncomplicated diseases. Second, instead of the patients with a high risk score, those patients with a medium risk score had the significantly highest incidence of complicated appendicitis among the three groups. A postulation to this observation could be related to the partial treatment by antibiotics prescribed by the primary physician or self-purchased in some of the patients with a more severe disease. Indeed, antibiotics alone as the only treatment for acute appendicitis has been widely reported.8 11 12 This might have affected some of their clinical assessments and thus lowered the overall score. Unfortunately, this postulation could not be proven in this study as this information was not always documented on the admission notes. Although the overall score could not predict disease severity, the analysis of individual items revealed that fever, localized tenderness at the right lower quadrant, and rebound tenderness are important clinical features that may suggest the presence of severe appendicitis. Unlike early appendicitis when the pain is mainly visceral in origin, the parietal peritoneum is also irritated in severe appendicitis to give rise to local peritonitis. Therefore, it is expected that the clinical signs of local peritonism, including localized tenderness and rebound tenderness, will become detectable in severe appendicitis. In addition, the measurement of absolute neutrophil count, which is a reflection of bacterial infection, has also been found to have a value in detecting complicated appendicitis. Based on the findings from this study, we recommend that the physical signs of local tenderness and rebound tenderness should be properly examined in any patient with suspected acute appendicitis. If resources allow, the absolute neutrophil count should also be measured in addition to the simple measurement of the leukocyte count. In order to reduce the negative appendicectomy rate, radiologic examinations have been used quite frequently in some centers with ultrasound or CT service. In North America, up to 86% of patients with suspected appendicitis would receive CT prior to surgery.13 While this practice may help to avoid unnecessary operation, it may result in the delay of management. For patients with a medium risk score, we believe they should also receive a prompt surgical treatment by laparoscopy especially in patients with fever, localized right lower quadrant tenderness, and neutrophilia. This is contrary to some of the previous reports which suggested the addition of radiologic examination in this situation.14
In addition to the analysis for complicated diseases, we also study the value of the Alvarado Score in predicting surgical complications. Patients with surgical complications were found to have a significantly higher score than those without complications. Being a retrospective study, a direct causal relationship could not be established, but this association may have an impact on daily clinical practice. In this situation, the operation should be performed by or with the presence of an experienced surgeon. Furthermore, we recommend that more attention should be given to the postoperative recovery in patients who have an initial high Alvarado Score, and a high index of suspicion of postoperative complication is warranted.
There are some limitations and confounding factors regarding this study. Although all the patients were managed by the same algorithm in two sister hospitals, the initial admission notes were written by multiple surgeons and might result in interobserver bias. Patients with appendiceal mass receiving interval appendicectomy were excluded from this study because their original diagnosis could not be confirmed with histologic analysis of the resected specimen. Their exclusion might have inevitably reduced the number of patients with severe disease, but fortunately they are small in numbers.
Conclusion
Alvarado Score does not predict disease severity but is associated with a higher incidence of postoperative complication. Those patients with a high risk score should be closely monitored during the postoperative period. For patients with a medium risk score, they should also receive prompt surgical treatment for the risk of developing complicated disease. Their treatment should not be delayed by radiologic examinations. The physical signs of fever, localized right lower quadrant tenderness, and rebound tenderness may be a signal for complicated appendicitis and should be properly examined. Absolute neutrophil count has a predictive value for severe appendicitis and should be included in the laboratory test for patients with suspected acute appendicitis.
References
Footnotes
Contributors PHYC conceived and designed the study. ZY and KD collected the data. KKYW supervised the study and advised on the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study has been approved by the hospital ethics committee and was done in accordance with the principles outlined in the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors welcome sharing of data from the study.