Article Text

Abstract
Background Multiple chalazia are common in children, and many are treated by surgery. However, the distribution of different types of multiple chalazia has not been studied. This research aimed to investigate the location and number of multiple chalazia in pediatrics who need surgical treatments.
Methods Patients with multiple chalazia treated by incision and curettage surgery (I&C) in a tertiary children’s hospital between June and December 2016 were reviewed. Demographic data, locations, and numbers of chalazia were recorded. Data were analyzed using generalized linear models of the counts and the occurrences of chalazia. Hypotheses were tested using likelihood ratio tests appropriate for each type of data.
Results The study included 128 subjects, most of which were 1–3 years old. The majority of patients had bilateral chalazia (95.3%), and the proportions of patients with internal, external, and marginal chalazion differed dramatically (99.2%, 61.7%, and 2.3%, respectively). The number of internal and external chalazia did not vary significantly with gender, age, or residence of the patients. Internal chalazia were located more frequently in the upper lids (p<0.001). External chalazia showed no preference of localization. The average number of internal chalazia in each eyelid did not relate to the presence of external chalazia.
Conclusions Multiple chalazia are common among younger children in southeast China. The anatomical distribution varies depending on the type of chalazion. Multiple chalazia often occur bilaterally and internally. If doctors are more aware of the anatomical distribution of chalazia, this might result in a higher success rate of I&C.
- Pediatrics
- Ophthalmology
- Surgery, Plastic
Data availability statement
Data are available on reasonable request. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Multiple chalazia are becoming more and more prevalent in children, and they usually need invasive treatments.
Multiple chalazia are usually classified into three types according to the location of lesions—internal, external, and marginal.
Spatial localization and distribution of different types of multiple chalazia in children have not been investigated.
What this study adds
Children aged 1–3 years were more vulnerable to multiple chalazia needing surgery than children aged 3–7 years.
Multiple chalazia were often presented bilaterally and internally. More nodules were located in the upper lids.
No relationship was found between internal and external chalazia for each lid.
How this study might affect research, practice or policy
We recommend everting every eyelid, especially the upper lids in a young patient presenting with chalazion because chalazia tend to be multiple and internal and require careful examination in this age group.
Introduction
Children often develop chalazia, which are lipogranulomatous lumps in the eyelids caused by obstruction of sebaceous glands.1 2 Multiple lumps can occur in an individual. In Bagheri et al’s study,3 11.8% of patients (aged 7–71 years) presented multiple chalazia. Although there were few reports about the incidence rate of multiple chalazia in children, pediatric ophthalmologists have encountered multiple chalazia more and more frequently in clinical settings.4 5
Multiple chalazia are usually classified into three types according to the location of lesions—internal, external, and marginal. An internal chalazion is caused by inflammation of a tarsal meibomian gland that spreads into the conjunctiva. An external chalazion is caused by a plugged sebaceous gland that extends anteriorly to the surface of the palpebral skin and presents as a reddish subcutaneous nodule.6 7 A marginal chalazion arises from an inflamed gland at the eyelid margin.
Conservative treatments commonly include warm compress, topical antibiotics or steroids. There are some problems of applying conservative treatments in children. For example, young kids may not cooperate well with warm compress, it is difficult to apply topical eyedrops, and long-term use of steroids may increase the risk of glaucoma, cataract or infection. Incision and curettage (I&C) surgery will be needed if conservative treatments are ineffective or poorly performed. In addition, an early I&C should be considered when astigmatism or cosmetic problems occur in the patients with some types of chalazia.8–13
Because children tend to present multiple chalazia and may not be able to cooperate well during examination, surgeons might miss some nodules in clinical examination, with subsequent increase in the recurrence rate or the possibility of requiring another general anesthesia for repeating I&C. Thus, for patients with multiple chalazia, analyzing the location of the three types of chalazia is important for the timing of surgery and for complete incision during I&C.
Nevertheless, previous studies relevant to the location of chalazia are limited or dated. In Herman et al’s study (published in 1951), 1693 patients from children to elderly showed a prevalence of chalazia in the lower lids, especially for the right eye.14 In Mustafa and Oriafage’s study, they reviewed 26 pediatric patients aged 3–16 years old with no more than two chalazia and reported that lesions were usually located in the upper lids.15 Ben et al reported a high occurrence of chalazion in the right upper lid (RUL) in adult patients who had planned to receive triamcinolone injection, but whether the chalazion was single or multiple was not mentioned.16 In Knezevic et al’s study, the right lower lid (RLL) was the most commonly affected site in a group of patients above 16 years old who received botulinum toxin injection for chalazion treatment; however, cases with infected nodules or small lesions less than 2 mm were excluded.17 Wu et al reported a higher frequency of chalazia in the left upper lid (LUL) in adult patients but excluded those with multiple chalazia in a single lid.18 Overall, few literature have targeted on pediatrics with multiple chalazia.
The aim of our paper was to use an optimized statistical scheme to investigate the distribution and relationship of three types of chalazia in pediatrics with multiple chalazia that required I&C surgery based on a tertiary children’s hospital in southeast China.
Methods
Study population
Children younger than 18 years of age, who presented with multiple chalazia and received I&C surgery in the department of ophthalmology, Children’s Hospital, Zhejiang University School of Medicine between 1 June 2016 and 31 December 2016, were reviewed retrospectively. These patients were assumed to be a representative sample of children with multiple chalazia in southeast China. Our research adhered to the tenets of the Declaration of Helsinki.
Exclusion criteria
We excluded patients who received chalazion incision in the outpatient clinic just before admission or whose chalazion spontaneously ruptured before I&C. We also excluded patients with eyelid lesions caused by idiot facial aseptic granuloma, acne, seborrhea, rosacea or atopy.
Ocular evaluation
An internal chalazion was diagnosed as a firm and purplish palpable nodule on the conjunctiva when the eyelid is everted. Sometimes a chronic internal chalazion could present as a pedicled granuloma and exceed the palpebral fissure. An external chalazion was diagnosed as a red, elastic nodule with well-defined borders on the surface of the eyelid skin. A marginal chalazion was diagnosed as a small reddish bump, which was usually 1–2 mm in size along the eyelid margin. Because it was difficult to count every nodule, especially tiny internal ones in a small child with poor cooperation, the location as well as the exact diagnosis of chalazion were determined intraoperatively with eversion of every eyelid by one senior ophthalmologist (XYZ) and a surgical assistant (TYW or SJZ). Diagnosis was then confirmed by pathological examination.
Clinical managements for chalazion
Patients with chalazion were recommended to have warm compresses on lids four times a day. Tobramycin-dexamethasone (Tobradex; Santen, Japan) or fluorometholone 5 mg/mL (Flumetholone; Santen, Japan) eye drops were sometimes given with close monitoring of intraocular pressure. If the nodules were painful or accompanied by purulent discharge, levofloxacin eye drops 5 mg/mL (Cravit; Santen, Japan) four times a day would be given. If the eyelid was highly inflamed, the nodules ruptured, patients had fever, or a routine blood test before surgery showed elevated white blood cell counts, oral azithromycin 10 mg/kg (Zithromax; Pfizer, USA) once a day for 3 days would be added. For lesions unresponsive to conservative treatments, lasting for more than 2 months, or showing potential visual or cosmetic risks, I&C surgeries under general anesthesia were performed. The specimens were submitted for histopathology examinations to confirm the diagnosis.
Data collection
To allow accurate counting of the lesions, we included only patients that underwent I&C under general anesthesia which allowed the surgeons to evert all eyelids to count the number of chalazia. Some lesions were adjacent to each other, integrated or overlapped. We counted adjacent or overlapped lesions separately and counted integrated lesions as one. We collected the following information for analysis: age, gender, place of residence (city vs country), type of chalazion, number and location of lesions, duration of presence of chalazion, and medical/ophthalmic history.
Statistical analysis
Statistical analyses were performed using R software V.4.0.2 (Vienna, Austria. https://www.R-project.org/). We analyzed the counts of chalazia using two classes of statistical models, one for the total number of chalazia observed at all locations and another for the number of chalazia observed at each location. The latter observations are needed to estimate the anatomical distribution of chalazia. The counts of internal and external chalazia were analyzed separately.
To be more specific, we assumed that the total number N of chalazia at all eyelid locations had either a Poisson distribution or a negative binomial distribution, whose mean µ was allowed to differ among patients of different gender, age category, or residence. That is, we assumed either

where log(µ) = β’’X specifies the mean as a function of observed covariates X and their effects β, or

where α is a positive, scalar-valued parameter that indicates the level of extra-Poisson variation in N . Our choice of Poisson or negative binomial models was based on an assessment of goodness of fit.
To estimate and make inferences about the anatomical distribution of chalazia, we conditioned on N and assumed the following model:

where Y1, Y2, Y3 and Y4 denote the numbers of chalazia observed at each of four eyelid locations (RUL, RLL, LUL, and LLL, respectively) and where p1, p2, p3, and p4 denote parameters for the proportions of N counts found at each eyelid location. Because this model conditions on the total count N (= Y1 + Y2 + Y3 + Y4), the parameters are necessarily restricted such that 1 = p1 + p2 + p3 + p4. Therefore, only three of the parameters are free to be estimated; the fourth parameter is estimated by difference.
We used the method of maximum likelihood to estimate the parameters of these models from data. We also used likelihood-ratio tests to assess the significance of effects of covariates on N and to examine alternative hypotheses about the anatomical distribution of chalazia.
To examine the co-occurrence of internal and external chalazia, we compared the number of internal chalazia per eyelid for two groups of patients, those with one or more external chalazia and those without external chalazia. More specifically, we assumed the following model:

where Yi,j denotes the number of internal chalazia in the jth eyelid location (j=1, …, 4) of the ith patient. The parameter λi,j denotes the number of internal chalazia that are expected in the jth eyelid of the ith patient given that external chalazia were present (xi,j=1) or absent (xi,j=0). Formally,

This parameterization of the model implies that β1,j is the logarithm of the mean number of internal chalazia in the jth eyelid of patients with external chalazia. The parameter β0,j corresponds to the same quantity, but for eyelids without an external chalazion. We tested the null hypothesis that β0,j = β1,j to assess whether numbers of internal chalazia depended on the presence or absence of external chalazia.
All the statistics were reported as two-tailed probabilities, with p<0.05 being regarded as significant.
Results
Subject characteristics
A total of 128 consecutive children with multiple chalazia were included in the study. No patients met the exclusion criteria. All the histopathological evaluations confirmed the diagnosis of chalazion by showing inflammatory granuloma with multinucleated cells and infiltration of neutrophils and lymphocytes.
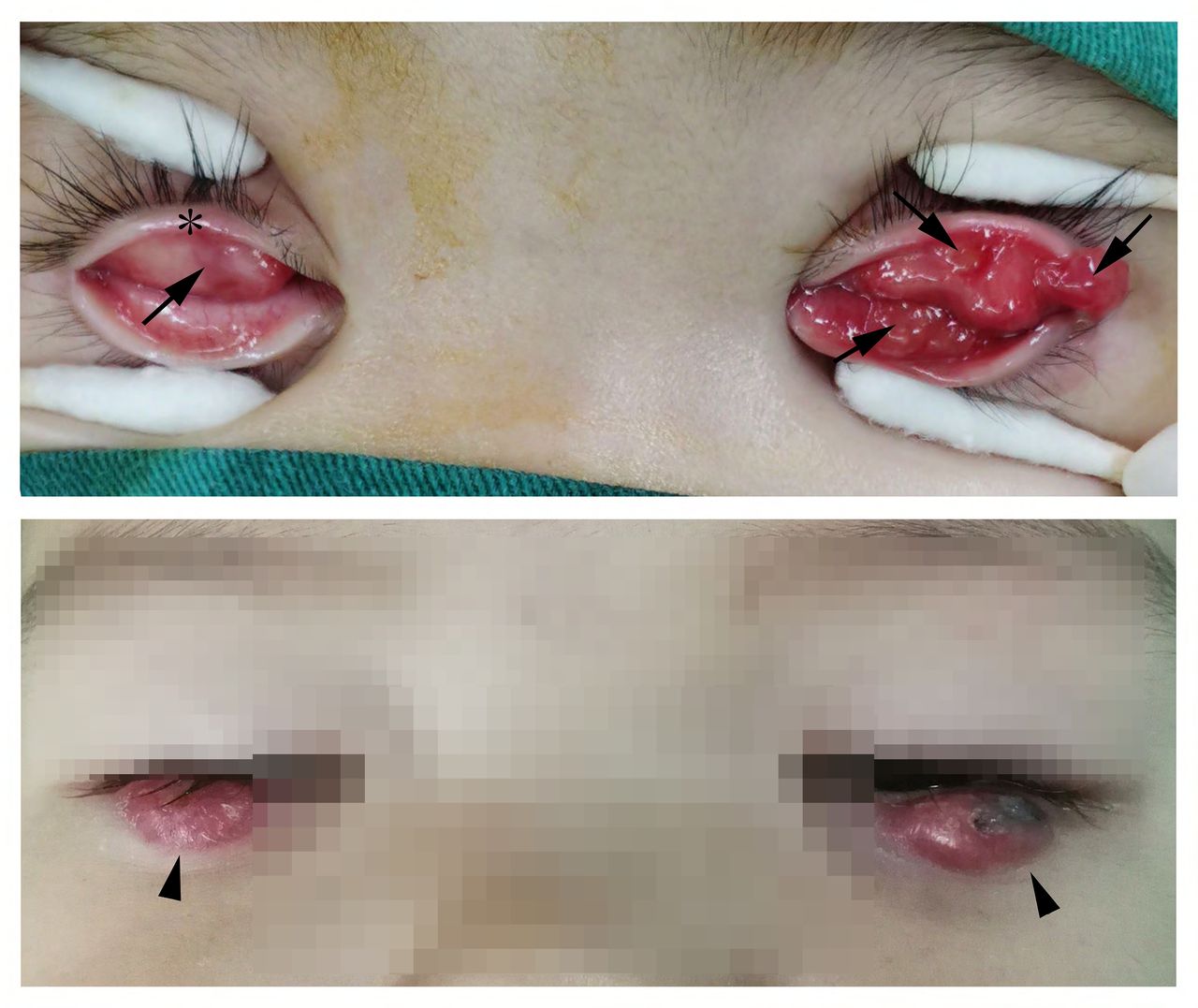
The majority of children (74.2%) were under 3 years old, with a mean±standard deviation (SD) age of 2.5±0.9 years (range 1.0–6.5 years). The mean±SD disease duration was 2.2±1.7 months (range 0.3–12.0 months). Fifty-seven patients were male (44.5%), 122 had bilateral lesions (95.3%), 127 presented internal chalazion (99.2%), 79 external chalazion (61.7%), and 3 marginal chalazion (2.3%). The mean±SD number of lesions per person was 8.30±3.75 (range 2–22). Typical examples of multiple chalazia are shown in figure 1.
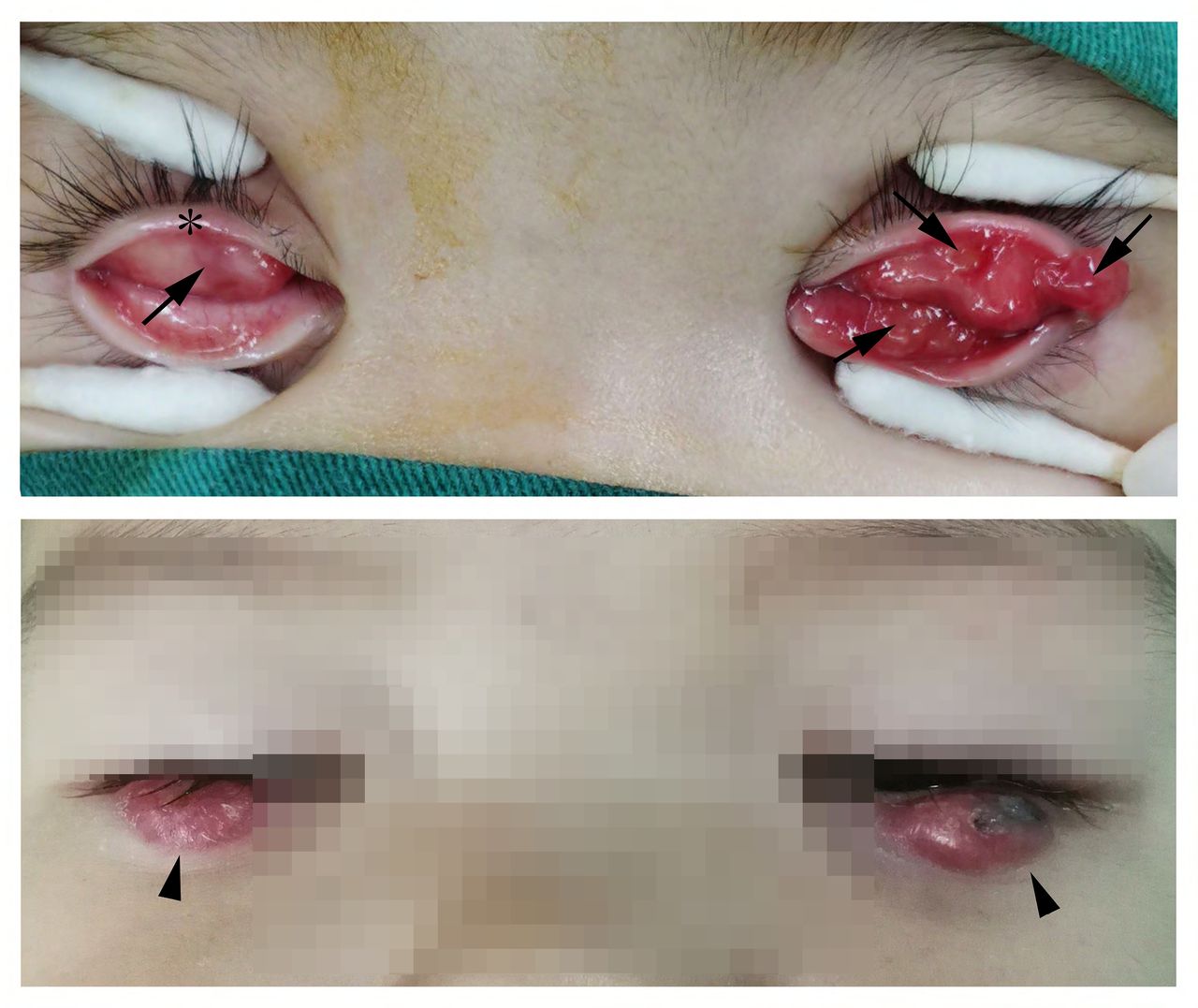
Typical manifestations of multiple chalazia in children, showing internal chalazion (arrow), external chalazion (arrow head), and marginal chalazion (asterisk). Parental consent of the patient in figure 1 was obtained.
Distribution of internal chalazia
A negative binomial distribution with mean  =7.42 and overdispersion
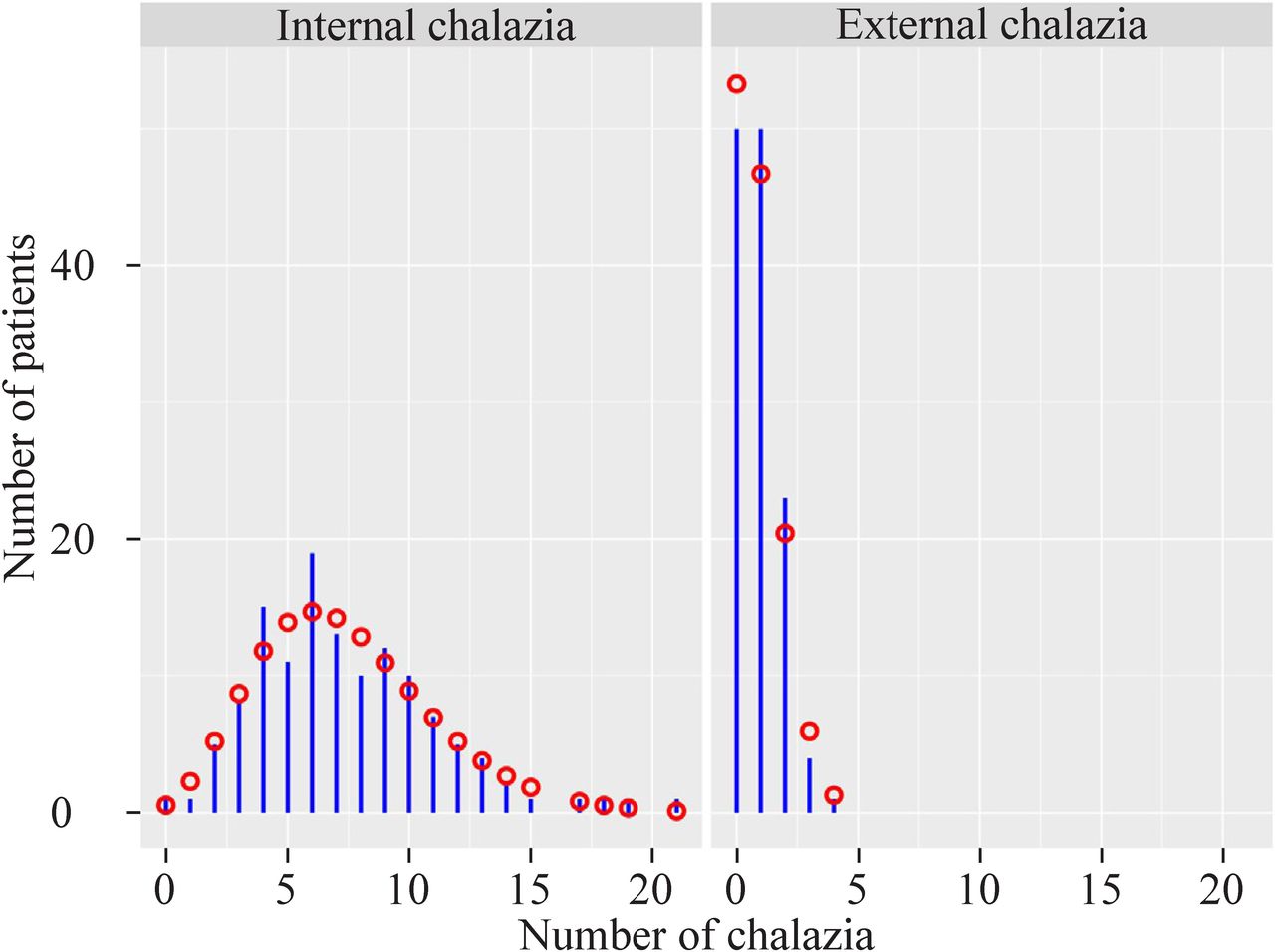
=7.42 and overdispersion  =9.06 provided a reasonably good fit to the observed numbers of chalazia (p=0.137, figure 2). The mean±SD numbers of internal chalazia was 7.42±3.73 (range 0–21). The total number of internal chalazia did not differ significantly with gender, age category, residence or any combination of these covariates (p=0.073, table 1).
=9.06 provided a reasonably good fit to the observed numbers of chalazia (p=0.137, figure 2). The mean±SD numbers of internal chalazia was 7.42±3.73 (range 0–21). The total number of internal chalazia did not differ significantly with gender, age category, residence or any combination of these covariates (p=0.073, table 1).
Demographic distributions and different types of chalazia
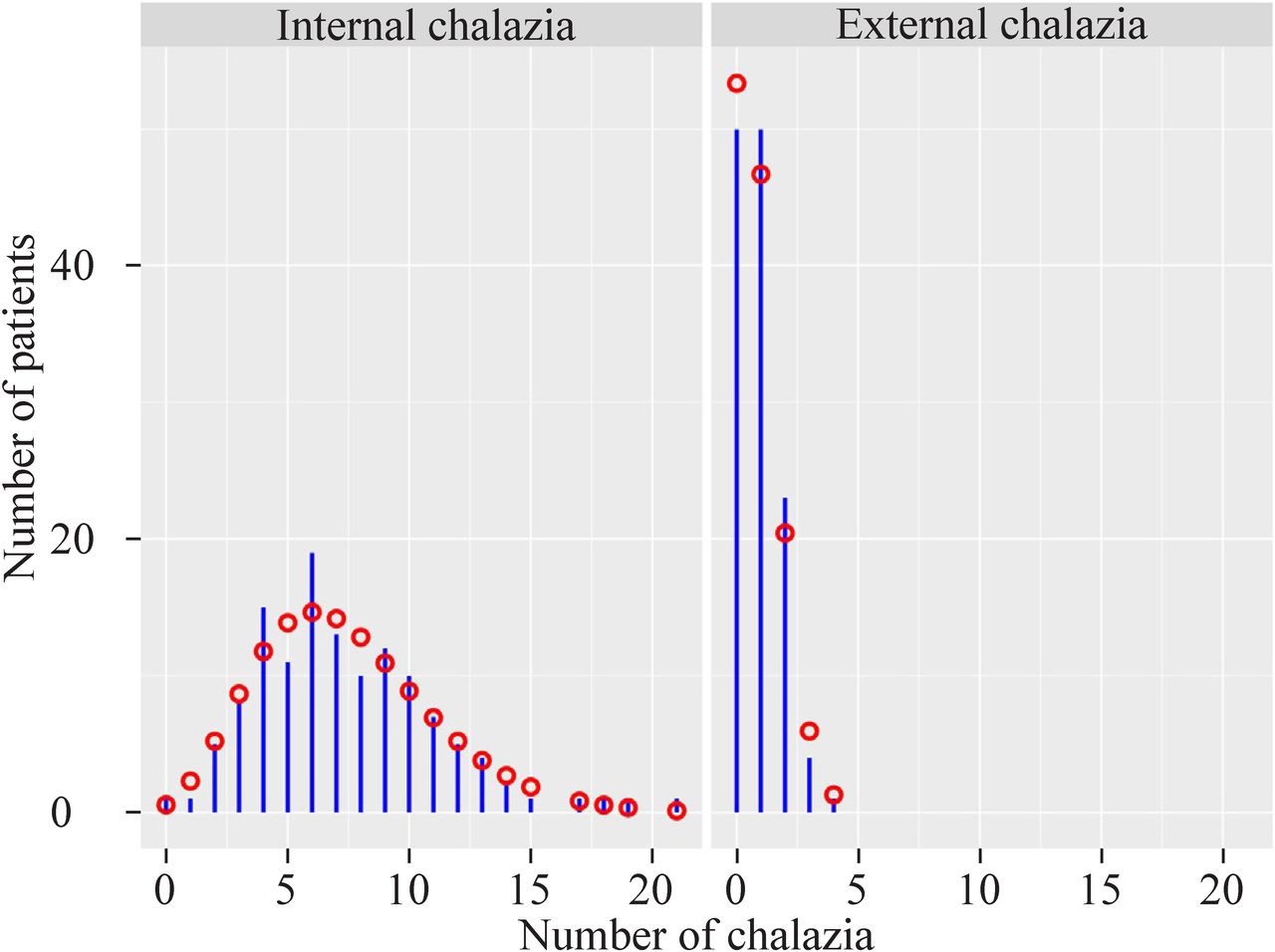
Distributions of the total number of chalazia observed among 128 patients. Circles indicate the expected numbers of chalazia based on the fit of a negative binomial model (internal chalazion) or a poisson model (external chalazion).
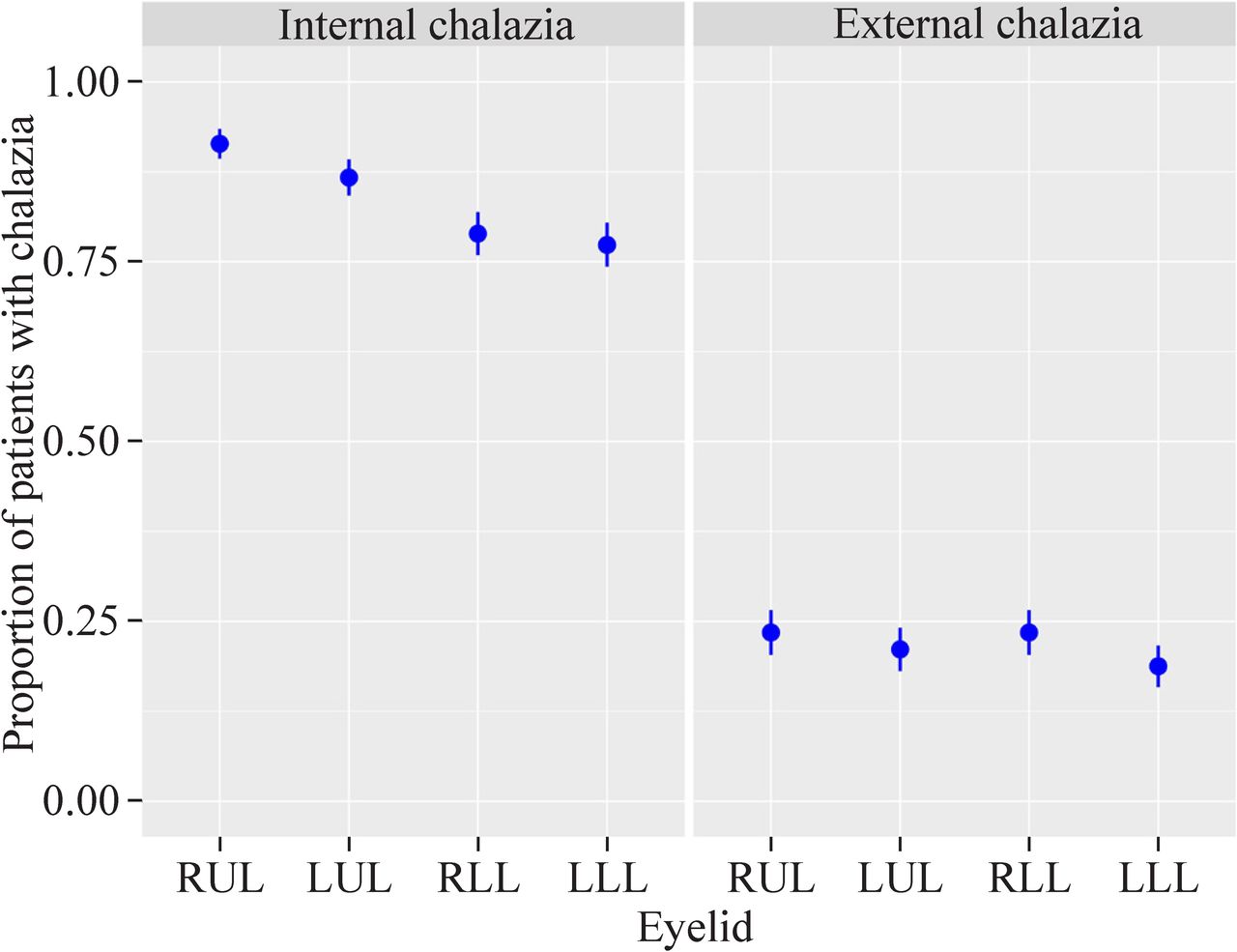
Estimates of the anatomical distribution of internal chalazia revealed a distinct pattern (table 2), wherein the proportion of chalazia located in the upper eyelids was significantly higher than that located in the lower eyelids (p<0.001, figure 3), and there were more patients with chalazia in RUL (91.4%), followed by LUL, RLL, and LLL (figure 4).
Details of lid distributions with respect to different chalazion types
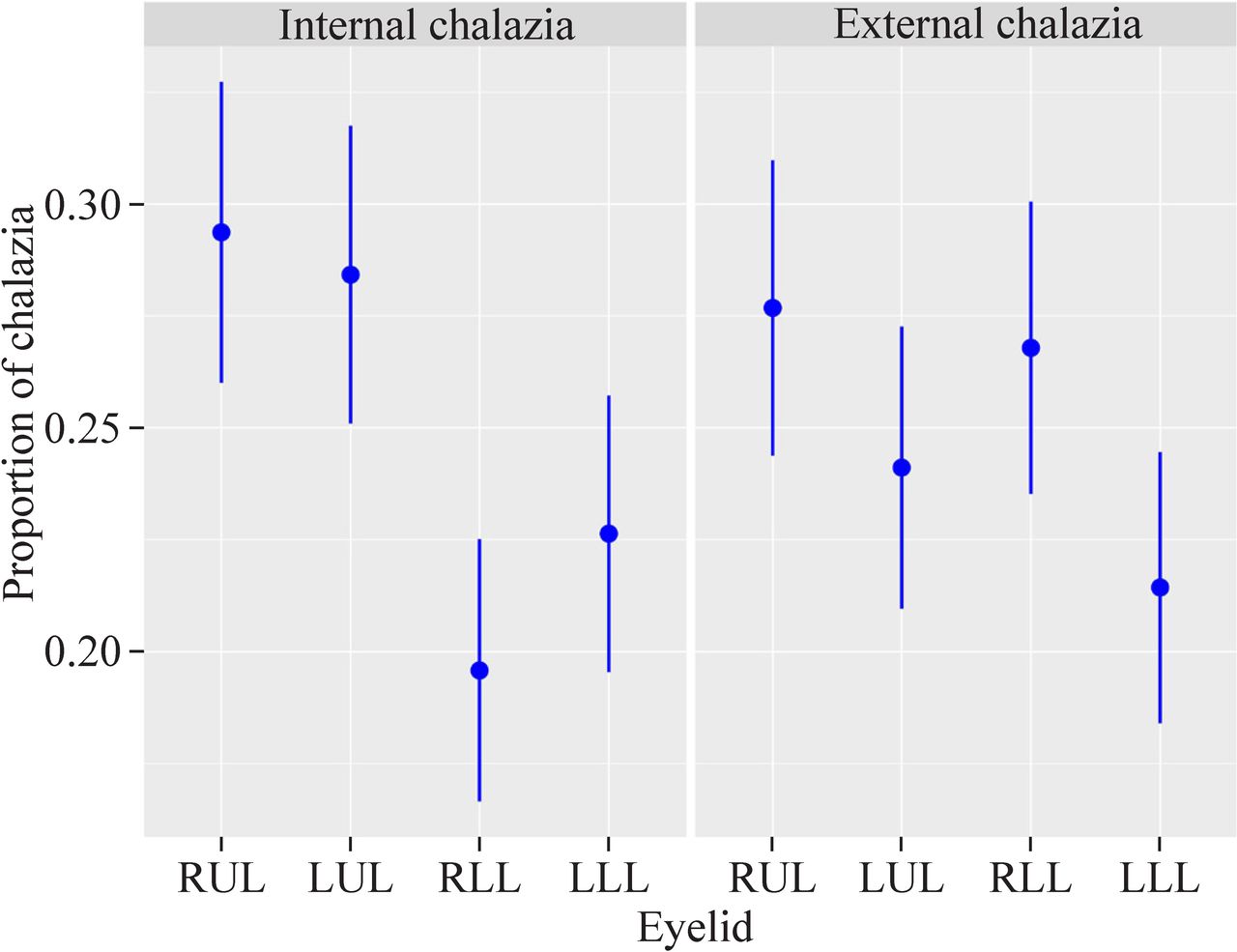
Estimates (with 95% CI) of the anatomical distributions of internal and external chalazion. CI, confidence interval; LLL, left lower lid; LUL, left upper lid; RLL, right lower lid; RUL, right upper lid.
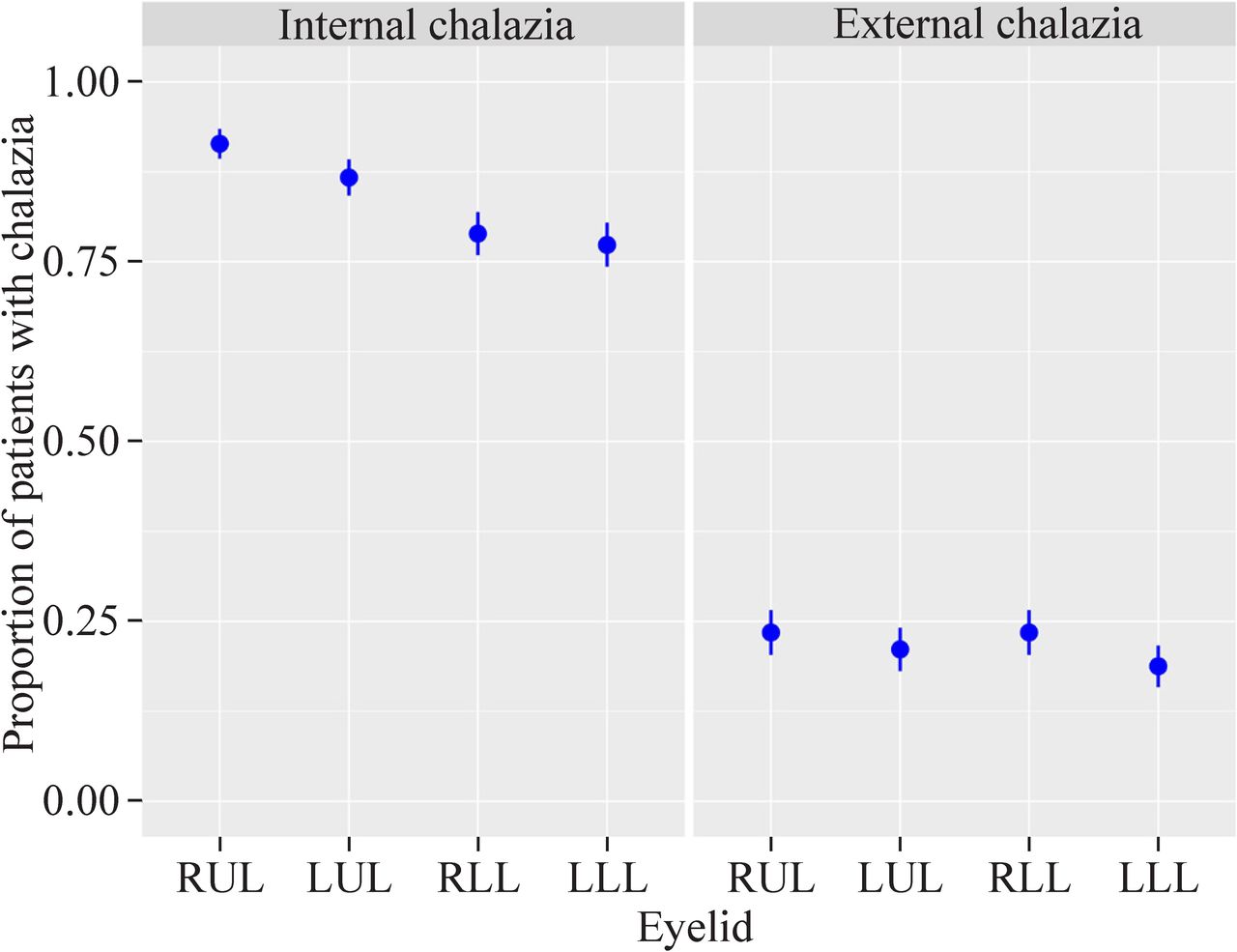
Estimates of the proportion of patients with internal and external chalazion. LLL, left lower lid; LUL, left upper lid; RLL, right lower lid; RUL, right upper lid.
Distribution of external chalazia
A Poisson distribution with mean=0.88 provided a reasonably good fit to the observed numbers of chalazia (p=0.383, figure 2). The mean±SD numbers of external chalazia per person were 0.88±0.87 (range 0–4). The total number of external chalazia did not differ significantly with gender, age category, residence or any combination of these covariates (p=0.280; table 1).
There were more patients with one or more external chalazia than those who had none (61.7% vs 38.3%, figure 2). Among those with presence of external chalazia, at most three lids were involved by external chalazia, and single lid involvement was most common (39.1%). The majority of patients in our study had no more than one external chalazion on each eyelid, except for one patient with two external chalazia on one eyelid. Estimates of the anatomical distribution of external chalazia revealed no significant differences among eyelid locations (p=0.581; figure 3), and there was no difference between the four lids with respect to the proportion of patients with external chalazion (figure 4).
Co-occurrence of internal and external chalazia
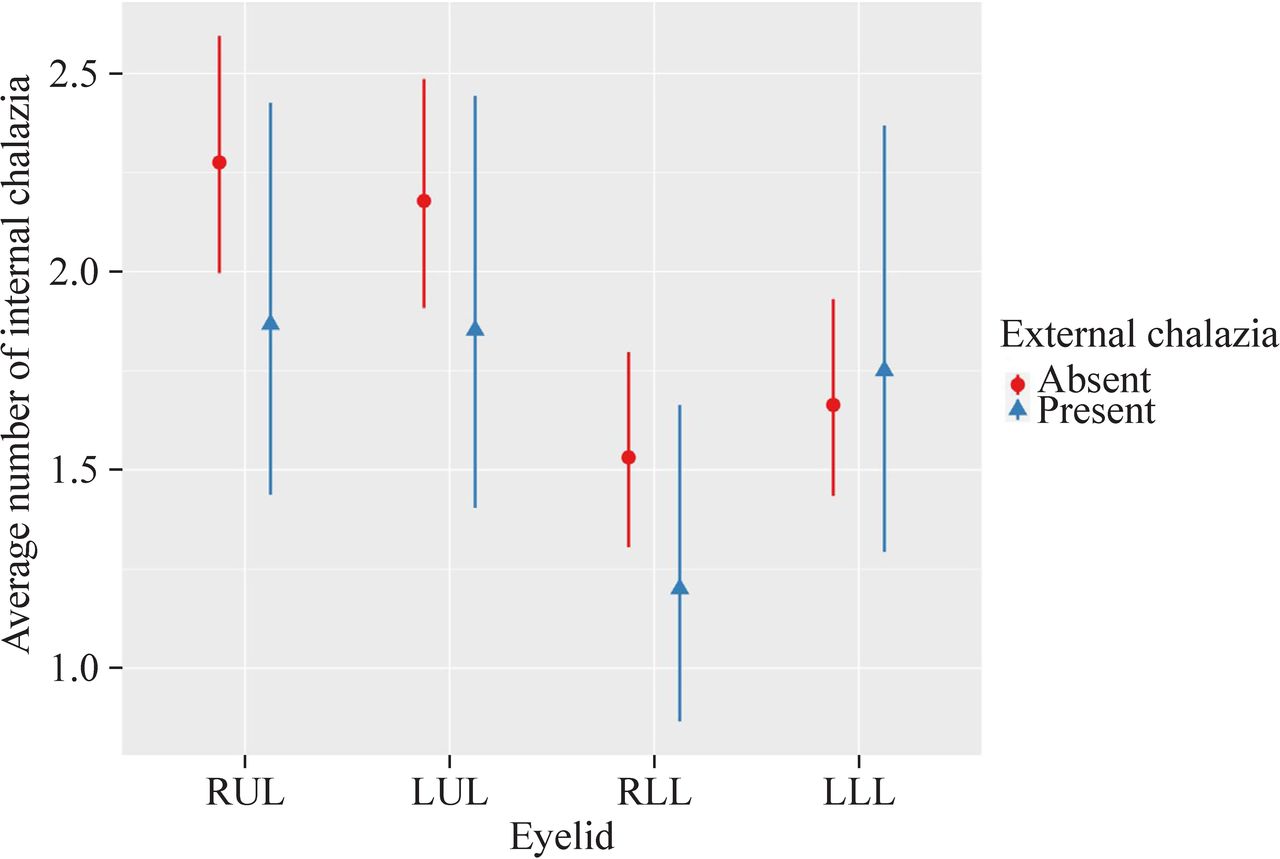
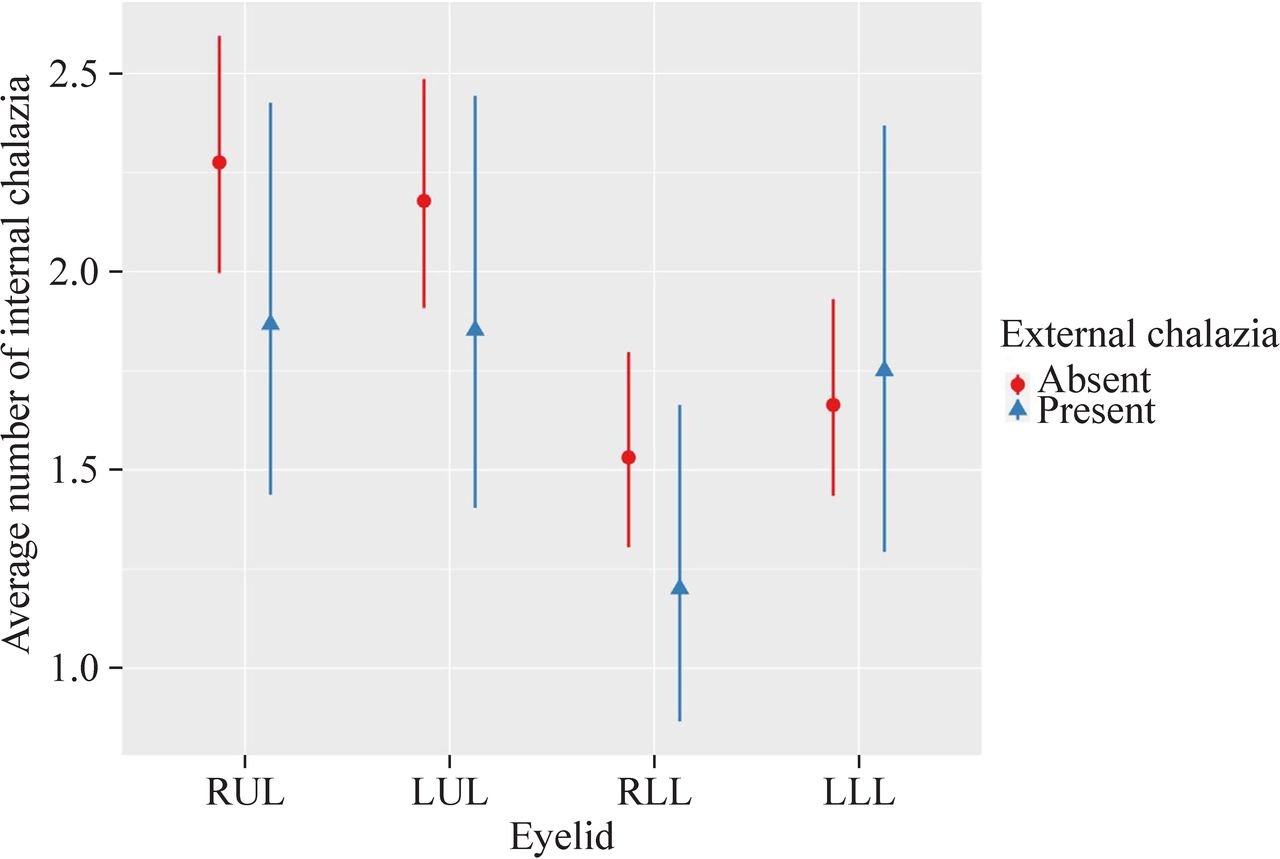
The number of internal chalazia was unrelated to the occurrence of external nodules (p=0.424). To be more specific, in each eyelid, the mean number of internal chalazia did not differ significantly between eyelids with external chalazia and eyelids without (p=0.177, 0.179, 0.292, and 0.769 for RLL, LLL, RUL, and LUL, respectively). The result is shown in figure 5.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimates (with 95% CI) of the average number of internal chalazion in eyelids where external chalazion were absent (red circle) or present (blue triangle). CI, confidence interval; LLL, left lower lid; LUL, left upper lid; RLL, right lower lid; RUL, right upper lid.
Discussion
In the present study, we demonstrated that multiple chalazia that need surgical treatment were prevalent in Chinese young children. The mean number of lesions per person was 8.3. Bilateral chalazia and internal chalazion were most common, external chalazion occurred in more than half of the patients, and marginal chalazion was relatively rare. In addition, the abundance of internal chalazia in upper lids was higher than that in lower lids, whereas the abundance of external chalazia was similar in each eyelid.
Nemet et al demonstrated a high incidence of chalazion in people from urban areas and in females aged from 10 to 29 years.19 Chen et al found that the proportion of multiple chalazia was significantly higher in younger children (6 months to 6 years of age) compared with older children (7–12 years of age).5 Wagner mentioned that children with multiple and bilateral chalazia were often between 3 and 5 years old.4 In our study, multiple chalazia were more common in children aged 1–3 years than in those aged 3–7 years; however, the number of multiple chalazia did not differ by gender, age category or residence groups. The reason that multiple chalazia were more prevalent in younger children than in older children may be due to decreased serum vitamin A in the younger group, and the consequent keratinization of the ducts of the meibomian glands.5
The anatomical distribution of internal chalazia correlates with the characteristics of meibomian glands. Shirakawa et al studied the meibography of Japanese children (aged 1 month to 12 years) and found the numbers of meibomian glands in the upper and lower tarsal plates were approximately 26.9 and 22.0, with no statistically significant difference.20 However, the upper lid had much denser, thinner, and longer meibomian glands,20 21 which were supposed to be the main anatomical traits responsible for the higher numbers of internal chalazia in upper eyelids. Our study showed that bilateral upper lids presented 1.4 times more internal lesions than the lower lids.
Compared with internal chalazia, the proportions of patients with external and marginal chalazia were lower (99.2% vs 61.7% and 2.3%), the number of external lesions per patient was smaller (7.4 vs 1.0), and the anatomical distribution of external type showed no difference between the lids (p<0.001 vs p=0.581). Little information is available on the precise number of Zeis glands. However, given the Zeis gland opens into eyelash follicles and that there are more upper eyelashes than lower eyelashes,22 we speculated that more Zeis glands should be present in the upper lids although we did not demonstrate a higher proportion of external chalazia in the upper lids. The anatomical distribution of external or marginal chalazia totally differs from that of internal lesions. There could be three possible reasons: (1) Compared with the meibomian gland, the Zeis gland is less likely to be plugged due to its shorter duct;23 (2) The sebum secreted by the Zeis gland can inhibit bacterial growth,24 which may play a role in chalazion formation;25 26 and (3) It would be more difficult for a lump from blocked Zeis gland to penetrate through skin than one from blocked meibomian gland to penetrate through conjunctiva because skin is thicker and stronger than conjunctiva. Besides, though a chalazion from meibomian gland could grow big enough to be external, it would more likely extend towards conjunctiva than towards skin because conjunctiva is closer to tarsus and softer than skin.
To our knowledge, the relationship between internal and external chalazion has not been reported previously. Sometimes an external chalazion comes from a growing internal chalazion that penetrates the tarsus and appears superficial on the skin. This can be proven by a hole running through the tarsal plate after the removal of a chalazion. However, our study showed no relationship between these two types of chalazia for each lid, which could indicate that the formation of internal and external chalazion is relatively independent.
Sometimes, doctors may only focus on the eyelid with external nodule or big internal lump that is especially conspicuous when the patient closes his eyes and may overlook the other eyelids that appear to be normal. Though doctors should evert each eyelid for examination during I&C, we still may find hidden internal chalazion in a seemingly normal eyelid that patients or primary care providers have not noticed. The present study highlights the facts that children are susceptible to multiple chalazia and that the nodules tend to grow bilaterally and internally. It should be emphasized that during I&C, especially in young children, an examination of both eyelids, especially the upper lids, should be conducted to detect any internal chalazion.
Our study was the first to describe the detailed anatomical distribution of multiple chalazia in Chinese children. The strength of the study lies in a large sample size focusing on chalazion distribution in young pediatrics whose eyes are difficult to be examined, and our results highlight the importance of examining every eyelid even if it seems to be normal. However, there are some limitations: (1) All the patients in our study came from one hospital in southeast China, and they all underwent I&C operations. Thus, the patients who did not receive surgery under general anesthesia were not included; (2) The subjects included in the present study were all preschoolers because cooperative old children might receive operations in the outpatient clinic; (3) Patients with two or more external chalazia on one lid were quite rare in our study, possibly because parents would opt for early treatment due to cosmesis as soon as they developed external lesions. For the external chalazion, the parents have two extreme attitudes: some people are eager for surgery because the growing external chalazion may cause more significant scar on the lid, while the others believe that spontaneous resolution with conservative management may leave smaller scar than surgical excision; (4) We did not assess the localization of chalazion in the eyelid, such as medial, central or lateral, because the classification is complex if the nodules are large or are adjacent to each other. However, this information is valuable because medial chalazion might lead to canaliculitis, which requires more complicated medical and surgical treatments or even destroys the structure of puncta or lacrimal canaliculi; (5) We did not collect the follow-up results, which would give us recurrence information. In the future, a multicentered study with a longer observation time and better definition of localization would help us learn more about the distribution of multiple chalazia.
In conclusion, among the children who needed I&C, multiple chalazia were more common in patients aged 1–3 years. Different types of chalazion presented different distributional characteristics. Multiple chalazia often occurred bilaterally and internally. Internal lesions were more abundant in the upper eyelids. There was no correlation between the distributions of internal and external chalazia. Our study provides a deeper understanding of the anatomical distribution of multiple chalazia in young pediatrics that need I&C. We would like to reinforce the importance of checking every eyelid, especially the upper lids in a young patient with chalazion, because the nodules tend to grow and multiply internally, therefore requiring careful examination in this age group.
Data availability statement
Data are available on reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of the Children’s Hospital of Zhejiang University, School of Medicine reference number: 2018-IRB-041 Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors XYZ is the guarantor and contributed to writing-original draft preparation and funding acquisition. RMD contributed to formal analysis and writing-review and editing. ZYZ and BNKC contributed to conceptualization, data curation, writing-review and editing. TYW and SJZ contributed to data curation, investigation. All authors read and approved the final manuscript.
Funding This study was supported by the Zhejiang Provincial Natural Science Foundation (No. LSY19H180011) and the Health Department of Zhejiang Province, China (Grant 2016KYA130).
Disclaimer The sponsor or funding organizations had no role in the design or conduct of this research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note This article has a preprint on Research Square (https://www.researchsquare.com/article/rs-37365/v1).