Article Text

Abstract
Background Although fetal ultrasound, fetal MRI and postnatal CT are now widely used in the evaluation of congenital lung malformations (CLM), their diagnostic accuracy remains undefined.
Objective To correlate prenatal and postnatal imaging studies with pathological data after CLM resection.
Design Retrospective, descriptive case series study.
Setting A North American tertiary care centre.
Patients One hundred and three consecutive lung resections for a suspected CLM between 1 January 2005 and 31 December 2015.
Main outcome measures Diagnostic accuracy of imaging diagnosis compared with pathological evaluation.
Results Pathological diagnoses included congenital pulmonary airway malformation ((CPAM) n=45, 44%), bronchopulmonary sequestration (BPS; n=25, 24%), CPAM/BPS hybrid lesions (n=22, 21%) and pleuropulmonary blastoma (n=2, 2%). Fetal ultrasound detected 85 (82.5%) lesions and correctly diagnosed whether or not a lesion was a CPAM in 75% of cases (sensitivity 93%, specificity 32%). Fetal MRI had a similar concordance rate (73%) but was superior in correctly determining whether a systemic feeding vessel was present in 80% of cases (sensitivity 71%, specificity 88%) compared with an ultrasound accuracy rate of 72% (sensitivity 49%, specificity 93%). By comparison, postnatal CT correctly diagnosed whether a CPAM was present in 84% of cases (sensitivity 86%, specificity 77%) and whether a systemic feeding vessel was present in 90% of cases (sensitivity 92%, specificity 88%).
Conclusions Fetal ultrasound remains an important tool in the detection and evaluation of congenital lung malformations. However, it does not correctly predict histology in approximately 25% of prenatally detected CLMs and remains limited by relatively poor sensitivity for systemic feeding vessels pathognomic for a bronchopulmonary sequestration. These data suggest the importance of obtaining additional cross-sectional imaging, preferably a postnatal CT scan, in all patients to help counsel families and to guide in the optimal management of these lesions.
- paediatric surgery
- fetal medicine
- lung
Statistics from Altmetric.com
What is already known on this topic?
Fetal ultrasound and MRI are widely used to characterize congenital lung malformations, but the diagnostic accuracy of these imaging modalities is not well defined.
What this study adds?
Fetal ultrasound detects the vast majority of lung malformations but does not correctly predict histology in approximately 25% of cases. Moreover, ultrasound is limited by relatively poor sensitivity for systemic feeding vessels pathognomic for a bronchopulmonary sequestration. These data suggest the importance of obtaining additional cross-sectional imaging, preferably a postnatal CT scan, in all cases to help counsel families and to guide in the optimal management of these lesions.
Introduction
Congenital lung malformations (CLM) consist of a broad range of rare lung anomalies, including congenital pulmonary airway malformations (CPAM), bronchogenic cysts, bronchial atresia, bronchopulmonary sequestrations (BPS) and congenital lobar emphysema (CLE).1–4 Likely related to improvements in prenatal screening and two-dimensional (2D) ultrasound image quality, the overall incidence of CLMs has increased over the past two decades, and most CLMs are now diagnosed prenatally.5 Based on recent studies, the current frequency of lung malformations may be as high as 1 in 2000 to 2500 live births.6 7
Although a specific prenatal diagnosis can often be made by ultrasound, the overlap and non-specific appearance of the different CLMs can make diagnosis challenging prior to birth. For this reason, the use of prenatal MRI has risen dramatically in recent years and has become the standard of care at many fetal care centres worldwide as a complementary study in the diagnostic workup of CLMs.8–12 More recently, investigators have suggested that a diagnosis by fetal MRI has nearly perfect concordance with findings on pathology,13 while others have argued that MRI may be the best imaging modality to predict perinatal outcome.14 Somewhat surprisingly, however, the comparative diagnostic accuracy of fetal ultrasound and MRI with postnatal CT, the current imaging gold standard, has not been well characterised in a large series of patients with CLM.12 15–19 In this study, we sought to correlate fetal radiological imaging with postnatal CT and pathological diagnosis in suspected CLMs.
Methods
The medical records of consecutive lung resections for a suspected CLM based on preoperative imaging between January 2005 and December 2016 were retrospectively identified (n=103) at C.S. Mott Children’s and Von Voigtlander Women’s Hospital, a major North American fetal and paediatric referral centre. Operative reports, anatomic pathology results and demographic data, including gender, age at resection, prenatal diagnosis and additional comorbidities, were analysed.
For each case, all pertinent prenatal and postnatal imaging studies, except for plain radiographs, were queried from the maternal and paediatric electronic records, respectively. Regardless of prior imaging findings on fetal ultrasound or neonatal plain radiographs, postnatal cases were routinely evaluated by chest CT angiography, using either a 16 or 64 multidetector General Electric scanner (GE Healthcare, Waukesha, Wisconsin, USA) as described elsewhere.20 Briefly, axial and multiplanar reconstructed CT images were reviewed and interpreted prior to resection by board-certified, fellowship-trained paediatric radiologists using a picture achieving and communication system workstation (Horizon Rad Workstation 11.9, McKesson, San Francisco, California, USA).
For all prenatally diagnosed lesions, the initial ultrasound at referral was reviewed using a prospectively maintained database. During the initial ultrasound, 2D images (Philips iU-22, Andover, MA; General Electric Voluson) were recorded and interpreted by one of six fellowship-trained maternal–fetal medicine specialists. The three-dimensional size of the echogenic lesion was routinely measured (in cm) to calculate a CPAM volume ratio (CVR) as detailed elsewhere.5 21 A morphological description of the lesion including location, homo/heterogenicity, echogenicity and signal intensity compared with normal lung was noted. The presence of a systemic vascular supply to the lung lesion was assessed by colour and power Doppler ultrasound. Based on the ultrasound data, a most likely diagnosis (ie, CPAM, BPS, hybrid lesion, CLE, bronchogenic cyst, bronchial atresia, other) was made.
To further delineate the anatomy in larger CLMs and in those with atypical features by ultrasound, selected fetuses also underwent an ultrafast MRI using a 1.5-Tesla Philips Achieva MRI scanner (Philips Healthcare) with a SENSE XL 16-element phased-array torso coil or a 1.5-Tesla Philips Ingenia MRI scanner with a 32-channel phased-array torso coil in the left lateral decubitus or supine position as previously described.22 Axial, coronal and sagittal SSFSE T1-weighted and T2-weighted images relative to the fetus were evaluated and interpreted. Based on the MRI data, a most likely diagnosis (ie, CPAM, BPS, hybrid lesion, CLE, bronchogenic cyst, bronchial atresia, other) was made by one of two paediatric radiologists.
Final pathological diagnosis was retrospectively correlated with initial prenatal ultrasound, fetal MRI and initial postnatal CT results. All values were reported as the mean±SEM unless otherwise indicated. Statistics, including sensitivity/specificity and positive/negative predictive values with 95% CIs, were performed as appropriate using Prism V.6.0 (GraphPad, La Jolla, California, USA). Significance was defined as p<0.05.
Results
Baseline characteristics
Basic demographic data are shown in table 1. Of 103 consecutive lung resections, there were 63 males and 40 females. Seventy were left sided, 33 were right sided and none were bilateral. Three (3.5%) underwent ex utero intrapartum treatment (EXIT)-to-resection for massive CLMs in association with early hydrops at a median gestational age of 36.4 weeks. The median gestational age at birth was 39.0 weeks (IQR 38.0–39.4), and the mean birth weight was 3.3±0.59 kg. Twenty-one (20.4%) neonates had respiratory symptoms at birth. The median age at CLM resection was 6.3 months (IQR 4.3–8.8). The most common pathological diagnoses were CPAM (n=45, 43.7%) and BPS (n=25, 24.3%). Lesions that had histological characteristics of a CPAM in association with a systemic feeding vessel were classified as CPAM/BPS hybrid lesions (n=22, 21.4%). The remaining diagnoses were CLE (n=8, 7.8%) and bronchogenic cyst (n=1, 1.0%). There was one case with both bronchial atresia and CLE. There were two (1.9%) suspected CLM lesions based on CT that were cystic type I pleuropulmonary blastomas (PPB). Both were initially diagnosed postnatally and presented as symptomatic lesions, at 4 months and 2 years of age.
Basic demographic data on congenital lung malformation patients (n=103)
Prenatal detection of lung malformations
Although all mothers reported receiving prenatal care that included a fetal anatomic survey by a local provider, 85 (82.5%) had a fetus with a CLM detected before birth. The median gestational age at initial ultrasound was 22.9 weeks (IQR 20.1–26.0), and the mean initial CVR was 0.77±0.69. The most common ultrasound diagnosis was CPAM without a feeding vessel (n=60, 70.6%, figure 1). A Stocker classification based on ultrasound images was given in 54 (63.5%) cases. There were 22 (40.7%) type I, 15 (27.8%) type II and 17 (31.5%) type III lesions. Mediastinal shift was documented in 25 (48.1%) cases. A systemic feeding vessel was seen in 23 (27.1%) studies (figure 2). Univariate analyses revealed that mothers with private insurance or who had a fetus with a CPAM/BPS hybrid lesion were more likely to be diagnosed prenatally (p<0.009 and p=0.01, respectively). In contrast, CLE and PPB were significantly less likely to be prenatally diagnosed (p<0.001 and p=0.029, respectively; table 2). Six (13.3%) CPAMs were initially diagnosed in the postnatal period.
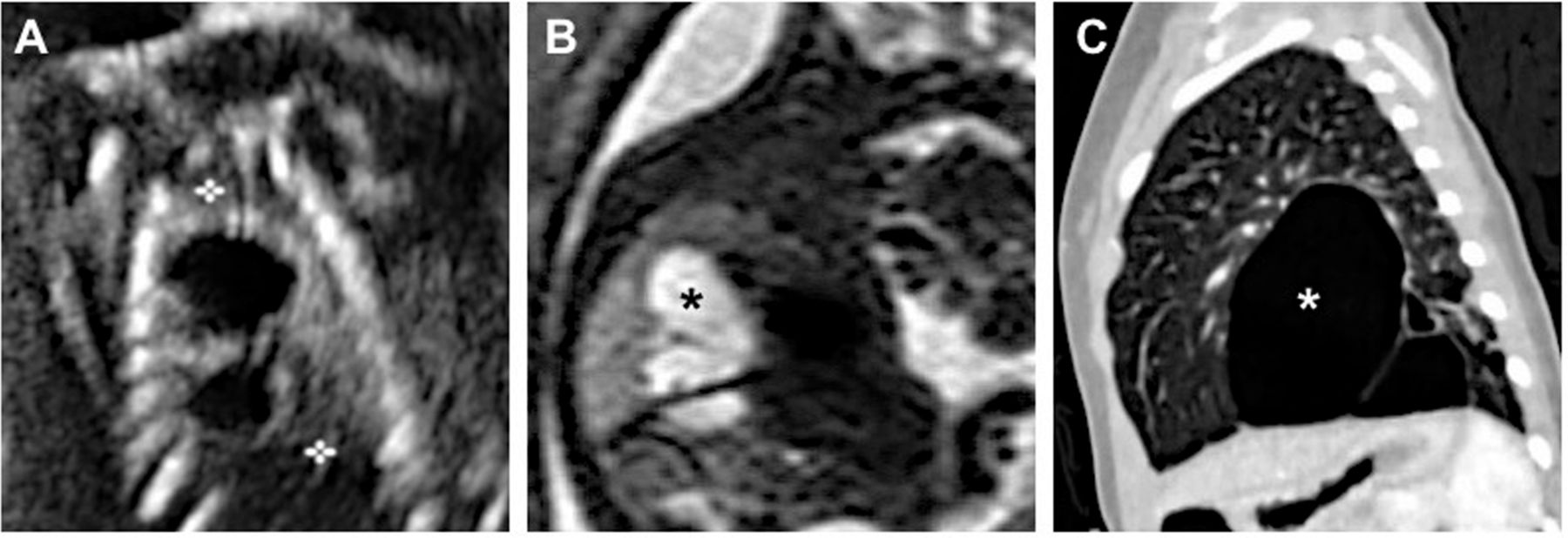
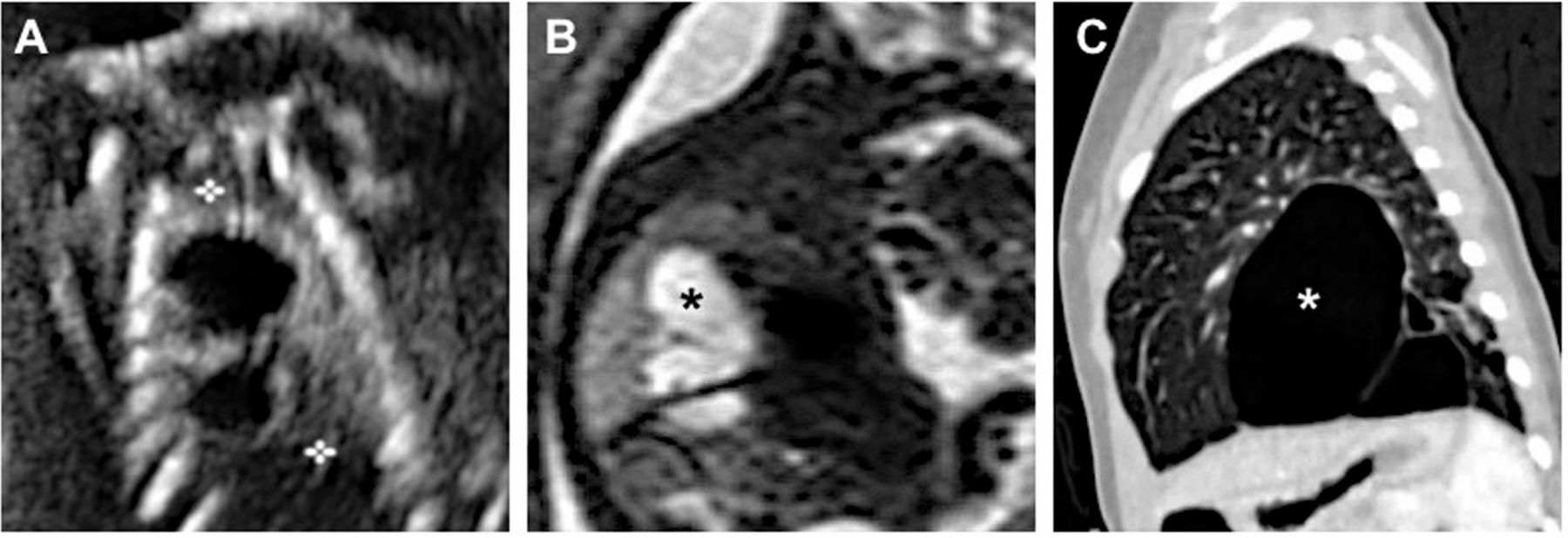
Representative radiological comparison of three imaging modalities in a child with a prenatally diagnosed macrocystic lung malformation. A thoracoscopic lobectomy was performed, and the lesion was confirmed to be a congenital pulmonary airway malformation without systemic blood supply. (A) Sagittal ultrasound image of the fetal thorax at 24-weeks gestation shows a macrocystic lung lesion (between callipers) in the region of the left lower lobe. (B) Corresponding sagittal T2-weighted fetal magnetic resonance image at 32-weeks gestation reveals multiple hyperintense, fluid-filled cysts (asterisk) localised to the left lower lobe. (C) Corresponding sagittal CT reconstruction (lung windows) at 3 months of age demonstrates the same left lower lobe macrocysts (asterisk) in a background of normal appearing lung parenchyma.

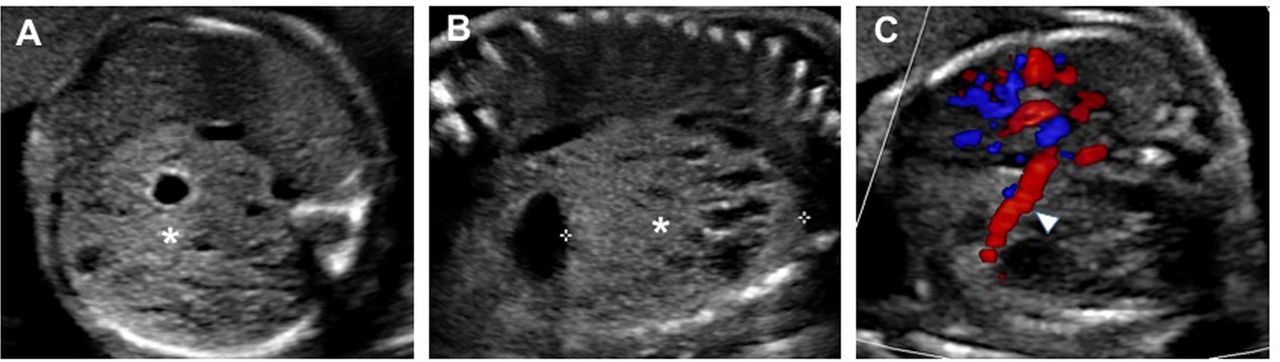
Ultrasound of a 21-week gestation fetus with a hybrid congenital pulmonary airway malformation with systemic blood supply. (A) Axial image of the thorax shows an echogenic lung lesion (asterisk) with macrocysts in the region of the left lower lobe. (B) Sagittal image demonstrates the extent of the same lung lesion (between callipers) with solid (asterisk) and cystic components. (C) On colour Doppler evaluation, an axial view at the caudal aspect of the mass reveals a systemic feeding artery (arrowhead) arising from the aorta.
Prenatal ultrasound detection of resected congenital lung malformations
Fifteen fetal MRIs were performed at a median gestational age of 31.3 weeks (IQR 26.5–32.9), which was significantly different compared with initial ultrasound gestational age (p<0.0001). The most common MRI diagnosis was CPAM without a feeding vessel (n=8, 53.3%), and a systemic feeding vessel was visualised in six (40.0%) CLMs (figure 3). Although there were no differences based on basic demographics and pathological diagnosis between those who had an MRI and those who did not, fetuses that were evaluated by MRI had larger lesions (mean initial CVR: 1.13 vs 0.85, respectively; p=0.063) associated with more mediastinal shift (84.6% vs 35.9%, respectively; p=0.003), maternal steroid use (30.8% vs 7.8%, respectively; p=0.004), hydrops (26.7% vs 5.7%, respectively; p=0.061) and respiratory symptoms at birth (53.5% vs 12.9%, respectively; p=0.002). The additional information acquired by MRI did not influence the prenatal management in any case with the exception of better delineating the anatomy in EXIT cases.

{kind=link}
{kind=link}
{kind=link}
Fetal MRI and postnatal CT of a hybrid lung malformation in the same patient. (A) Axial T2-weighted MRI at 34 weeks gestation shows a hyperintense left lower lobe lung lesion (asterisk) compared with the normal contralateral side. (B) Coronal MRI reconstruction demonstrates the same lesion (asterisk) with a systemic artery flow void (white arrowhead) that arises directly from the aorta. (C) Axial CT (lung windows) at 3 months shows multiple air-filled cysts (asterisk) in the left lower lobe similar to (A), consistent with a congenital pulmonary airway malformation. (D) Coronal CT reconstruction demonstrates the cystic lesion supplied by a large systemic feeding vessel (black arrowhead) arising from the aorta.
There were 92 postnatal CT scans obtained at a median age of 3.3 months (IQR 2.0–5.0). The most common CT diagnosis was CPAM without a feeding vessel (n=40, 43.5%) followed by BPS (n=30, 32.6%). A systemic feeding vessel was visualised in 44 (47.8%) CT scans (figure 3).
Diagnostic accuracy among imaging modalities
Among lesions detected in utero, ultrasound was concordant with the pathological diagnosis of CPAM in 75.3% of cases. The sensitivity and specificity of ultrasound for CPAM were 93% (95% CI 84% to 98%) and 32% (95% CI 15% to 54%), respectively. The positive predictive value and negative predictive value of ultrasound for CPAM were 77% (95% CI 65% to 86%) and 67% (95% CI 35% to 90%), respectively. There were no significant differences between correctly diagnosed and incorrectly diagnosed cases by ultrasound based on gender, lesion side, race, insurance status, gestational age at diagnosis, Stocker type, mediastinal shift, hydrops or CVR.
Fetal MRI had a similar concordance rate (73.3%) for the pathological diagnosis of CPAM. The sensitivity and specificity of MRI for CPAM were 83% (95% CI 34% to 100%) and 67% (95% CI 30% to 93%), respectively. The positive predictive value and negative predictive value of MRI for CPAM were 63% (95% CI 24% to 91%) and 86% (95% CI 42% to 100%), respectively. There was a trend towards MRI as a superior fetal imaging modality for correctly determining whether a systemic feeding vessel was present. MRI had an 80.0% concordance rate compared with 71.8% for ultrasound. For the detection of a feeding vessel, the sensitivity of ultrasound (49%, 95% CI 33% to 65%) was lower compared with that of MRI (71%, 95% CI 29% to 96%), although this failed to reach statistical significance (p=0.75) due to the relatively small number of patients imaged by MRI.
Postnatal CT had a concordance rate of 83.5% of cases with the pathological diagnosis of CPAM. The sensitivity and specificity of CT for CPAM were 86% (95% CI 76% to 93%) and 77% (95% CI 56% to 91%), respectively. The positive predictive value and negative predictive value of CT for CPAM were 92% (95% CI 83% to 97%) and 64% (95% CI 45% to 81%), respectively. For the detection of a systemic feeding vessel, CT had a concordance rate of 90.2%, the highest among all imaging modalities. This rate was statistically significant when compared with that of prenatal ultrasound (p=0.002) but not significant when compared with fetal MRI (p=0.37). The sensitivity and specificity of CT for detection of a feeding vessel were 93% (95% CI 80% to 98%) and 88% (95% CI 76% to 96%), respectively. The positive predictive value and negative predictive value of CT for detection of a feeding vessel were 86% (95% CI 73% to 95%) and 94% (95% CI 83% to 99%), respectively.
Discussion
Obtaining accurate imaging of CLMs is important for paediatric providers for several reasons. First, it allows surgeons to better understand the anatomy, including unsuspecting anomalous vessels, which may be critical for surgical planning and a safe operative resection.15 23 Second, optimal imaging helps to predict lung mass histology and its associated postnatal natural history, which may include recurrent pneumonia, progressive mass effect on adjacent mediastinal structures, pneumothorax, high output cardiac failure and malignant degeneration.2 24 Although we and others have shown that lesion size is a more relevant prognosticator of outcome than histological diagnosis,5 25 26 a reliable prediction of disease pathology can affect clinical decision-making in asymptomatic infants, such as whether to proceed with elective resection versus observation, an alternative management strategy that has gained some traction in Europe and elsewhere.27 28 Finally, accurate imaging can help improve the ability of maternal–fetal providers to deliver concrete, evidence-based information during prenatal counselling discussions with anxious family members.29
In this study, we systematically assessed the diagnostic accuracy of fetal 2D ultrasound, fetal MRI and postnatal CT. To our knowledge and review of the literature, this work is the largest reported radiology–pathology comparative series. The three imaging studies were chosen since they are all commonly used in the routine evaluation of CLMs at tertiary and quaternary care units worldwide. Based on pathological evaluation from each CLM, we found that fetal ultrasound performed well in some areas but clearly had limitations in others. The overall sensitivity of contemporary second-trimester fetal ultrasound imaging for detecting a CLM was respectable given that over 80% of all resected lung lesions were detected prenatally. Moreover, our maternal–fetal medicine specialists were able to reliably diagnose whether or not a lesion was a CPAM by ultrasound in three out of four cases, and the fetal ultrasound concordance rate for identifying a CPAM was statistically comparable to that of MRI. Several investigators have documented the accuracy of ultrasound with concordance rates between 35% and 62% in smaller groups of patients with CLM.15 18 MRI concordance rates ranging from 46% to 98% have been previously demonstrated by other groups.13 16 18
Although we successfully identified all CPAM/BPS hybrid lesions by ultrasound, our data showed an overall low sensitivity of fetal ultrasound for finding systemic feeding vessels (49%), a result that is consistent with some but not all studies.19 30 It is possible that the earlier gestational age at ultrasound and relatively smaller size of fetal ultrasound-imaged lesions could have underestimated its relative diagnostic accuracy. Nevertheless, given the poor negative predictive value of ultrasound for detecting systemic feeding vessels, the clinical implications of these data highlight the importance of obtaining a fetal MRI, or preferably an early postnatal CT scan, to best delineate the anatomy when surgical resection is imminent. Compared with MRI, CT scan had a higher concordance rate for characterising the lung parenchyma consistent with CPAM and was the most accurate study for the detection of a systemic vasculature to the mass. Some paediatric providers may have concerns regarding the risks of CT ionising radiation in infants due to the greater radiosensitivity of their organs and tissues,31 but relatively low doses of radiation can be utilised without sacrificing image quality as described elsewhere.20 32
Our study confirms that fetal ultrasound remains an indispensible screening tool in the evaluation of CLMs. However, in comparison to ultrasound, the acquisition of clear images by MRI is not limited by maternal body habitus, fetal positioning and amniotic fluid volume.9 MRI may yield additional information regarding anatomic location of the lesion due to enhanced soft tissue contrast resolution. However, the utility of MRI in the majority of CLM cases remains controversial since the marginal benefit of MRI for most lesions is questionable, both in terms of increasing risk factor stratification accuracy and facilitating prenatal management.19 33 Our data shown here is congruent with this reported experience since the additional information acquired by MRI did not influence prenatal decision-making in most cases. Therefore, our group, among others, advocate for a more selective role of MRI in CLMs, as indicated based on unclear anatomy by ultrasound or when large lesions are identified by ultrasound. Based on the congenital diaphragmatic hernia (CDH) literature,34 35 MRI may be helpful in CLM management in terms of better estimating the volume of the normal lung parenchyma in larger, more high-risk lesions (eg, CVR >1.6) given that pulmonary hypoplasia and pulmonary hypertension would be a concern at birth.36 Fetal MRI may also be considered in this patient population in lieu of a planned postnatal CT scan given the possibility that large, high-risk lesions are more likely to require earlier surgical intervention, including thoracoamniotic shunting, fetal resection, EXIT-to-resection and early neonatal resection patients in massive respiratory distress.37 38
Despite the aforementioned findings from our comparative study, there are several caveats and limitations that should be acknowledged. First, this was a single institution, retrospective study of CLMs that were resected and submitted for pathological evaluation. As a result, these data may not be generalisable to other institutions where maternal–fetal medicine specialists and radiologists may have more varied expertise with CLM imaging, especially given that ultrasound can be highly operator dependent. Second, the exclusion of certain patient groups may have led to some sample selection bias. For example, some CLMs at our centre (approximately 10%–20%) were managed non-operatively over the study period, and this subset of patients was not included in the analysis given the absence of pathology data required for tissue diagnosis. Since we also did not include fetuses referred for a suspected CLM who were ultimately diagnosed with other thoracic anomalies (eg, CDH), it is certainly possible that fetal MRI may have been critical in excluding alternative diagnoses.9 Third, in contrast to ultrasound and CT, the number of MRIs evaluated was relatively small and interpreted by only two paediatric radiologists. The selective use of MRI for larger lesions at our institution also raises the possibility of selection bias. In contrast, the degree of effort made by the multiple sonographers to identify systemic feeding vessels at the initial ultrasound may have been more variable. Fourth, we did not evaluate the diagnostic accuracy of plain radiographs performed in the postnatal period. Finally, we recognise that the different imaging studies were done in sequence such that all MRI and CT scans were likely interpreted in the context of prior imaging data for a given patient. As discussed elsewhere,39 this bias is well recognised in clinical research and undoubtedly may have been a contributing factor in explaining the higher diagnostic accuracy of subsequent imaging studies. Future research studies that would yield more insightful data on radiology–pathology correlation should focus on direct comparisons among the different imaging modalities in a prospective, blinded fashion.
Acknowledgments
The authors wish to thank the collaborative efforts of Jeannie Kreutzman, RN, MSN, CPNP, of the Fetal Diagnosis and Treatment Center, as well as the Center for Statistical Consultation and Research (CSCAR) at the University of Michigan.
References
Footnotes
Contributors GBM, MCT and SMK contributed to the study conception and design. RAM, KNJ and AH were responsible for the acquisition of data. RAM, ML-T, MCT and SMK performed the analysis and interpretation of data. RAM and SMK drafted the manuscript. RAM, MCT and SMK contributed to the critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This HIPAA-compliant study was approved by the Michigan Medicine Institutional Review Board (#51132)
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The University of Michigan is committed to the open and timely dissemination of research outcomes and will adhere fully to the NIH Statement on Sharing Research Data (http://grants.nih.gov/grants/guide/noticefiles/NOT-OD-03-032.html) and the NIH Grants Policy Statement http://grants.nih.gov/grants/policy/nihgps_2003/index.htm). Research Resources generated with funds from this grant will be readily available in a timely fashion for sharing and distribution to any academic investigators for the purposes of non-commercial research.