Article Text

Abstract
Objective: Almost all children with quadriplegic cerebral palsy (CP) have feeding difficulties. Our aim was to identify the major determinants of feeding-related quality of life (QoL) in children with quadriplegic CP from the perspective of parents and to compare findings with the perceptions of health professionals.
Design: Qualitative cross-sectional study.
Methods: A trained facilitator conducted four semi-structured focus groups with parents (n = 21) of children with quadriplegic CP attending a multi-disciplinary feeding clinic at a paediatric teaching hospital in Sydney, Australia, between November 2003 and February 2005. All sessions were audio- and video-taped. NVivo software was used to facilitate thematic analysis of the transcribed audiotapes and to compare them with data from focus groups conducted by the same research team with health professional participants.
Results: Parental perceptions clustered into the same five themes described by health professionals (parent–child interaction; delivery of health services; the child’s emotional well-being; the child’s physical well-being, and socialisation), but the content of the subthemes and the values attached differed, for example health professionals valued weight gain, whereas parents valued their child feeling loved. Health professionals did not consider the full range of issues important to families. The differences in priorities for treatment outcomes negatively affected the parent–health professional relationship.
Conclusions: Disparities between parents’ and health professionals’ perceptions provide useful insight into communication between the two, identify the range of issues important to families, and highlight the parents’ expert role in assessing the child’s emotional and social well-being. The five themes identified provide a framework for a comprehensive evaluation of the health status of children with quadriplegic CP and feeding difficulties.
Statistics from Altmetric.com
Up to 90% of children with quadriplegic cerebral palsy (CP) experience feeding difficulties.1 2 Lack of self-feeding skills is associated with significant morbidity3–7 and a sixfold increase in hazard for mortality.8 Feeding difficulties are associated with increased support needs, increased parental stress and decreased social participation.9–12
Previous studies have used interviews to explore parents’ experience of feeding difficulties.10 13–19 These studies have focused on children with gastrostomy tubes and explored limited aspects of quality of life (QoL). Importantly, they do not provide a comparison of perceptions of parents and health professionals, who do not always agree in their assessment of QoL or treatment priorities.20–24 In order to understand the full range of effects of feeding difficulties on QoL and also obtain insight into parents’ priorities, it is necessary to examine both parents’ and health professionals’ perceptions.
The aims of this study were to use a qualitative approach (focus groups) to explore parents’ perceptions of the major determinants of feeding-related QoL and to compare these with health professionals’ perceptions (identified in a previous study using the same methodology) to identify possible disparities. This information will provide a framework for evaluating health-related QoL in the clinical setting and could also be used to develop a feeding specific QoL questionnaire for children with quadriplegic CP.
METHODS
Participants
All parents, or primary carers, of a child with quadriplegic CP and feeding problems who attended a multi-disciplinary feeding clinic at The Children’s Hospital at Westmead, Sydney between August 2000 and January 2005, were contacted by phone and invited to participate. Eligibility required sufficient proficiency in English to contribute fully as a focus group participant and was determined by the primary investigator during this initial phone call. The feeding clinic receives referrals for a wide range of children with disabilities and feeding problems from throughout New South Wales. A feeding problem was defined as feeding requiring intervention by medical or allied health teams. Parents of children with and without gastrostomy were included. Ethical approval was obtained from the hospital.
Focus groups
A trained facilitator (the first author) and scribe conducted four semi-structured focus groups. Verbal consent was obtained at the time of recruitment. The questions used to stimulate discussion were open ended (eg, How do you think feeding problems affect your child’s QoL?). Specific questions or prompts were used as required to clarify points raised by participants or to focus the discussion on the topic in hand.25 The duration of each focus group was approximately 2 h and all were recorded by both audio and videotape. The focus groups varied in size (seven, five, four, five). Two focus groups were composed of parents of children who had a gastrostomy (current or past), and two were groups of parents of children who had never had a gastrostomy.
Data were analysed for patterns of interaction between group participants.26 There was strong convergence of opinions across the four groups and informational redundancy (“saturation point”)27 was reached by the third group with no new opinions or themes emerging in the fourth group.
Analysis
The audiotapes were transcribed and then proof read by the first author using the videotapes to check for accuracy and to identify non-verbal cues. The transcribed data were analysed using NVivo v.7 (QSR International, Doncaster, Australia), a software programme developed to facilitate the analysis of qualitative data.28 Passages of text were then coded according to theme using the constant comparative method whereby each piece of data is compared to the rest of the data to establish analytical categories.29 Additional analysis was conducted to explore group dynamics and identify differences in responses according to whether or not the child had a gastrostomy tube. The data were also analysed quantitatively to identify the percent of text coded for each identified theme to provide a measure of saliency.
We also carried out a comparison between themes and subthemes which emerged from the analysis of health professionals’ perceptions with those of parents.30 Data were compared quantitatively for percent of text coded for each theme/subtheme and qualitatively for content.
RESULTS
Between November 2003 and February 2005, 24 potential participants were approached, and of these 21 agreed to participate and were allocated to one of the four focus groups. Participants included mothers (n = 17), fathers (n = 2), a foster mother (n = 1) and one female sibling. Two participants had two affected children. Of the participants, 12 were carers of children who had a gastrostomy (11 current, one previous), and nine were carers of children who had never had a gastrostomy. The gastrostomies had been placed by a number of different services. The children’s ages ranged from 4 to 19 years and all children were gross motor function classification system level V (severe physical impairment with no independent mobility).
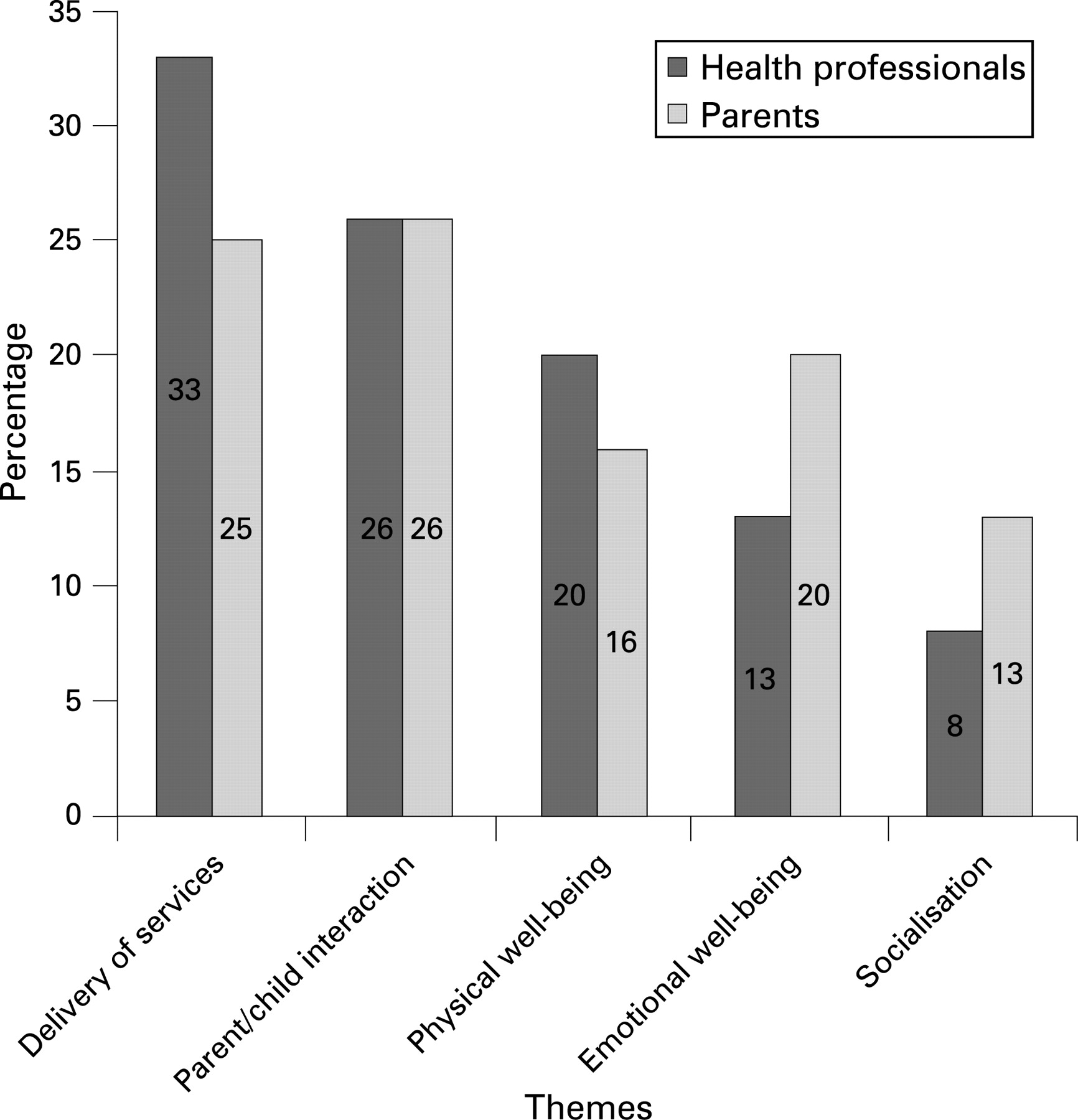
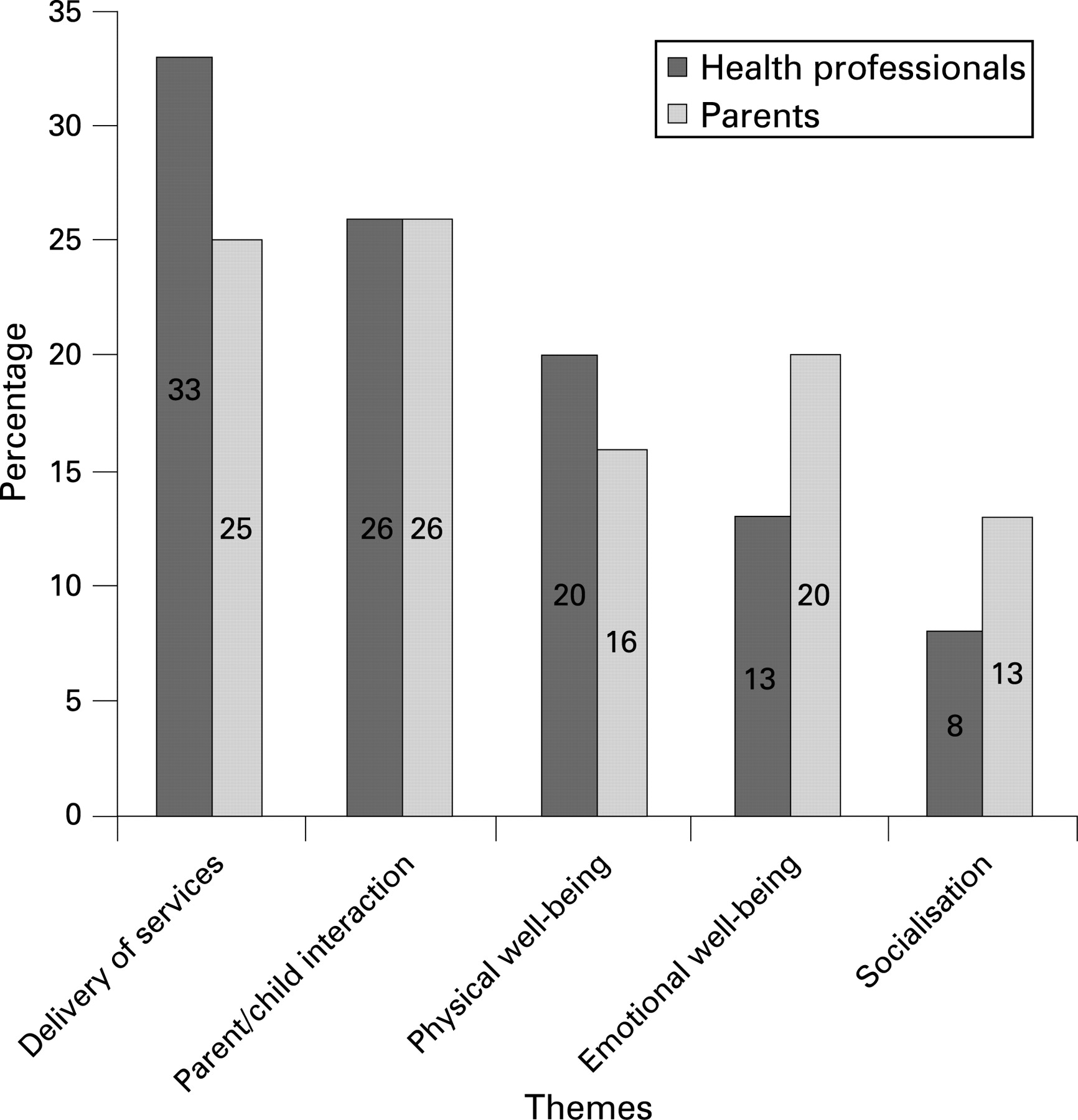
Five major themes were identified which comprised the following percentage of total amount of coded text: parent–child interaction (26%), delivery of services (25%), emotional well-being of the child (22%), physical well-being (16%) and socialisation (13%). These themes were further divided into subthemes (table 1).
Parent–child interaction (table 2)
Reciprocity of QoL
Parents recognised that parent and child QoL are inseparable. Parents described the physical work and extra tasks involved in caring for children with disabilities not as a burden but as an inevitable part of their lives. Stress surrounding their ability to safely and adequately feed their child and simultaneously manage other family needs weighed heavily on them (2.1). While they worried about their child’s future and the transition to adult services and long term care, many maintained hope for a “cure” or some improvement in their child’s condition. Dependence on one carer (usually the mother) was frequently an issue. Parents found the responsibility of choosing on behalf of their child difficult. They wanted to protect their child from possibly unnecessary or life threatening (eg, anaesthetics) interventions. Parents described how precious their time with their child was given their child’s shortened life expectancy.
Time impact
The time impact of feeding was a major issue for parents (2.2). Time spent preparing food and feeding the child and the preparation required for an outing meant less time was available for other activities and other family members including self. Nevertheless, for some parents the time spent feeding the child was regarded as an opportunity for quality time.
Family cohesion
Parents reported a negative impact on their marriage due to stress (2.3), and there was also tension in the extended family with differences of opinion or disapproval about management choices. The effect on siblings was very distressing for parents. Parents reported behaviour issues (eg, separation anxiety) among siblings.
Love
Parents talked at length about how much they loved their child and would do anything for them (2.4). They stressed the importance of love as an essential factor in QoL and that this was not often taken into account by staff (7b).
Delivery of services (table 3)
Interaction with professionals
Parents felt interaction with health and education professionals had a large impact on their QoL and that of their child. While some parents reported positive experiences, the majority reported negative experiences when communicating with staff. Often parents felt their opinions were not considered important (3.1a) and that they were not given all the necessary information about treatment options. Parents believed they were made to feel guilty or ashamed, particularly in regard to their child’s nutritional status. They thought staff took a very clinical approach without considering the families’ lived experience.
Parents felt a need for coordination of the multiple services to help them prioritise their child’s needs and that this was not adequately provided by their general paediatricians. Parents of children without gastrostomy expressed more satisfaction with the clinical care they had received than parents of children with a gastrostomy.
Parents often felt forced to challenge professionals for what they felt was in their child’s best interest. Parents noted that while their children had many problems in common, the individual needs of each child differed. When deciding about an intervention, they wanted to speak to other parents who had already been through the same process. Parents were very concerned that in hospitals, schools and respite care their child did not receive the same standard of care as an able bodied child (3.1b).
Gastrostomy
The majority of parents of children with gastrostomies reported a positive experience due to reduced time impact, decreased burden of care and improved physical comfort for the child. Many of the parents who had a positive view of gastrostomy considered it necessary for their child’s survival. Respiratory compromise was a strong incentive for proceeding with gastrostomy. The impact on ease of socialisation greatly affected parents’ views on gastrostomy. Gastrostomy reduced concern over safe, adequate nutrition, hydration and administration of medications and reduced dependence on one carer for feeding.
Parents with a negative experience of gastrostomy described unacceptable complications (eg, tube falling/being pulled out, infections), poor follow-up services and resources, and deterioration in the child’s health, happiness or socialisation. Some felt they had been pressured into accepting a gastrostomy or had not been informed of the potential negative aspects of gastrostomy (7a). Reasons for resisting a gastrostomy included reluctance to deprive the child of enjoyment of food, a perception that a gastrostomy is “unnatural”, concern about operative/anaesthetic complications, or hearing negative reports from other parents. Many felt that accepting a gastrostomy meant failing or giving up on efforts to orally feed (3.2).
Access to health services
Most of the parents felt that following gastrostomy they received inadequate ongoing support with management and insufficient supplies for replacement buttons (3.3). They believed that staff in hospitals, schools and respite services were often inexperienced in managing problems arising with gastrostomies and were frequently unwilling to be involved in the management of these issues. However, some parents reported that staff at schools and health services were extremely helpful.
Parents reported they were not always well informed about available funding to help meet the expenses associated with their child’s special needs. Some children (with and without gastrostomies) were refused access to services (schools and respite) as a result of feeding problems. Adequate respite was considered difficult to access.
Child’s emotional well-being (table 4)
Happiness
Parents felt their child was happy when they looked content, smiled, were less distressed, were more alert and were interactive with their environment. They believed the child’s personality and intelligence impacted on their happiness. Many parents thought staff underestimated their child’s intelligence. They were concerned that staff sometimes equated absence of pain with happiness for a child with a disability (7c). Parents identified friendships in their child’s life as an important part of QoL (4.1).
Enjoyment of food
Enjoyment of food was considered very important especially by parents of children without gastrostomy. Many felt that food was one of the child’s few enjoyments in life and wanted them to experience different tastes, textures and the social aspect of meals. Some of the parents of children with gastrostomies were very surprised that following gastrostomy their child was no longer interested in oral feeding and that what had been interpreted as enjoyment of food was actually hunger (4.2).
Independence
Parents discussed the child’s self-determination in being able to choose what and when they wanted to eat and who they wanted to feed them (4.3).
Physical well-being (table 5)
Physical comfort
Oesophagitis, reflux and respiratory issues (coughing, aspiration, pneumonia) were major contributors to level of physical comfort and pain (eg, orthopaedic); poor sleep, constipation, hunger, drooling and unpleasant interventions also contributed (5.1).
Nutritional status
Parents thought nutrition was important for their child’s general health and level of contentment. Some parents felt health professionals put too much emphasis on weight and that it was not the most important issue (7d). Some parents felt their children were thin naturally or due to their condition and that health professional’s expectations were too high (5.2a). The difficulty of having to manage a heavier child was a concern for a few parents (5.2b).
Other
Parents found managing intercurrent illnesses, trying to maintain nutrition and hydration and administer medications in a child with feeding problems was problematic. The child’s fatigue resulted in increased difficulty in feeding and less time and energy for other activities.
Socialisation (table 6)
Feasibility of social interaction
Parents viewed social interaction and the child’s opportunity to “experience life” as a major factor in QoL (6.1). Feeding problems limited social participation because of the required preparation and equipment, reduced accessibility and the need for special facilities to prepare appropriate food.
Social acceptance and normality
Parents reported that their child was often excluded from social events or attracted negative attention in public (6.2a). Parents stressed the need for the general public to be more accepting of people with disabilities. Many parents found they lost their friends when they had a child with a disability (6.2b). Parents were keen to approximate normality for their child where possible and wanted their child to have the same opportunities as a “normal” child.
Sharing a meal
Sharing a meal was considered an important part of social interaction. However, managing the child’s feeding problems often meant that neither parent nor child could partake in a social meal (6.3).
Comparison of parents’ and health professionals’ perceptions (table 7)
The five major themes identified were the same as those which emerged from the health professionals focus groups,30 however the content of subthemes and attitudes expressed differed greatly. Parents and health professionals also differed in the amount of discussion generated around each theme (percent of coded text, fig 1). Parents were more likely than health professionals to discuss subjective aspects such as emotional well-being and socialisation.
{kind=link}
Parent–child interaction (7.a)
Health professionals often talked of the “burden” the child’s condition placed on the parents, whereas parents viewed their child’s disability as a part of their lives and a source of joy despite the anxiety it generated. Unlike health professionals, parents did not talk about feeding being essential for bonding but acknowledged it was an important aspect of nurturing.
Health professionals speculated about parents’ dilemmas of prolonging and curtailing life when deciding about interventions, whereas parents talked about prolonging life and the fact that they would do anything to ensure their child’s well-being.
Delivery of services (7.b)
Both parents and health professionals talked extensively about communication difficulties with each other. Health professionals discussed how parents resist their recommendations, and while parents also raised this topic it was not a major issue for them. Parents and professionals agreed that this resistance was often in the context of gastrostomy and time to adjust to changes was a major factor in acceptance of recommendations. Overall, health professionals had very positive views of gastrostomy, while some parents reported that they had not been advised of potential negative aspects of gastrostomy.
A small minority of health professionals speculated that some parents actively sabotage medical interventions in order to avoid the child gaining weight. While many of the health professionals expressed compassion for the difficulties these families experience, the parent focus groups revealed a strong sense that they were not listened to by health professionals or had been made to feel guilty or ashamed over aspects of the care of their child. Parents raised a new subtheme stating the way professionals treated the child (3.1b) had an impact on their child’s well-being.
Childs’ emotional well-being (7.c)
Subthemes only arising in the parent focus groups included: love, personality, intelligence and friendship as important contributors to their child’s emotional well-being. Health professionals said they found a child’s happiness a difficult quality to assess.
Parents talked at length about how much they loved their child and considered love an important contributor to QoL, whereas health professionals did not mention the impact of love in the children’s lives.
Physical well-being (7.d)
Parents thought health professionals put too much emphasis on weight gain. Health professionals thought parents were very concerned about the difficulty of managing a heavier child, but this did not emerge as an important issue in the parent focus groups.
Socialisation (7.e)
Parents put greater emphasis on socialisation as a factor in QoL compared to health professionals. Parents often described their children as being part of the spectrum of normality while health professionals tended to describe the children as “not normal”.
DISCUSSION
This is the first study to use focus group methodology to explore parents’ perceptions of feeding-related QoL in children with quadriplegic CP and to compare parents’ perceptions with those of health professionals. Five major themes contributing to feeding-related QoL were identified: parent–child interaction, delivery of services, physical well-being, emotional well-being, and socialisation. These themes are consistent with the findings of previous studies.10 13–17 19 31 32
The key differences in the perceptions of parents and health professionals were that they differed in the relative importance they gave to each theme and the content of the themes (fig 1). Parents gave more importance to the themes of emotional well-being and socialisation, while health professionals focused more on the objective components of QoL. These differences in priorities may explain why communication between parents and professionals was frequently described by both groups as being difficult. Parents have a valuable contribution to make to the team of specialised professionals caring for their child as they possess “expert” knowledge of the child’s emotional and social well-being and the impacts which disability and treatments have on this aspect of QoL and are therefore well qualified to act as advocates for their child.
When parents are considering an intervention, the provision of information packs and opportunities to speak to families with both good and bad experiences of that intervention may facilitate informed decision making.
In this study, all sessions were audio- and video-taped and this enabled close monitoring and understanding of group dynamics and of verbal and non-verbal interactions. It also provided a measure of quality control by allowing recording of the verbal and non-verbal behaviour of the facilitator. The focus groups provided an environment similar to the social context in which parents make decisions, by providing an opportunity for them to discuss issues with their peers. The methods and research staff were common to both the parents’ and health professionals’ focus groups and so data are comparable.
Our finding that patients’ and health professionals’ views of QoL are often discordant has been found in many other studies. Health professionals often underestimate QoL in children with debilitating conditions, show less agreement on subjective aspects and underestimate pain.20–23 33–36
What are the clinical implications of this study? Both staff and parents agreed that the weighting of each theme varied between families and at different times, which highlights the need for professionals to be guided by the parents in assessing the child’s QoL. The information gathered in these focus groups provides a framework for clinical evaluation of QoL through addressing the five themes. Addressing QoL in clinical practice using the proposed framework may help to improve communication between health professionals and parents and ensure staff recognise the type and range of issues important to parents. The themes and subthemes which have emerged in these focus groups could be further developed to generate a formal measure of feeding-related QoL for use in clinical practice and research.
What is already known on this topic
Parents and health professionals have different perceptions regarding quality of life.
Feeding difficulties impact on the quality of life of children with quadriplegic cerebral palsy.
What this study adds
Parents are important in assessing aspects of their child’s quality of life such as socialisation and emotional well-being.
Health professionals are not aware of the full range of issues affecting feeding-related QoL as identified by parents.
Health professionals put more emphasis on the physical aspects of well being than parents.
Parents felt health professionals did not always listen to their viewpoints, often made them feel guilty or ashamed and only presented the positive aspects of gastrostomy feeding.
Acknowledgments
We would like to thank the parents and health professionals who participated in this study. We would also like to extend our gratitude to Dr Madeline King, CHERE, University of Technology, Sydney for her interest and advice, Cheryl Frazer for her efficient transcribing of the focus group tapes and Alison Lowe for assistance with the focus groups.
REFERENCES
Footnotes
Funding: AM was funded by a University of Sydney research scholarship and the Westmead Millennium Foundation Clancey Donald Scholarship. Additional funding was provided by the Centre for Kidney Research and the Department of Gastroenterology at the Children’s Hospital at Westmead.
Competing interests: None.