Article Text

Abstract
Background Preoperative imaging assessment of surgical risk is very important for the prognosis of these children. To develop and validate a radiomics-based machine learning model based on the analysis of radiomics features to predict surgical risk in children with abdominal neuroblastoma (NB).
Methods A retrospective study was conducted from April 2019 to March 2021 among 74 children with abdominal NB. A total of 1874 radiomic features in MR images were extracted from each patient. Support vector machines (SVMs) were used to establish the model. Eighty percent of the data were used as the training set to optimize the model, and 20% of the data were used to validate its accuracy, sensitivity, specificity and area under the curve (AUC) to verify its effectiveness.
Results Among the 74 children with abdominal NB, 55 (65%) had surgical risk and 19 (35%) had no surgical risk. A t test and Lasso identified that 28 radiomic features were associated with surgical risk. After developing an SVM-based model using these features, predictions were made about whether children with abdominal NB had surgical risk. The model achieved an AUC of 0.94 (a sensitivity of 0.83 and a specificity of 0.80) with 0.890 accuracy in the training set and an AUC of 0.81 (a sensitivity of 0.73 and a specificity of 0.82) with 0.838 accuracy in the test set.
Conclusions Radiomics and machine learning can be used to predict the surgical risk in children with abdominal NB. The model based on 28 radiomic features established by SVM showed good diagnostic efficiency.
- Pediatrics
- Medical Oncology
Data availability statement
Data sharing not applicable as no datasets generated and/or analyzed for this study. No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Neuroblastoma (NB) is one of the most common solid abdominal malignant tumors in children and seriously that threatens children’s lives and health.
Current therapeutic approaches for NB include surgery, chemotherapy, and radiotherapy combined with comprehensive treatment, which improve the prognosis for patients. However, surgery is still an important part of the treatment of NB, and its safety cannot be ignored.
To strive for total resection of the lesion or minimize tumor load during surgery and enable surgeons to choose a more appropriate surgical method before surgery and prevent intraoperative complications in advance, preoperative evaluation of surgical risk is of great significance to children with NB.
WHAT THIS STUDY ADDS
With the advent of the era of artificial intelligence and big data, radiomics, as an emerging technique, has been increasingly proved to have clinical significance.
Radiomics can capture automated quantitative analysis of phenotypic information through a data representation algorithm and extract meaningful imaging features from quantitative analysis of visual medical images, which can further play a role in guidance and prediction in clinical practice.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
If radiomic features are combined with other clinical data of children, advanced bioinformatics tools are used to conduct in-depth excavation and develop models, and comprehensive evaluation of tumor characteristics can be carried out to improve the accuracy of preoperative evaluation.
Radiomics can realize the noninvasive, quantitative, automatic assessment of the potential of spatial heterogeneity of tumors and predict the risk.
INTRODUCTION
Neuroblastoma (NB) is one of the most common solid abdominal malignant tumors in children. It can occur anywhere along the sympathetic nervous system, accounting for approximately 6%–10% of all tumors in children with a mortality rate of 15% and seriously threatening children’s life and health.1 Although current therapeutic approaches for NB include surgery, chemotherapy and radiotherapy combined with comprehensive treatment, which improve prognosis for patients, their effect remains poor, with a high risk of recurrence2 due to its diverse biological behavior. However, surgery is still an important part of the treatment of NB, and its safety cannot be ignored. NB has been staged with a gradual improvement from the International Neuroblastoma Staging System (INSS) to the international neuroblastoma risk group (INRG) in recent years.3 Abdominal NB in children is often large and easily invades surrounding tissues and blood vessels, resulting in high surgical difficulty and risk of postsurgical complications. Therefore, preoperative imaging assessment of surgical risk is very important for the prognosis of these children.
In recent years, image-defined risk factors (IDRFs) in the International Neuroblastoma risk Classification Group (INRG) have often been used as evaluation indicators4 to predict the risk of complications associated with tumor resection. The stratified risk assessment was carried out by preoperative imaging assessment including tumor location, whether the tumor invaded important blood vessels or organs and whether it entered the spinal canal and other indicators, which suggests that the incidence of surgical complications in IDRF-positive children was much higher than that in IDRF-negative children.5–7 Although IDRFs currently play the main role in the evaluation of surgical risk in NB, there are subjective interpretation errors. Only semiquantitative image information can be used to evaluate the structural characteristics of tumors, and there is no distinction between low-risk, medium-risk, and high-risk NB, which lacks the information needed for personalized biology and targeted therapy. It also fails to provide the molecular and gene-level biological information needed for precision medicine.
With the advent of the era of artificial intelligence and big data, radiomics, as an emerging technique, has been increasingly proved to have clinical significance. It can capture automated quantitative analysis of phenotypic information through a data representation algorithm and extract meaningful imaging features from quantitative analysis of visual medical images. Machine learning models for prediction can be established using these features,8 which can further play a role in guidance and prediction in clinical practice. At present, a number of studies on adults have reported that the pathological classification and grading of tumors9–13 and prognosis can be predicted before surgery by extracting radiomic features from medical images of abdominal malignant tumors and using machine learning for in-depth analysis. This study aimed to develop and validate a radiomics-based machine learning model based on the analysis of radiomics features to predict surgical risk in children with abdominal NB.
Materials and methods
Study population
A retrospective study was conducted from April 2019 to March 2021 among 74 children with abdominal NB at the Children’s Hospital, Zhejiang University School of Medicine. Inclusion criteria included (1) patients who underwent magnetic resonance imaging (MRI) plain scan of abdomen before treatment; (2) patients whose NB was removed; (3) patients who were confirmed by pathology; and (4) patients who did not receive any treatment before diagnosis. Exclusion criteria included (1) patients who had MRI contraindications; (2) patients who failed to be sedated; (3) patients with unknown pathology; and (4) patients whose MRI artifacts were obvious.
Data collection
Patient demographic and clinical data related to NB were extracted, including age, sex, neuron-specific enolase, INSS, MCYN amplification, absence of 11q-23 and SRD-1p36 and Ki67, and distant metastasis.
Criteria for surgical risk
According to the INSS and INRG,3 the included patients were divided into two groups: patients with surgical risk and patients without surgical risk. Criteria for surgical risk included: (1) NB surrounding peripheral large vessels (including celiac axis, superior mesenteric artery, iliac vessels and inferior vena cava); (2) NB crossing the midline; (3) NB extending into the adjacent spinal canal; (4) NB associated with lymph node metastasis (including retroperitoneal lymph nodes, mesenteric lymphoid nodes, inguinal lymph nodes, iliac vessels peripheral lymph nodes);5 (5) NB invading one or both renal pedicles; and (6) NB invading nearby organs (including liver, pancreas, duodenum, septum).
Fifty-five patients had surgical risk, and 19 had no surgical risk among the 74 included children with abdominal NB.
Examination method
All patients were scanned on a 3.0 T MRI scanner (Achieva 3.0 T Rex, Philips) with gradient field intensity 80 mT/m, slew rate 200 mT/(m s), using a dual-channel volume coil for transmission and an eight-channel coil with high sensitivity for reception. Children under 5 years of age should be given 10% chloral hydrate for sedation by coloclysis or oral administration approximately 40 min before examination and scanned after sleep. Children were provided hearing protectors for scans under free-breathing conditions. The following sequences were used: T1-weighted (T1W), T2-weighted (T2W), fluid-attenuated inversion recovery, mix, and B1. A complete MR examination lasted 15 min. Images were retrieved from The Picture Archiving and Communication System (PACS) for imaging feature extraction.
Image processing
The 3.0 T MRI plain scan data were downloaded from PACS to a personal laptop. Two radiologists with more than 15 years of clinical experience worked together to delineate ROIs on abdominal NB images in a double-blind manner using semiautomatic image segmentation method under three-dimensional Slicer (3D Slicer).14 Interobserver repeatability in feature delineation was preliminarily analyzed. Then, the two repeated delineations were performed according to the same procedure within 2 weeks to verify the intraobserver repeatability. The intraclass correlation coefficient (ICC) was used to determine intraobserver and interobserver differences.
Imaging feature extraction
Pyradiomics, an open-source Python package, was used to analyze and extract the radiomic features of ROIs in MR images of children with abdominal NB.15 After undergoing N4 bias field correction, isotropic voxel resampling and signal intensity normalization, the MR images used for radiomic feature extraction were transformed by Wavelet, Laplacian of Gaussian (LoG), Square, SquareRoot, Logarithm, and Exponential. All obtained images were extracted for radiomic features, and a total of 1874 features were obtained.
The extraction contents included first order statistics, Shape-based 3D, gray level co-occurrence matrix (GLCM), gray level run length matrix, gray level size zone matrix (GLSZM), neighboring gray tone difference matrix (NGTDM), and gray level dependence matrix (GLDM).
Statistical analysis
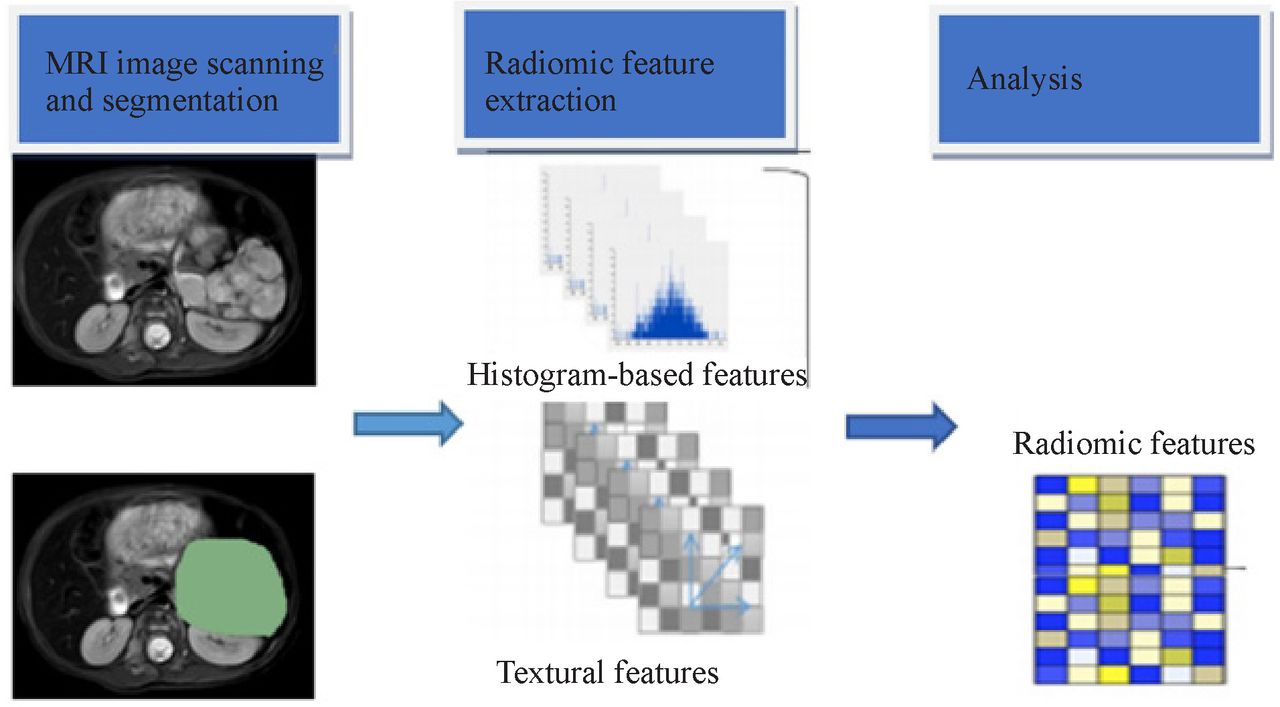
Demographic statistics were analyzed using R language (V.4.0.0, https://www.r-project.org/). A t test was used for age analysis, and the χ2 test was used for gender difference analysis between the two groups. Python was used to analyze the extracted radiomic data. Pandas, Numerical Python (Numpy), Scikit-learn (Sklearn), Scipy, seaborn, and matplotlib were used for data analysis and visualization. Feature selection was performed by independent sample t test and least absolute shrinkage and selection operator (Lasso).16 The selected radiomic features were used to establish an SVM-based model in the training set to predict the surgical risk in children with abdominal NB. After data imbalance correction via the synthetic minority oversampling technique, the prediction model was validated in the test set. The receiver operating characteristic (ROC) curve was plotted, and the area under the curve (AUC) was calculated to evaluate the performance of the model. P<0.05 was considered statistically significant. The flow chart of image processing, radiomic feature extraction and machine learning is shown in figure 1.
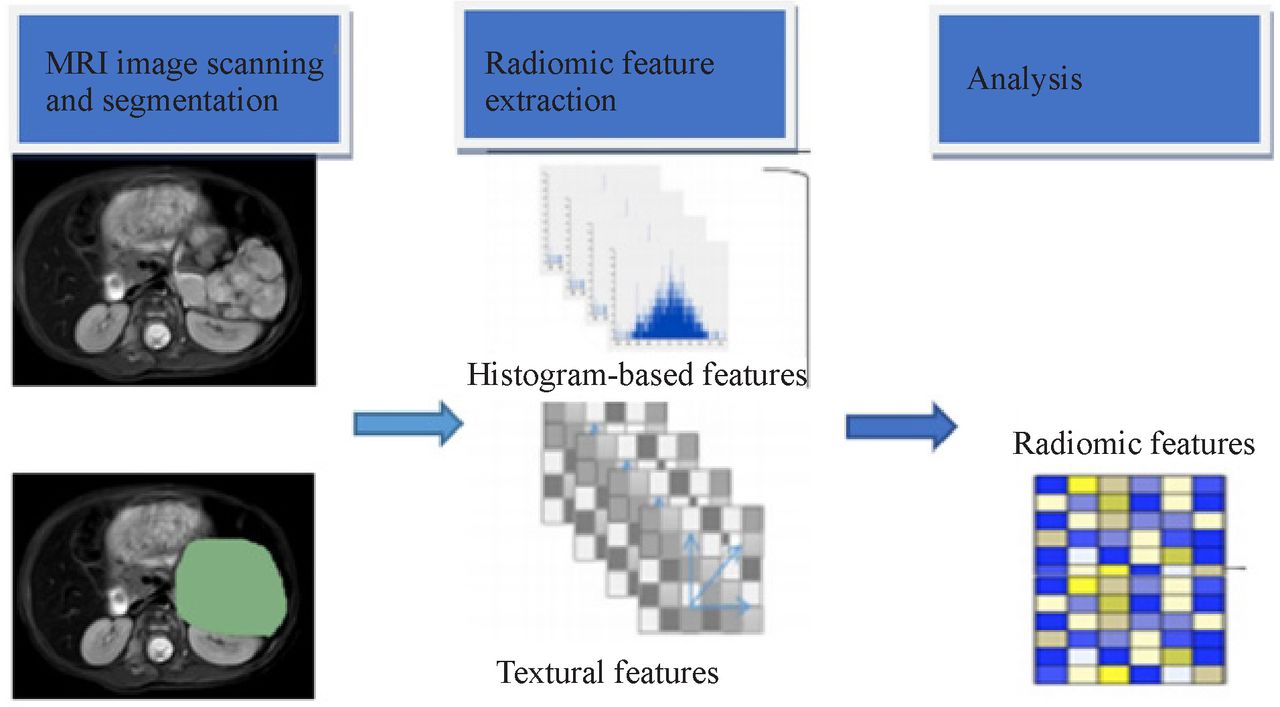
Flow chart of image processing, radiomic features extraction, and machine learning. MRI, magnetic resonance imaging.
Results
Clinical parameters
A total of 74 children with abdominal NB were included in this study, including in the training set with surgical risk and 19 in the test set without surgical risk. The mean age of patients was 4 years (0.1–13.9 years) and 4.2 years (0.2–12.1 years) in the training and test group, respectively. The results of the clinical parameters are shown in table 1.
Demographic and clinical data of included children with abdominal NB
Intraobserver and interobserver agreement
After the features of ROIs obtained by two radiologists underwent the ICC test, the features with poor agreement were deleted, and 1538 features with agreement above 0.75 were retained.
Radiomic feature extraction
A total of 1874 radiomic features were extracted from each patient’s MRI images and filter-transformed images using pyradiomics. A t test combined with Lasso identified that 28 radiomic features were associated with surgical risk, including 11 GLCM features, 3 NGTDM features, 4 GIRIM features, 4 GLSZM features, and 3 GLDM features (table 2, figures 2 and 3). These features were significantly different between the group with surgical risk and the group with no surgical risk (p<0.05), with a weight shown in figure 4. A correlation heatmap was also drawn with the feature to evaluate collinearity and redundancy among extracted radiomic features (figure 5).
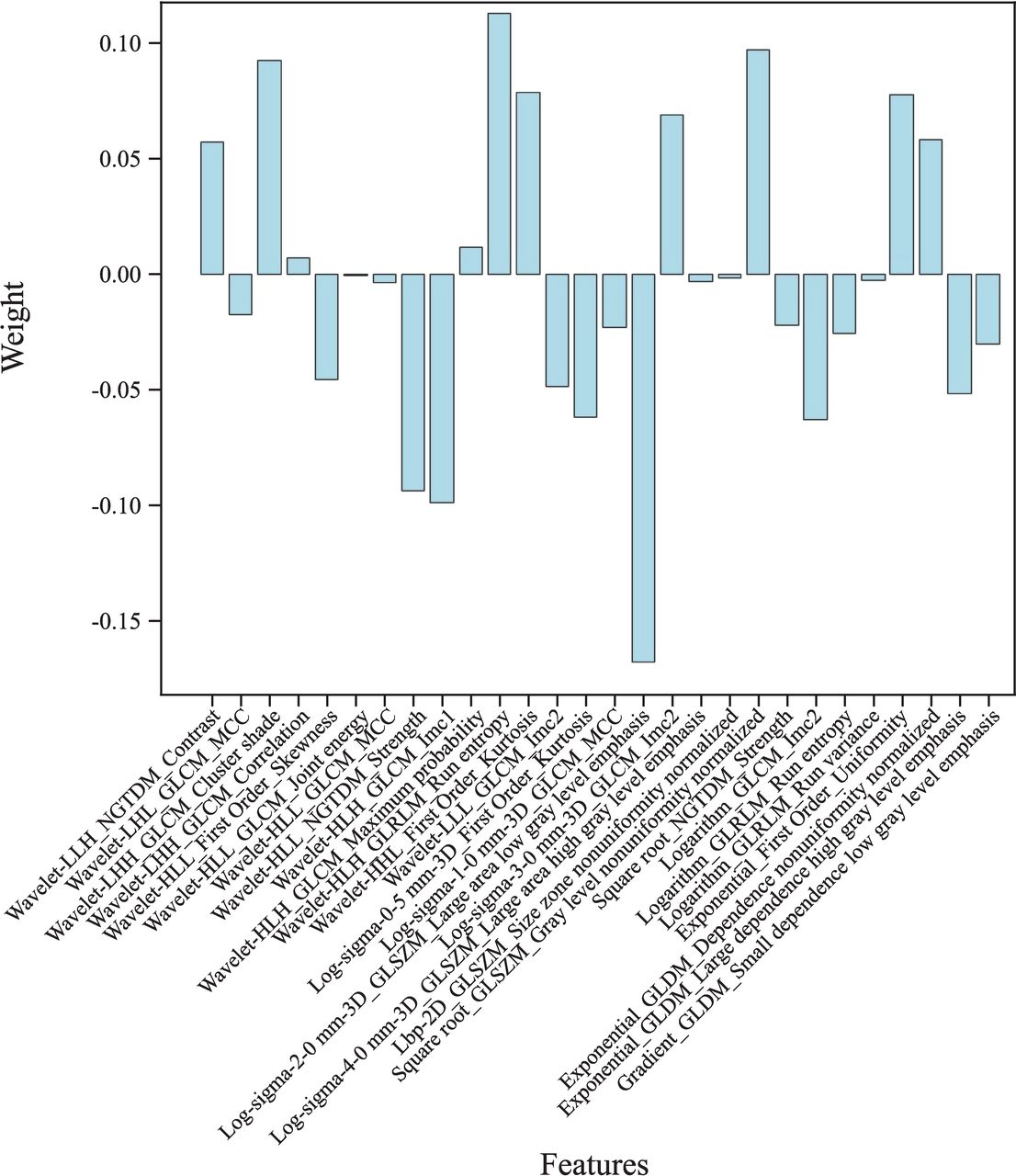
Weights of radiomic features obtained by selecting. (‘L’ means a low-passfilter. ‘H’ means a high-passfilter. ‘HLH’, respectively, means x, y. and z axis of the wavelet filter. ‘Wavelet-HLH’means that a high-passfilter, a low-passfilter and a high-passfilter was applied on x, y, and z axis of the wavelet filter, which was named analogously for ‘Wavelet-HHH’and ‘Wavelet-LLL’). GLCM, gray level co-occurrencematrix; GLDM, gray level dependence matrix; GLRLM, gray level run length matrix; GLSZM, gray level sizezone matrix; MCC, maximal correlation coefficient; NGTDM, neighboring gray tone difference matrix.
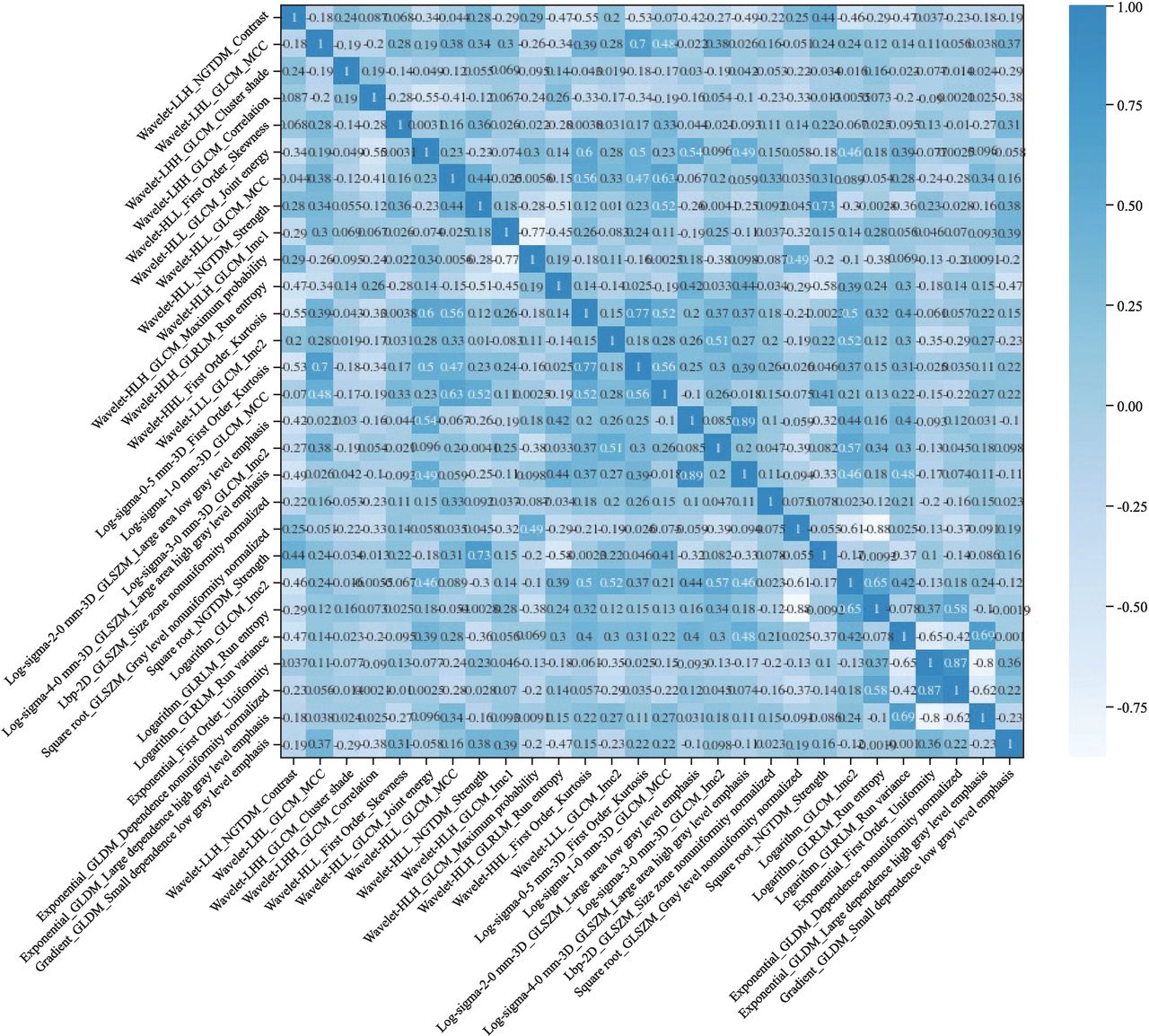
A correlation heatmap of radiomic feature (‘L’ means a low-passfilter. ‘H’ means a high-passfilter. ‘HLH’, respectively, means x, y. and z axis of the wavelet filter. ‘Wavelet-HLH’means that a high-passfilter, a low-passfilter and a high-passfilter was applied on x, y, and z axis of the wavelet filter, which was named analogously for ‘Wavelet-HHH’and ‘Wavelet-LLL’). GLCM, gray level co-occurrencematrix; GLDM, gray level dependence matrix; GLRLM, gray level run length matrix; GLSZM, gray level sizezone matrix; MCC, maximal correlation coefficient; NGTDM, neighboring gray tone difference matrix.
Selected radiomic features and their weights
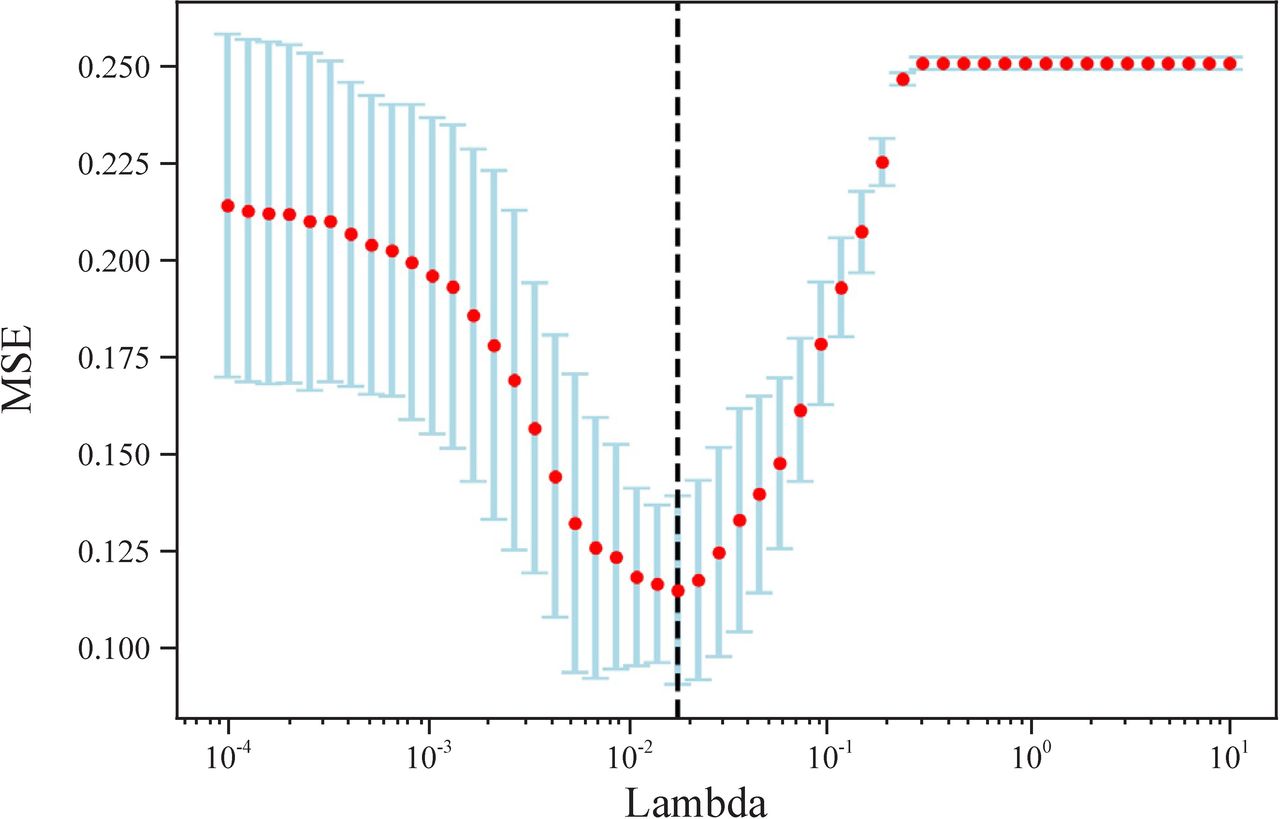
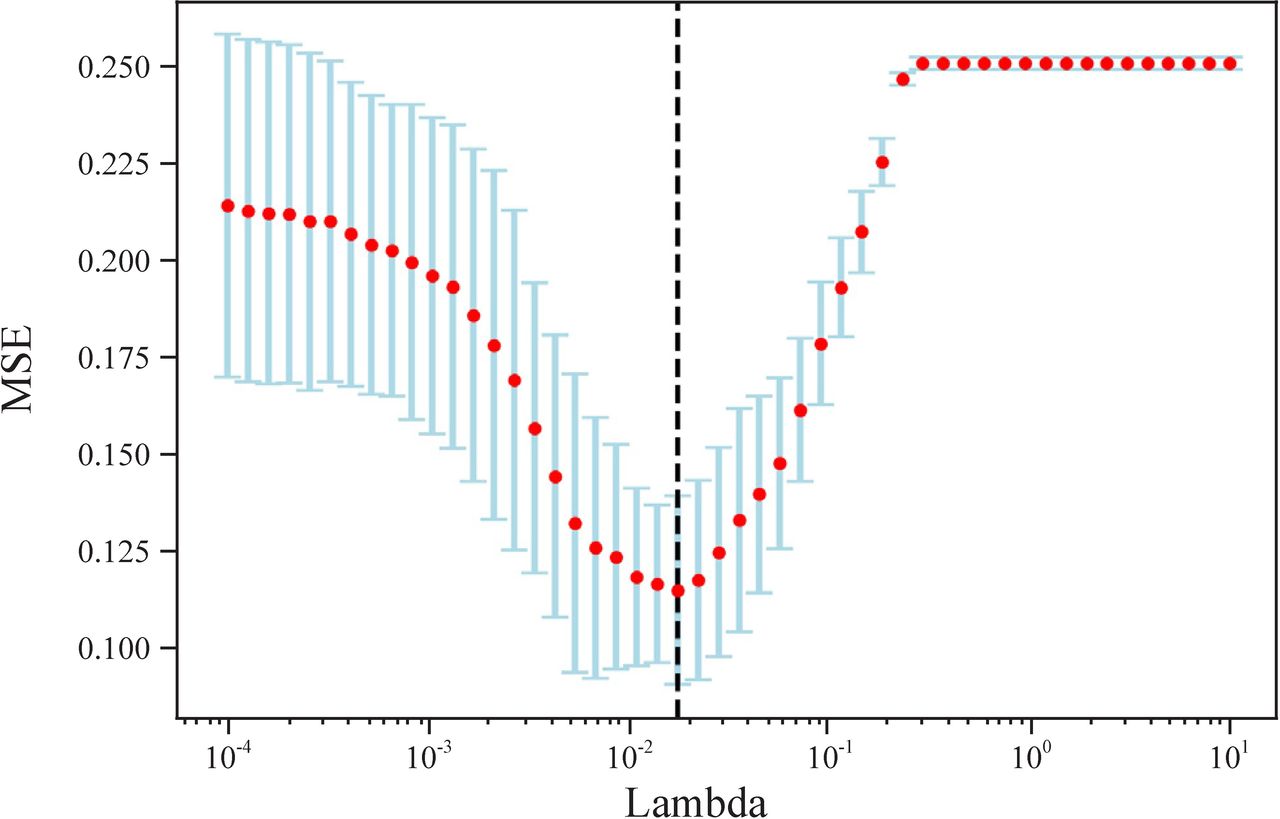
Lambda selection in Lasso. MSE, mean square error.
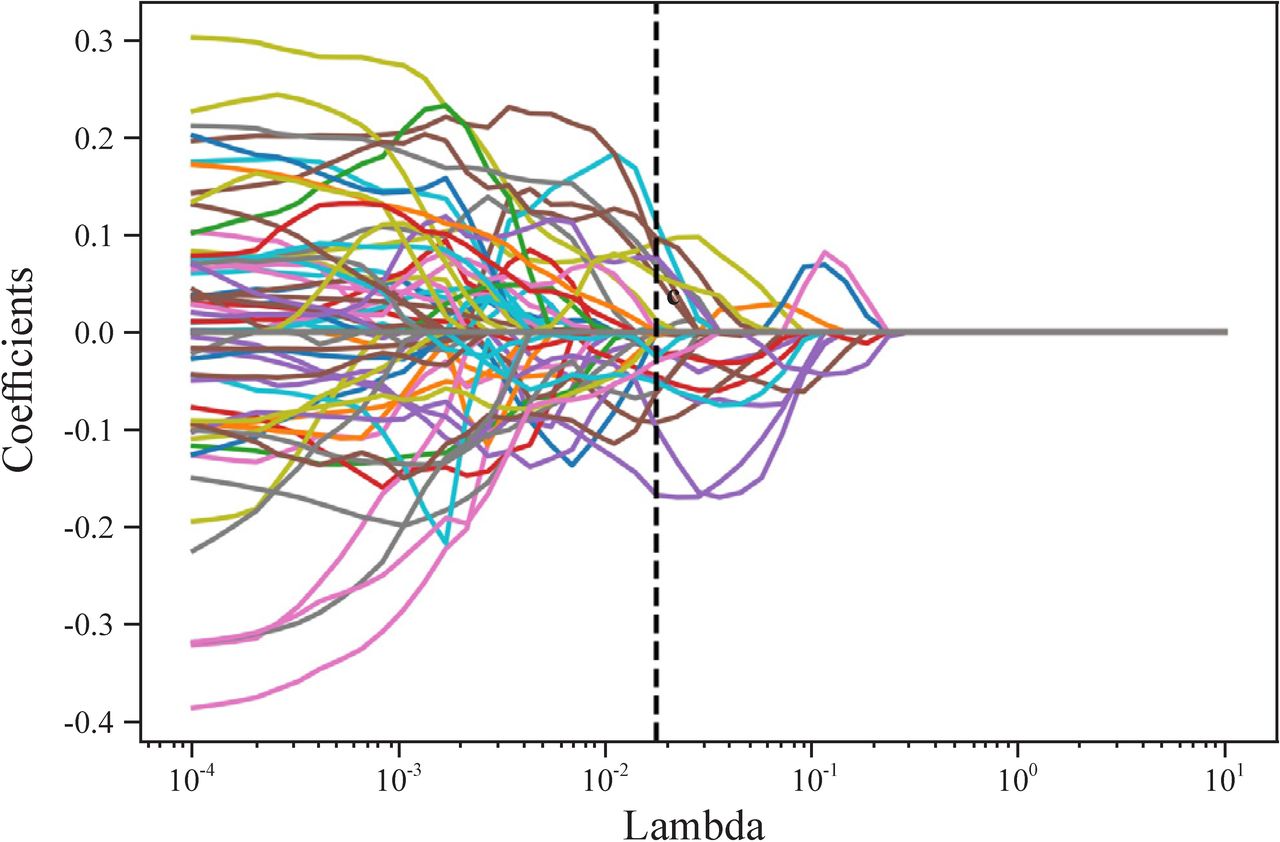
Curve of coefficient with Lambda changes when using Lasso selecting radiomic features.
ROC analysis
Eighty percent of the included children with abdominal NB were randomly selected as the training set, and the remaining 20% were selected as the test set. An SVM-based model to predict the surgical risk in children with abdominal NB was developed by applying the radiomic features selected in the training set and then verified in the remaining test set.
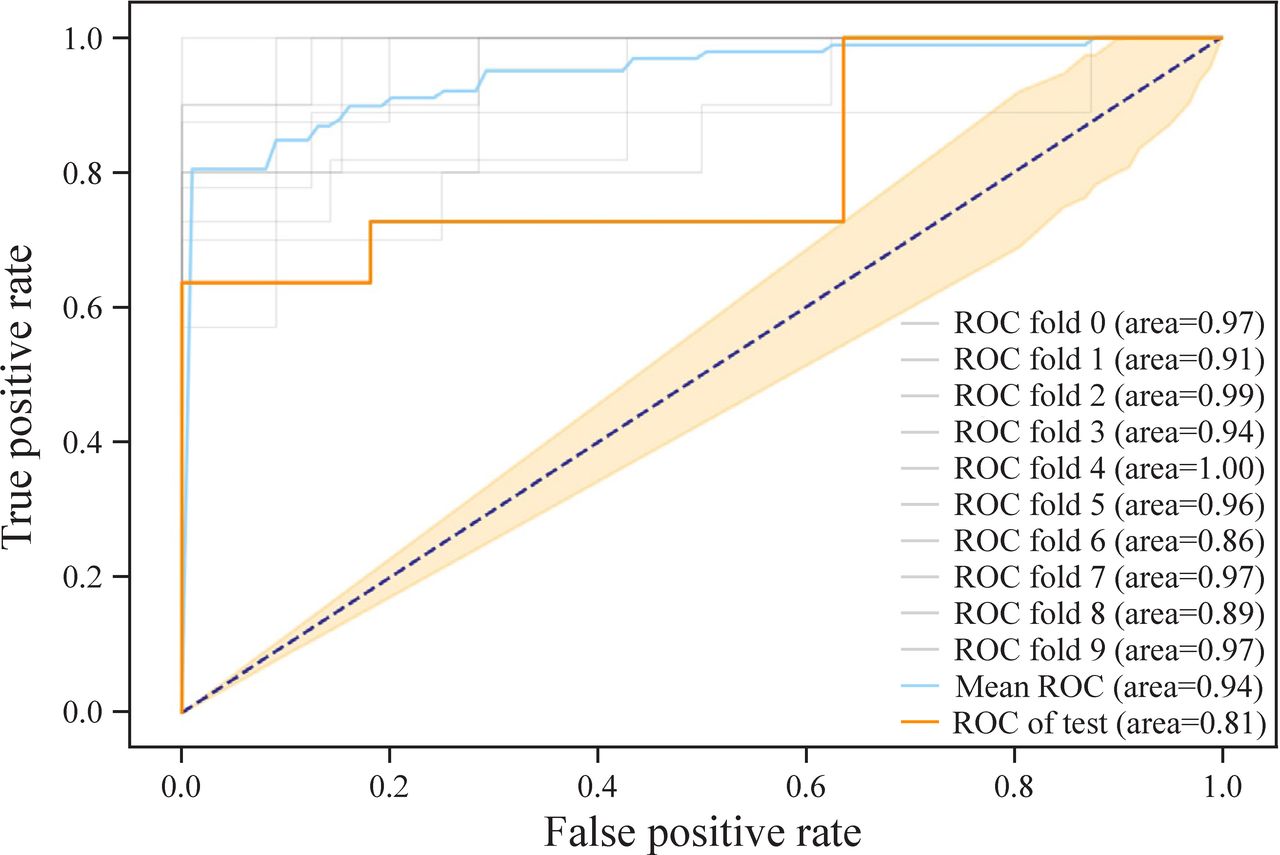
Repetitive parameter optimization of SVM was performed for the best classification effect and avoided overfitting, achieving an AUC of 0.94 (a sensitivity of 0.83 and a specificity of 0.80) with 0.890 accuracy in the training set and an AUC of 0.81 (a sensitivity of 0.73 and a specificity of 0.82) with 0.838 accuracy in the test set when penalty parameter C was 100 and Gamma was 0.01 (figures 6 and 7).
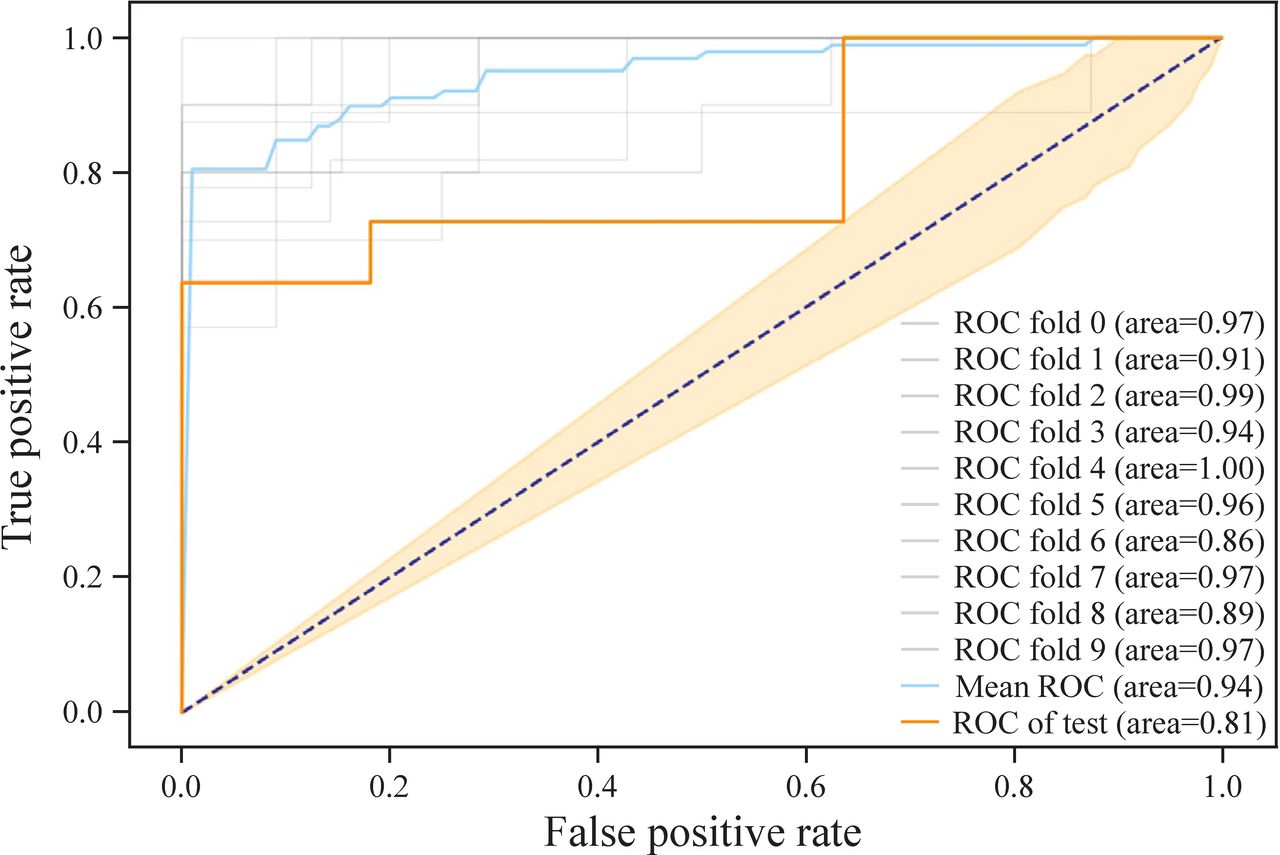
ROC curve of SVM-based model to predict the surgical risk in abdominal NB. NB, neuroblastoma; ROC, receiver operating characteristic; SVM, support vector machines.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
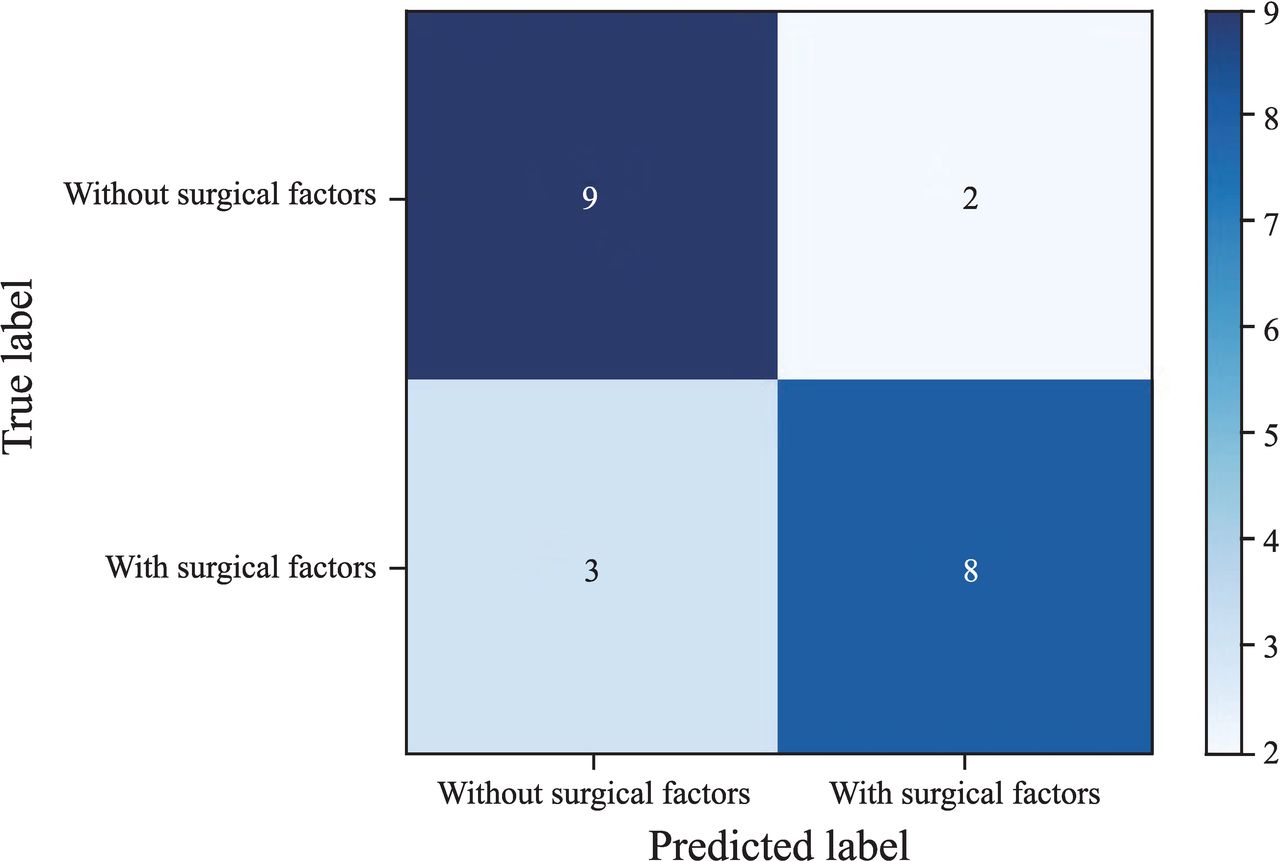
Matrix diagram of test set classification.
Discussion
NB is an embryonal malignant tumor of the sympathetic nervous system in children, and its prognosis varies greatly among children. According to the current international treatment guidelines, there is no surgical risk for NB with clear boundaries with surrounding tissues, so tumor resection can be performed directly without induction chemotherapy. However, it is considered that there is surgical risk for NB with close association with surrounding tissues; therefore, surgery can be considered only after biopsy, induction chemotherapy, and reevaluation. To strive for total resection of the lesion or minimize tumor load during surgery and enable surgeons to choose a more appropriate surgical method before surgery and prevent intraoperative complications in advance, preoperative evaluation of surgical risk is of great significance to children with NB.17–20
Although the rapid development of radiomic equipment and technology in recent years has allowed tumor growth and invasion to be determined according to the characteristics of morphology, density, edge, and other features, it is still difficult for radiomic doctors to quantitatively judge the local invasion of the tumor by naked eye and find a few blood vessels and lymph nodes. Although these images reveal far more valuable information than human beings can recognize, it is still difficult to effectively use them during image interpretation in practical work. Radiomics, as an in-depth medical image analysis tool, is capable of high-throughput, automated analysis, and extraction of large quantitative image features and thus has the potential to assess the spatial heterogeneity of tumors and can be used as a noninvasive tool for ‘multiple virtual biopsies’.21 22 If radiomic features are combined with other clinical data of children, advanced bioinformatics tools are used to conduct in-depth excavation and develop models, and comprehensive evaluation of tumor characteristics can be carried out to improve the accuracy of preoperative evaluation and prediction of prognosis.23 Gao et al13 used pyradiomics to conduct radiomic analysis on CT images of 165 gastric cancer patients in three independent cohorts, obtaining six robust radiomic features and established models to verify and test the good estimation of tumor infiltrating regulatory T cells (TITreg) in the cohorts. Multivariate Cox regression analysis showed that the radiomic feature was an independent risk factor for poor overall survival in patients with gastric cancer. Kaissis et al24 applied pyradiomics to analyze preoperative CT images of 207 patients with pancreatic duct adenocarcinoma and developed a random forest machine learning algorithm to predict molecular subtypes of pancreatic cancer based on radiomic features. The sensitivity, specificity, and AUC were 0.84±0.05, 0.92±0.01, and 0.93±0.01, respectively, suggesting that radiomics analysis could predict the molecular subtypes highly correlated with the survival of patients with pancreatic cancer.
In our study, pyradiomics was used to achieve radiomic feature extraction, and a t test and Lasso were used to identify 28 radiomic features associated with surgical risk from a large number of radiomic features. These radiomic features showed statistical features between NB cohorts with and without surgical risk. The SVM-based prediction model achieved an AUC of 0.94 (a sensitivity of 0.83 and a specificity of 0.80) with 0.890 accuracy in the training set and an AUC of 0.81 (a sensitivity of 0.73 and a specificity of 0.82) with 0.838 accuracy in the test set, showing a good effect. This result indicated that radiomics and machine learning were feasible for predicting the surgical risk in children with abdominal NB. The GLCM and GLSZM in the model based on 28 radiomic features established by SVM had greater weights. Considering the relatively small number of children included in the analysis, we believe that the classification of 28 radiomic features in these six categories for surgical risk in NB should be interpreted carefully. At present, it is only a preliminary exploration.
There were some limitations in our study:1 Due to the limitation of the number of patients, the sample size for machine learning is still relatively small. After expanding the sample size in the future, more parameters can be included for modeling to observe whether the prediction ability of the model can be further improved.2 This study lacked an independent validation set. To ensure that our method can be extended to independent data, further research and validation in independent data sets are needed. We plan to seek multicenter cooperation to remedy this defect.3 Parmar et al,25 through in-depth studies, believed that the selection of classification methods was the most important factor for performance differences (accounting for 34.21% of the total differences), and the determination and application of the best machine learning method was an important step to explore stable and clinically relevant radiomic biomarkers. In this study, we only verified SVM machine learning to develop a radiomic model. Whether other classifiers have better effects was not involved. We will further explore and verify the effectiveness of other classifiers in future studies.
In summary, this study attempted to predict surgical risk in children with abdominal NB via radiomics and machine learning. SVM was used to establish a machine learning model based on 28 radiomic features. The results showed that the model had a high accuracy in distinguishing preoperative surgical risk for abdominal NB, which could provide a reference for the quantitative selection of clinical treatment strategies.
Data availability statement
Data sharing not applicable as no datasets generated and/or analyzed for this study. No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Ethics Committee of the Children’s Hospital Affiliated to Zhejiang University School of Medicine, and all guardians of the subjects understood the contents of the examination before conduction and signed the informed consent form (2021-IRB-117). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors XJ contributed to manuscript preparation and data collection. JL and XM contributed to manuscript preparation. WW and CL contributed to manuscript editing and review. XJ is responsible for the overall content as guarantor. She accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.