Article Text

Abstract
Objective One option for the treatment of perforated appendicitis in pediatric patients is interval appendectomy (IA). A patient decision aid (PDA) can be useful in the decision-making process regarding IA. The purpose of this study was to evaluate parents’ decisional conflict before and after engaging with a developed PDA.
Methods Participants included (a) parents who are considering IA surgery for their child, (b) have not yet had their follow-up appointment postdischarge, and (c) were fluent in either the official languages of English or French. This study used a pretest and post-test design to measure participants’ decisional conflict and treatment option choice. Perceptions and acceptability of the PDA were also assessed.
Results A total of 18 participants completed the study (16 mothers). Major findings include significant decreases in all Decisional Conflict Scale items from pre-PDA to post-PDA engagement, except for one item. The majority of participants perceived the PDA to be useful, easy to find information regarding risks and provided enough information to help them make a decision regarding their child’s treatment.
Conclusions This is the first study to develop and evaluate a PDA among parents who are making a decision regarding IA surgery. The results showed a significant decrease in decisional conflict after using the PDA. The results also showed that the PDA was generally accepted among parents and had positive perceptions regarding length, content, and balance. The use of PDA for this population can help ease feelings of decisional conflict and equip parents with the information to make informed decisions.
- Pediatrics
- Gastroenterology
- Patient Participation
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Research on the risks of treatment options for perforated appendicitis is inconclusive, and parents often experience decisional conflict when deciding whether their child should undergo elective interval appendectomy (IA) surgery. A patient decision aid (PDA) can assist parents in the decision-making process.
WHAT THIS STUDY ADDS
This study evaluates the first ever PDA for pediatric patients with perforated appendicitis. The results of this study suggest that PDA is favorable among parents and can reduce feelings of decisional conflict and equip them with knowledge to make informed decisions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Healthcare practitioners might consider using a PDA when discussing a child’s IA with parents. This can facilitate the shared decision-making process and make parents feel more informed about the benefits and risks of management of their child’s appendicitis.
Introduction
Appendicitis is one of the most common surgical diagnoses among pediatric patients, with over 30% of patients diagnosed with appendicitis presenting with perforation with a higher prevalence among younger patients.1–5 Perforated appendicitis (ie, a visible hole present in the appendix) is a relatively common condition and can be treated with antibiotics.1 6–9 If improvement is observed, the healthcare team decides whether to conduct an interval appendectomy (IA) or use a more conservative approach (ie, expectant management). At our center (ie, the Children’s Hospital of Eastern Ontario (CHEO)), treatment practice varies, but when a patient experiences greater than 5 days of symptoms or there is imaging depicting an abscess, then conservative management and necessary drainage is undergone. In the broader literature, there is a lack of consensus on whether conservative management or IA is superior to the other. To provide clarity, a recent systematic review regarding the risk of developing negative outcomes from IA versus expectant management treatment options was conducted. The results of the review suggest that the risks of developing negative outcomes from either treatment option were similar.9 Given the lack of consensus regarding optimal treatment, this information should be made available to parents of children with perforated appendicitis, as decision-making regarding surgical treatment is often left to parents.
When parents are held responsible for deciding whether their child should undergo elective IA, they may experience decisional conflict (ie, when an individual experiences uncertainty regarding actions that involve high stakes).10 Experiences of decisional conflict can peak when decision-makers feel uninformed and experience a lack of clarity and confidence regarding their decision-making abilities, possibly resulting in indecisiveness, delayed decision-making, and decisional regret.11–13 Shared decision-making (SDM), a collaborative decision-making model of healthcare involving children, their parents and healthcare providers, can help facilitate decision-making among parents.14 One strategy within the SDM model of healthcare is the use of patient decision aids (PDAs).
PDAs are evidence-based tools that can be used to assist in SDM among parents facing difficult decisions regarding surgical treatments such as IA. While the use of PDAs has been shown to improve feelings towards treatment decisions,15 there has been little literature surrounding the use of PDAs among parents making decisions regarding the treatment of perforated appendicitis. To address this gap, the research team conducted a needs assessment among parents considering elective IA.16 Additionally, feasibility was assessed among Canadian pediatric surgeons. They indicated that delivering the PDA to families at initial discharge and answering questions at the follow-up appointment would be feasible and would not cause barriers to care provision. Findings from this needs assessment revealed the presence of decisional conflict among parents considering elective IA for their children, suggesting the need for a PDA to support them in their decision-making process.16
To address the decisional conflict experienced by parents and their desire for more information to inform their decision-making, Nasr and colleagues created the first ever prototype PDA for parents considering IA surgery for their children by conducting a needs assessment among parents at CHEO. A full description of the needs assessment that informed the development of the PDA can be found in Grandpierre et al.16 Based on the feedback from the needs assessment, a prototype of the PDA was created in collaboration with healthcare practitioners, researchers and parents. The Ottawa Decision Support Framework was used to guide the development of the PDA, and the standardized PDA template provided by the Ottawa Patient Decision Aid team was used and adapted for the PDA.17 18 The current study took place at CHEO and is part of a multiphase study aimed at assessing PDA among parents in ‘real-life’ situations. The purpose of the current study was to evaluate parents’ decisional conflict before and after engagement with the PDA. A secondary purpose was to conduct post-PDA engagement questionnaires regarding parents’ acceptance of the PDA.
Methods and materials
Context of the PDA
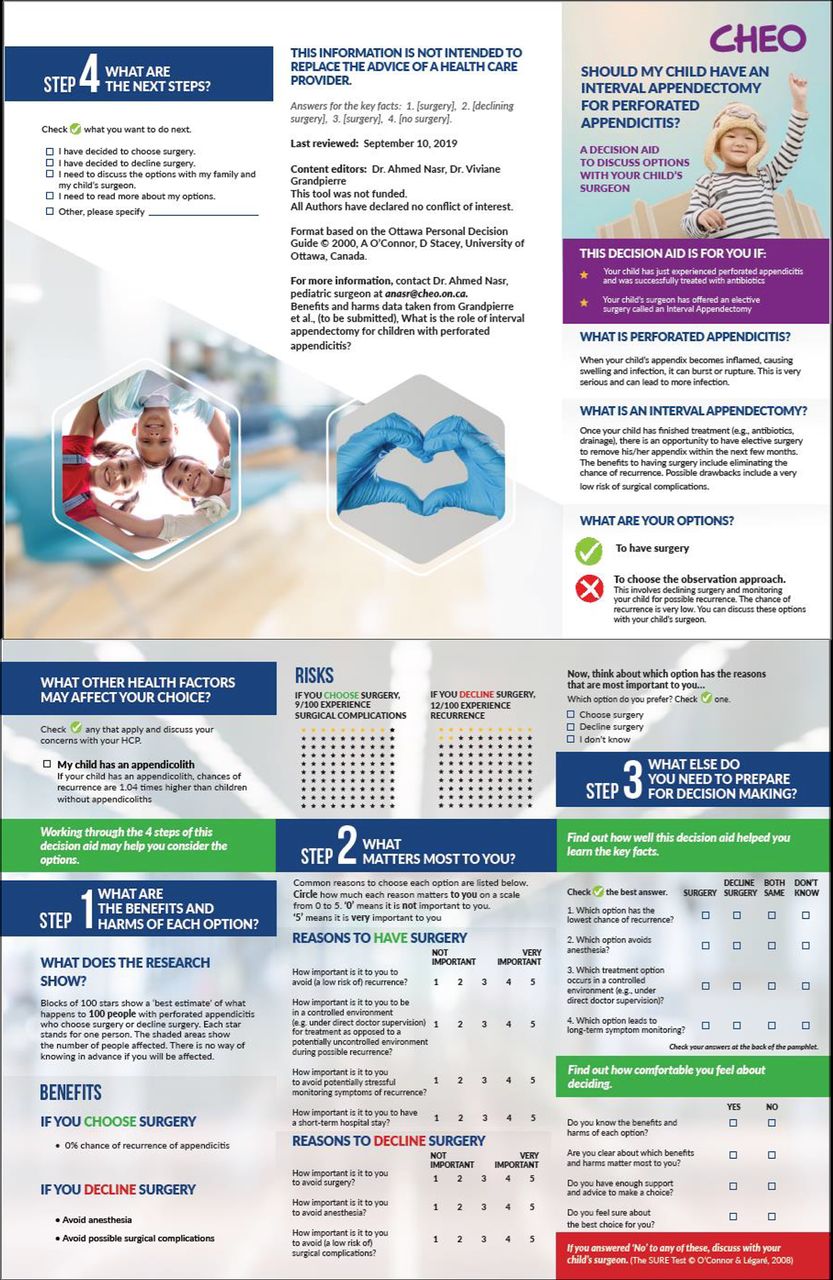
The PDA (see figure 1) developed as part of the Canadian Association of Paediatric Surgeons (CAPS) Decision Aids Project and adheres to the International Patient Decision Aid Standards.19 The research team already collaborates with the CAPS to produce the CAPS Evidence-Based Resource, which provides summaries of the best available evidence on a variety of pediatric surgical topics and is an essential step in the development of a PDA.20 The PDA used in this study was informed by a systematic review of the literature regarding IA surgery among pediatric patients9 and a needs assessment among families of patients with perforated appendicitis.16 The PDA contains four steps: (a) summaries of both treatment options, (b) benefits versus risks, (c) exercises to determine what matters most to them in the decision-making process, and (d) the identification of any additional needs that may influence decision-making. The PDA developed by Nasr and colleagues was used as the PDA for parents of pediatric patients who are considering IA surgery for their child.

{kind=link}
Pilot interval appendectomy patient decision aid. CHEO, Children’s Hospital of Eastern Ontario; HCP, healthcare provider.
Participants
Participants were eligible if they were (a) parents of children with perforated appendicitis who are undergoing the decision-making process of whether their child will have IA surgery, (b) have not yet had their follow-up appointment postdischarge, and (c) were fluent in either the official languages of English or French. At CHEO, perforated appendicitis is defined as a visible hole or tear in the appendix, with signs of abscess, phlegmon, or collections. Recruitment occurred between February 2020 and November 2021. Eligible participants were approached during initial admission by the research coordinator or the primary investigator. Once informed consent was obtained, participants were provided with the PDA after their child recovered as an outpatient. Patients were being treated by antibiotics or drainage, and PDA was provided to participants after the patient was discharged to help them decide whether they wanted to proceed with the IA surgery. Then, researchers arranged and conducted the interviews. Interviews were conducted between February 2020 and November 2021. The research team has extensive experience in clinical research, including interviewing parents of sick children.
Measures
Pretest baseline measures
Participants were asked to complete a brief demographic questionnaire assessing age, level of education and career. The primary investigator also reviewed the child’s medical history specific to his/her appendicitis (eg, child’s age at date of admission, diagnosis, treatment, discharge—see case report form). Next, a validated Decisional Conflict Scale was administered, which was used to distinguish between families who are hesitant about treatment decision-making and those who are decisive.21 Participants were asked to rate their agreement (0=strongly agree to 4=strongly disagree) on a series of statements (eg, I know which options are available to me, I am choosing without pressure from others, and This decision is easy for me to make). Last, participants were asked to indicate which treatment option they were considering for their child.
Post-test measures
After completing the PDA, participants once again completed the Decisional Conflict Scale. Finally, they completed a standardized acceptability questionnaire that evaluated items such as clarity, length, and helpfulness of the information within the PDA.21 Participants were also asked to rate their acceptability of the PDA (0=poor, 1=fair, 2=good, 3=excellent) on a series of eight statements (eg, treatment options, benefits of surgery and benefits of no surgery). Finally, participants were asked to indicate which treatment option they were considering for their child.
Data analysis
Descriptive statistics were used to describe the sample. Pre-PDA and post-PDA differences in the Decisional Conflict Scale were analyzed using paired sample t-tests. Frequencies were calculated for treatment option choice pre-PDA and post-PDA and participants’ acceptability of the PDA. Mean scores were also calculated for the acceptability questionnaire. Statistical analyses were performed using SPSS V.28.
Results
Participants’ characteristics
A total of 18 participants were recruited and included in this study (16 mothers and fathers). The mean age of the participants was 41.94 years (SD=6.881). Education level included high school (n=3), college diploma (n=9), undergraduate university degree (n=5), and graduate degree (n=1).
Pre-PDA and post-PDA Ddecisional Conflict Scale
Paired sample t-tests were calculated to understand the difference in means from the Decisional Conflict Scale before and after completing the PDA. Significant decreases in all items within the Decisional Conflict Scale were observed at a p level of 0.05 except for the item ‘I am choosing without pressure from others’ (p=0.110). The results of the paired sample t-tests are described in table 1.
Comparison of scores from Decisional Conflict Scale before and after PDA
Treatment option choice
Descriptive statistics were calculated to determine participants’ treatment option choice pre-PDA and post-PDA. The results can be found in table 2. Those who were unsure of a treatment choice pre-PDA had made a decision post-PDA.
Treatment option choice pre-PDA and post-PDA
Acceptability of PDA
Means were calculated for participants’ perceived acceptability of the PDA. Acceptability scores can be found in table 3. All acceptability scores were rated as ‘good’ by participants.
Acceptability of the PDA
Participants also found the length of the PDA ‘just right’ (n=17) and the amount of information ‘just right’ (n=17). The majority of participants found the PDA to be ‘balanced’ (n=16), where one participant found it to be ‘slanted toward having surgery’, and another participant found it to be ‘slanted toward not having surgery’. The majority of participants (n=17) found the PDA useful when making a decision regarding surgery. All participants (n=18) agreed that the PDA made it easy to find their child’s risk of recurrent appendicitis. The majority of participants (n=15) thought that the rest of the PDA made their decision easier. The majority of participants (n=12) thought there was enough information included in the PDA to help them make a decision regarding their child’s surgery.
Discussion
To our knowledge, this study is the first to develop and evaluate a PDA among parents who are making a decision regarding treatment for their child’s perforated appendicitis. A systematic review of the literature regarding perforated appendicitis treatments found that the risk of postoperative complications is similar to the risk of recurrence of appendicitis (9). While the risks of both options are relatively low, there is uncertainty surrounding an optimal treatment option. Given this uncertainty, there was a need for the development of a PDA to help parents make a decision regarding their child’s appendicitis treatment. Considering that decision-making regarding pediatric surgery is often left to parents,16 the present study developed a PDA to address the decisional conflict parents were experiencing regarding their child’s appendicitis treatment. The purpose of this study was to evaluate parents’ decisional conflict before and after engagement with PDA as well as to evaluate parents’ acceptability of PDA.
When comparing decisional conflict from pre-engagement to postengagement with the PDA, we revealed that all variables related to decisional conflict significantly decreased (except for ‘I am choosing without pressure from others’), demonstrating that the PDA had a positive effect on parents’ decisional conflict regarding treatment for their child’s appendicitis, as their decisional conflict decreased after engaging with the PDA. One reason why the item ‘I am choosing without pressure from others’ did not exhibit decreases from pre-engagement to postengagement with the PDA could be because this item is an environmental or contextual factor that may not be easily influenced by the PDA. For example, parents may experience pressure from outside sources such as family members, friends or social media to either choose or decline IA surgery for their child. It is also possible that parents felt pressure from the medical support team to make their respective decisions.
The findings from the current study corroborate previous research regarding the use of PDAs among parent populations in healthcare settings.15 22 For example, parents in this study felt as though they had enough information to make a decision. It has been shown that PDAs used in conjunction with healthcare practitioner interactions can help increase knowledge of available treatment options.15 22 Furthermore, small changes were observed in treatment choice from pre-engagement to postengagement with the PDA, as two parents who were unsure of a treatment choice before engaging with the PDA had reached a decision after. These findings demonstrate that PDA for parents regarding perforated appendicitis treatment can have a positive effect on those who are indecisive. A database of systematic reviews indicates that the use of PDAs reduces the proportion of undecided participants while also having a positive effect on patient–clinician SDM.15 It is possible that the PDA provided the parents in this study with more information or an opportunity to rationalize the treatment options, which has been demonstrated in previous research.15
General acceptability of the PDA was rated between fair and good for all items, indicating that the parents in this study accepted the PDA and that it could be helpful in their decision-making process. Furthermore, parents in this study found the length and amount of information in the PDA to be just right, balanced and useful. All parents agreed that the PDA made it easy for them to find their child’s risk of recurrent appendicitis. Information that is presented clearly can help parents make informed and evidence-based decisions.15 The majority of parents also agreed that the PDA made their decision regarding treatment easier and that the amount of information was sufficient to help them make a decision.
While this study’s strength is that it is the first to examine a PDA among parents considering treatment options for their child’s appendicitis, this study does not go without limitations. Namely, the small sample size made it difficult to run more sophisticated statistics. Future research is encouraged to recruit a larger sample to examine changes in knowledge from before and after engaging with PDA to determine the effectiveness of PDA. Future research is also encouraged to conduct qualitative focus groups with parents and clinicians to gather feedback on the PDA and use this feedback to develop future iterations. In this study, data were collected via telephone to adhere to the in-person restrictions due to the COVID-19 pandemic, which can affect engagement with the PDA. Ideally, future qualitative focus groups should be conducted in person.
In conclusion, this is the first study to examine PDA among parents making a decision regarding treatment for their child’s perforated appendicitis. The results from the pre-post test design indicate significant decreases in decisional conflict and changes in treatment option choices to which those who were unsure before engaging with the PDA had made a decision after the PDA. The PDA was generally accepted among parents and had positive perceptions of the length, content, and balance. These results indicate that a PDA for this population can help ease feelings of decisional conflict and equip parents with information to make informed decisions. Future research is encouraged to recruit a larger sample to conduct more complex statistical analyses to determine PDA effectiveness. The findings from this study can inform the development of future iterations of PDAs for this population of parents.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the CHEO Research Institute Research Ethics Board (CHEOREB number: 16/172X). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors VL was responsible for data analysis and writing of the manuscript. IO and VG were responsible for measures development and data collection. AN supervised the study and was responsible for conception of the study as well as assisting with editing and data analysis. AN is the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.