Article Text

Abstract
Background No systematic review and meta-analysis to date has examined multiple child and parent-reported social and physical quality of life (QoL) in pediatric populations affected by Hirschsprung’s disease (HD) and anorectal malformations (ARM). The objective of this systematic review is to quantitatively summarize the parent-reported and child-reported psychosocial and physical functioning scores of such children.
Methods Records were sourced from the CENTRAL, EMBASE, and MEDLINE databases. Studies that reported child and parent reported QoL in children with HD and ARM, regardless of surgery intervention, versus children without HD and ARM, were included. The primary outcome was the psychosocial functioning scores, and the secondary outcomes were the presence of postoperative constipation, postoperative obstruction symptoms, fecal incontinence, and enterocolitis. A random effects meta-analysis was used.
Results Twenty-three studies were included in the systematic review, with 11 studies included in the meta-analysis. Totally, 1678 total pediatric patients with HD and ARM underwent surgery vs 392 healthy controls. Pooled parent-reported standardized mean (SM) scores showed better social functioning after surgery (SM 91.79, 95% CI (80.3 to 103.3), I2=0). The pooled standardized mean difference (SMD) showed evidence for parent-reported incontinence but not for constipation in children with HD and ARM after surgery that had a lower mean QoL score compared with the normal population (SMD −1.24 (-1.79 to –0.69), I2=76% and SMD −0.45, 95% CI (−1.12 to 0.21), I2=75%). The pooled prevalence of child-reported constipation was 22% (95% CI (16% to 28%), I2=0%). The pooled prevalence of parent-reported postoperative obstruction symptoms was 61% (95% CI (41% to 81%), I2=41%).
Conclusion The results demonstrate better social functioning after surgery, lower QoL scores for incontinence versus controls, and remaining constipation and postoperative obstruction symptoms after surgery in children with HD and ARM.
- congenital abnormalities
- pediatrics
- gastroenterology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hirschprung’s disease (HD) and anorectal malformations (ARM) are congenital intestinal anomalies, typically manifesting during early infancy, and contribute to symptoms of severe constipation and intestinal obstruction.1–3 HD and ARM affect 1 in 5000 live births with a slight male preponderance (ie, male-to-female sex ratio of 4:1).4–6 Surgical techniques have improved the results of children with HD by decreasing operation time, blood loss, length of hospital stay, and frequency of postoperative complications at 3 years after surgery.7–9 Despite these short-term advantages, bowel dysfunction and enterocolitis persist long-term and can adversely affect the psychosocial health of children with HD and ARM into adulthood.10–13 Quality of life (QoL) is a construct aimed at measuring the physical and psychosocial sequelae of parents and their children afflicted by gastrointestinal diseases.14 15 When applied to medicine, QoL refers to the ‘subjective health status’ of a patient and measures the effect of illness or disease, moving past physician assessment to consider the patient’s well-being and progress.16 17 The results pertaining to the social adjustment of children with ARM are mixed with certain studies reporting difficulties forming relationships,18 elevated behavior problems,19 absence of psychological maladjustment,20 or the presence of emotional disturbance in children experiencing frequent soiling accidents.21 Into older age, the major determinant of QoL continues to be fecal incontinence.22 Multiple meta-analyses have already investigated the short-term and mid-term postoperative outcomes in patients with HD who underwent different surgical approaches, yet the rates of postoperative complications are still variable.23–27
There has been no systematic review and meta-analysis to date, which encompasses multiple social and physical dimensions in a pediatric population with consideration of parent perspectives. Our aim is to conduct a systematic review of existing literature to quantitatively summarize the parent and child-reported psychosocial and physical functioning scores and frequencies of children affected by HD and ARM and in comparison to children without these diseases if data permit.5
Methods
This review followed the Cochrane Methodology to identify and select the studies28 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.29
Search strategy and selection criteria
A systematic search for relevant studies was performed on November 5, 2019 and again on December 17, 2020, identifying six additional studies.6 30–34 MEDLINE, including Epub Ahead of Print, In-Process and Other Non-Indexed Citations, were searched between 1946 to October 25, 2020, Embase from 1947 to 2019 October 25, and the CENTRAL Trials Registry of the Cochrane Collaboration (September 2019 Issue) using the Ovid interface. Searches were designed and conducted by librarian experienced in systematic reviews, using a method designed to optimize term selection.35 Search strategies can be found in the online supplemental file 1). The study protocol has been registered in Open Science Framework (10.31219/osf.io/zqbgx). All duplicate records were removed online, and records retrieved by the electronic search were downloaded and imported into a Reference Manager database, and then uploaded to Covidence (www.covidence.org) for title and abstract screening and full text review. Five reviewers (EB, IO, MK, VG, VL) screened independently at title/abstract level and full text review stages, and citations were excluded if at least two reviewers agreed to exclude; disagreements were reviewed and resolved by the study leads, where necessary (AN). The study colead (IO) reviewed all eligible citations to confirm eligibility.
Supplemental material
Inclusion criteria
Case-control, cohort studies, and randomized-control trials examining child and parent reported QoL in children aged less than 18 years with HD and ARM, regardless of surgery intervention (ie, Duhamel, Swenson, endorectal pullthrough, laparoscopy-assisted pull-through and open pull through), were included.
Exclusion criteria
Case studies, literature reviews, systematic reviews, editorials, letters to the editor, conference abstracts, and commentaries were excluded. Primary studies published before 2007 that were not written in English were also excluded. A previous systematic review captured studies before 2007; hence, why we excluded studies published before 2007.
Data extraction
Three authors (IO, EB, MK) performed data abstraction using a predesigned, piloted, and modified sheet in Excel V.14.7.7, which was validated by our statisticians (LH, VB). The extracted information included the following: study details including study design; type of QoL report (parent proxy or child), length of follow-up, age of children when QoL was assessed, QoL instrument facilitated, threshold for interpreting QoL scales, and parent-reported versus child-reported QoL scores, in addition to the sample sizes of children who presented with physical complications postoperatively.
Outcome definitions
The primary outcome was the mean scores on the psychosocial functioning domains. The secondary outcomes included the followings: reported frequencies and mean scores on QoL instruments of physical symptoms for constipation, intestinal obstruction, fecal incontinence, and enterocolitis. Definitions for each outcome depended on the QoL instrument used (online supplemental file 2, table S1). We defined short-term follow-up as: results from QoL interviews or questionnaires obtained before 2 years from study onset, while long-term follow-up referred to measurements after 2 years. Parents may have reported on study outcomes if children were too young to report themselves.
Supplemental material
Assessment of risk of bias (ROB) within studies
Two reviewers (MK and IO) independently reviewed each study. The validated Methodological Index for Non-Randomized Studies (MINORS) criteria was used to assess the quality of the studies.36 Based on the Cochrane handbook for considering bias, reasons for disagreement were explored and resolved.37 Items assessed included: clearly stated aims, inclusion and representativeness of patients, reliable prospective data collection, appropriate and unbiased endpoints, sufficient follow-up period, follow-up loss, adequate study size calculation, contemporary groups (to address historical bias), baseline equivalence, and adequate statistical analysis.36 Items 1–7 apply to non-comparative studies, while items 8–12 for comparative ones. Records were given scores of zero through two. The maximum (ideal) global score is 24 for comparative studies and 16 for non-comparative studies. One study was a randomized control trial (RCT).38 Therefore, the Cochrane Risk of Bias tool was used. The ROB tool covers six domains of bias: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. Within each domain, assessments are made for one or more items and support for judgment is made by providing a free text description and assigning judgment into high, low, or unclear risk of material bias for each item.39
Statistical analysis
All statistical analyses were performed using the R statistical programming language (V.4.0.).40 Data were meta-analyzed using a random effects model with R package ‘meta’.41 Scores of all QoL instruments were scaled to 0–100 scale using the ‘min-max scaling’ method (Hogg, p. 69).42 All scores were standardized—scores closer to 100 indicated higher or better QoL. Pooled proportions and pooled QoL standardized mean scores with 95% CI were reported in cases of low heterogeneity (I2=75%). In cases of high heterogeneity, the mean scores of individual studies without pooled estimate were presented by subgroups of potential sources of variability: duration of outcome (short 0–2 vs long 2+ years), instrument type, and scale (0–100 vs other). The results were reported separately for the child and parents.
Results
Our initial search yielded 498 studies. After an update was performed, there were 6 additional studies that met our inclusion criteria and 23 (22 observational and 1 RCT) included in the systematic review, with two studies included in the meta-analysis for child-reports and nine for parent-reports (figure 1). One study was excluded, due to patient overlap.22
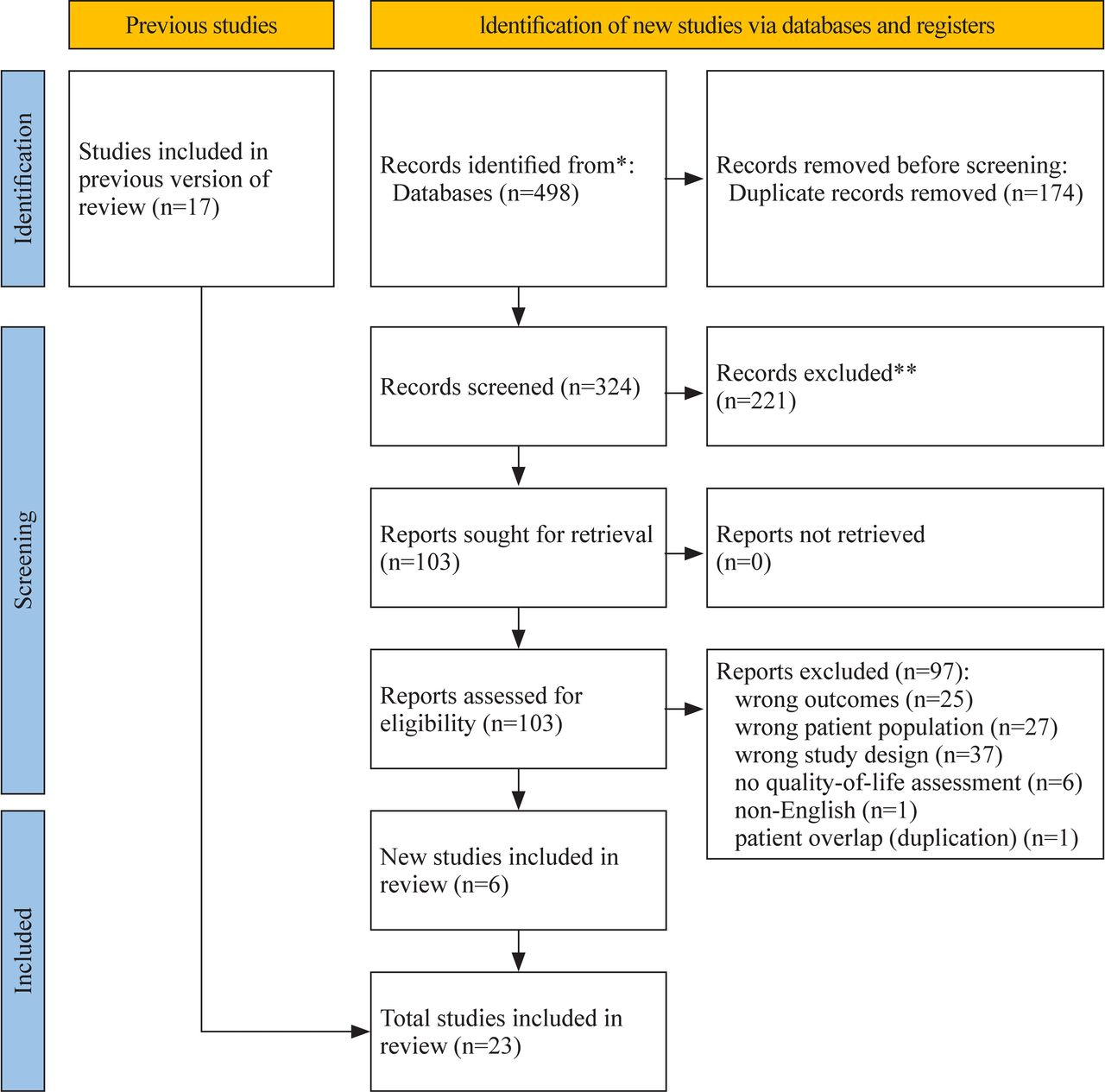
PRISMA flow diagram. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools.29 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics and individual results
In total, 1678 pediatric patients with HD and ARM who underwent surgery vs 392 healthy controls without HD and ARM were included (online supplemental file 3). Children were typically between the ages of 2 and 18 years. A mean age was not reported because the timing of symptom presentation may have differed for each outcome. There were three prospective case control studies,43–45 two prospective case and retrospective control data studies (ie, established controls from literature),5 46 one retrospective case control study,33 nine retrospective cohort studies,32 34 47–53 six prospective cohort studies,6 15 30 54–56 one RCT,38 and one mixed-method sequential explanatory cohort study.31 These studies were implemented in various pediatric centers around the world, including Japan,43 Australia,5 44 the Netherlands,46 48 United Kingdom,30 32 China,33 34 38 52 Sweden,55 Egypt,15 Ireland,47 Finland,53 and the USA.49 51 Prevalent surgical approaches, included the trans anal endorectal pull-through, and the Duhamel methods. No study recruited patients with congenital diseases, neurological defects and other syndromes (eg, Down syndrome). The minimum follow-up was 6 months and maximum was 28 years, for QoL assessment.
Supplemental material
Risk of bias across studies
Two reviewers (MK, IO) independently assessed RoB of the included studies. Common reasons for disagreement, included discrepancies on unbiased endpoints (ie, blinded interviewers for QoL assessments), follow-up period (2 years minimum), and loss to follow-up (<95% loss). The discrepancies were resolved by consensus (online supplemental file, table S3). Online supplemental file, tables S3 and S4 (online supplemental file 4) displays the quality appraisal results. MINORS scores for comparative studies (n=7) ranged from 14 to 20, with mean 16.4±2.1. MINORS scores for non-comparative studies (n=15) ranged from 10 to 14, with a mean of 11.7±1.0. Based on these mean scores, the MINORS criteria suggests fair study quality. Weaknesses in the comparative studies included a follow-up period of less than 2 years, greater than 5% loss to follow-up, insufficient double blinding, and no exploration of confounders or evidence of a statistical test when demographic characteristics differed between cases and controls (age and sex). Weaknesses of the non-comparative studies were: high attrition bias (>5%), no indication for Research Ethics Board (REB) approval, and potential for experimenter bias when administering QoL questionnaires (online supplemental file, table S3). The RCT published by Wang et al38 38 demonstrated fair quality due to absence of reporting bias. A lack of reporting in compliance and social adjustment did not bias additional outcomes such as incontinence (online supplemental file, table S4).
Supplemental material
Primary outcomes
Psychosocial QoL outcomes
Pooled parent-reported mean scores showed better social functioning after surgery (91.79, 95% CI (80.3 to 103.3), I2=0) (figure 2). Due to high heterogeneity for parent-reported emotional and psychosocial domains, only a narrative synthesis is presented, suggesting high emotional and psychosocial scores after surgery (online supplemental file 5). Please refer to the supplementary files that describe the altering of original scores using min-max scaling.
Supplemental material
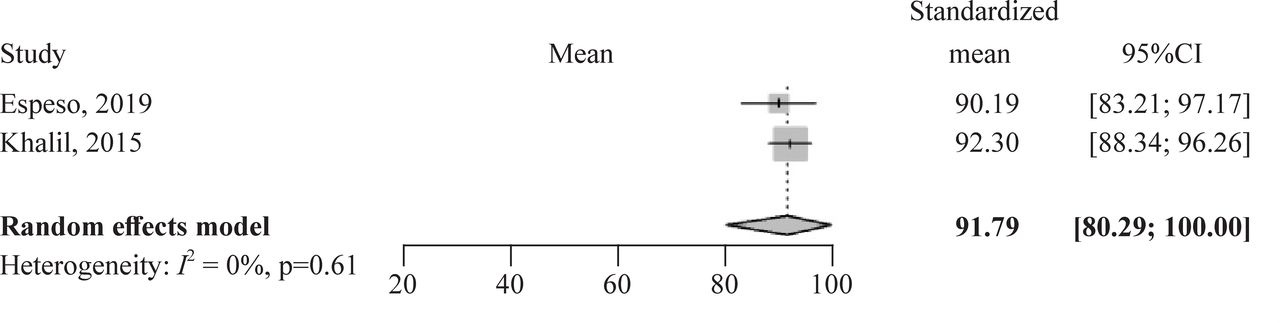
Pooled quality of life score mean estimate and 95% CI for parent-reported social functioning domain for Hirschsprung’s disease only.
Secondary outcomes
Physical QoL outcomes in cases versus controls
The pooled effect for parent-reported shows evidence for incontinence but not for constipation. Children with HD and ARM after surgery have a lower mean QoL score compared with the normal population (standardized mean difference (SMD) −1.24 (–1.79 to –0.69), I2=76% and SMD −0.45, 95% CI (−1.12 to 0.21), I2=75%) (figure 3), respectively. For parent-reported incontinence scores, a subgroup analysis based on instrument type was performed (scale from 0 to 100 vs transformed to 0 to 100). Regardless of instrument type, incontinence scores are high or better after surgery (online supplemental file 5).
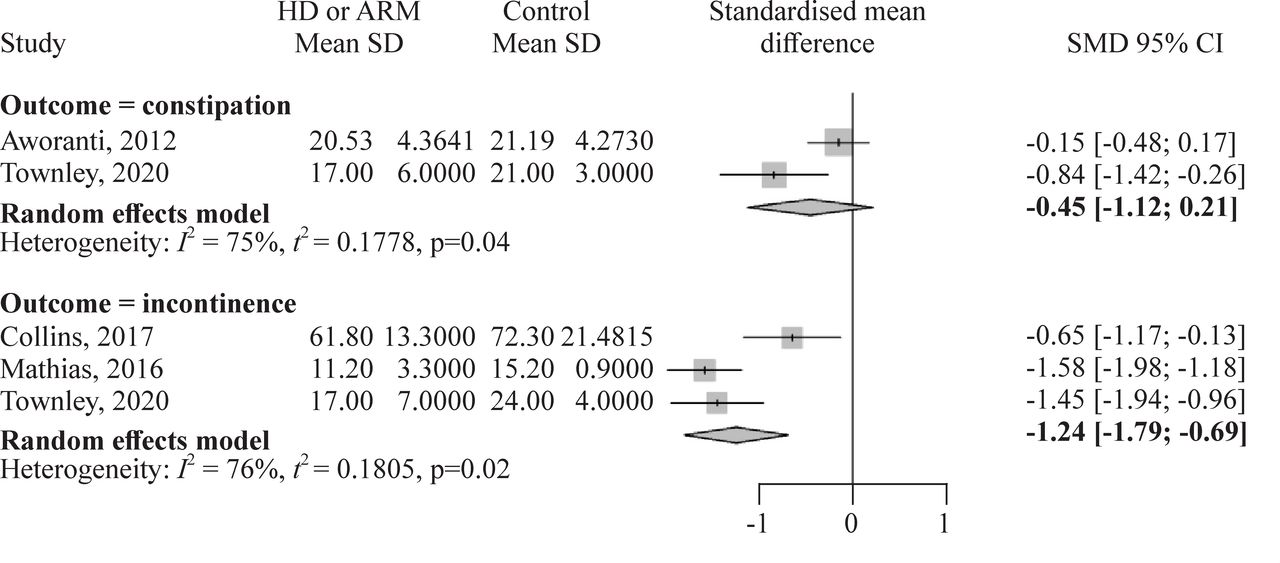
Pooled estimates and 95% CI for parent-reported constipation and incontinence scores. ARM, anorectal malformations; HD, Hirschsprung’s disease; SMD, standardized mean difference.
Physical complications
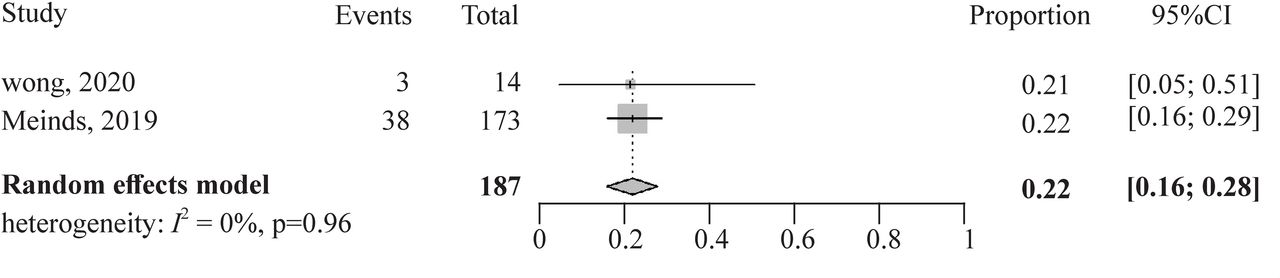
Pooled prevalence of child-reported constipation was 22% (95% CI (16% to 28%), I2=0%) (figure 4). Subgroup mean score for short-term versus long-term parent-reported constipation were showed, with short-term proportions ranging from 4% to 41% and long-term from 8% to 76% (online supplemental file 5). Pooled prevalence of parent-reported obstruction symptoms was 61% (95% CI (41% to 81%), I2=41%) (figure 5).
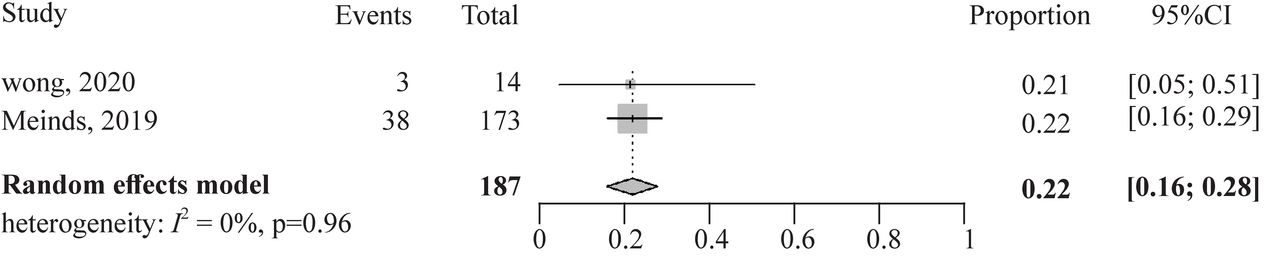
Pooled prevalence plot for child-reported constipation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled prevalence plot for parent-reported obstruction symptoms.
Discussion
The objective of this systematic review was to capture the parent and child-reported psychosocial and physical functioning scores and physical complications of children affected by HD and ARM. Our main, low heterogeneity results demonstrate: (1) better social functioning after surgery; (2) lower QoL scores for incontinence versus controls; and (3) remaining constipation and obstruction symptoms after surgery in children with HD and ARM. In accordance with our findings, previous literature suggests that parents typically report better social functioning, such as good social relationships with friends in their children with HD and ARM.5 57 58 One potential explanation for this finding is that older pediatric patients with chronic disease experience a ‘response shift’, in that they respond to their new reality living with the disease and adjust to functional norms. In other words, they are able to emotionally and mentally shift to living with their chronic disease, giving them feelings of greater control.
This theory might help explain why parents observed better social functioning in their children, based on the internal coping strategies the children may have employed.58–60 However, relying on purely parent responses alone is not the only reliable method for assessing social functioning QoL in children with chronic disease. This is because discrepancies in QoL reporting persist with their children, and a combination of both is recommended.61 In fact, children with HD may report poor psychosocial and social functioning after surgery62 63 in comparison to their parents. Moreover, one systematic review found that children with HD and ARM experience difficulties with anxiety, peer rejection, and behavioral problems, while adolescents report low self-esteem, poor body image, and depression.64
Our review found that children with HD and ARM have lower QoL scores for incontinence versus published controls but no evidence were found for constipation, which is in agreement with another 2021 systematic review65 that did not determine the significant difference of constipation rates (42%) between HD children and the general population, when strict clinical definitions for constipation were used to monitor these patients.1 66 Therefore, when thresholds to qualify as constipation are set high, children may not meet all the criteria at the time of assessment. Hence, constipation rates in our review may be underreported. Additionally, numerous studies have echoed that children with HD have increased or worse incontinence scores and lower physical functioning, compared with age and gender matched controls,5 44 48 67 68 regardless of the QoL instrument used. Interestingly, incontinence scores correlate with lower QoL scores for behavior and self-esteem, unlike in normal controls.46 Plausible reasons why children with HD and ARM suffer from fecal incontinence might be due to increasing severity of fecal incontinence over time, as children age, which consequently negatively affects their QoL.
Conversely, children without these conditions may not experience the same complications.5 In our review, we included children between the ages of 0 and 18 years. Younger patients who have not lived long enough with HD may not cope positively to effectively manage their ongoing functional symptoms, thus reporting poorer physical QoL relative to controls.44 Last, children with only a few functional problems are frequently discharged from follow-up and not transitioned to adolescent or adult care. As such, it is possible that this review underreported the functional problems of constipation and incontinence among cases.48 Twenty-two per cent of children reported having constipation after surgery, while long-term parent-reported constipation was as high as 76% in our review. Parent-reported postoperative obstruction symptoms was 61%, and incontinence ranged from 13% to 68%. Comparing these findings to prior literature is difficult, given that clinical definitions for constipation, postoperative obstruction symptoms, and incontinence vary greatly across studies and may be captured differently based on the data collection method used.65 In fact, certain studies report no HD patients experiencing constipation69 70 vs 30%–76% after surgery.48 66 Similarly, cohort studies document ranges of incontinence from 19% to 82%.44 62 71–76 Long-term follow-up after surgery may increase the ability for researchers to detect the incidence of constipation and incontinence. Moreover, the pediatric population is heterogeneous in that they may present with neurological impairments and syndrome-associated diseases, which are correlated with increased constipation and incontinence scores.1 65 77 No children in studies included in our review possessed such impairments.
Limitations
Limitations of the evidence included in this review mainly stem from the wide variability in child and parent documented psychosocial and physical QoL outcomes, which we attempted to examine via subgroups for instrument type, scale, and duration of outcome. Heterogeneity was likely due to underlying clinical differences in the pediatric population and/or discrepancies between parent and child reports. Furthermore, sample sizes in cohort studies were small, and certain case control studies captured control data from previously established literature, rather than controls recruited during their study. We also surmise that physical complications were more likely to be detected during long-term postoperative follow-up.
Future directions
Given the variability in psychosocial and physical functioning QoL instruments, there is a need to standardize child and parent-reported QoL measurements to improve the robustness and generalizability of the current evidence. Moreover, creating validated, age-specific child QoL measurements would also be beneficial to explore differences in QoL by age. In terms of the complications of constipation and incontinence, standardizing clinical definitions and treatment plans are encouraged. Prospective, multicentered, and longitudinal studies with consistent monitoring of QoL and complications of children with HD and ARM into adulthood, is an area of future research.
Clinical implications
For clinical benefits, postsurgical treatment interventions should target reducing constipation, postoperative obstruction symptoms, and incontinence scores based on consultation with patients and their health risk profile. In order to obtain an accurate perception of child social functioning, more informants (children, parents, teachers) in clinical research are recommended, to support patients and their families after surgery.64 78 79
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank Margaret Sampson, MLIS, PhD, AHIP (Children’s Hospital of Eastern Ontario) for developing the electronic search strategies and Lindsey Sikora, MISt (University of Ottawa) for peer review of the MEDLINE search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Five reviewers (EB, IO, MK, VG, VL) screened independently at title/abstract level and full text review stages, and citations were excluded if at least two reviewers agreed to exclude; disagreements were reviewed and resolved by the study leads, where necessary (AN). The study colead (IO) reviewed all eligible citations to confirm eligibility. Two analysts (LH, VB) were responsible for assisting with the analysis. IO was responsible for writing the final manuscript with assistance from VL.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.