Article Text

Abstract
Background The splenic tumor is relatively rare in children. However, diagnosing and managing this disease remain controversial. This study aimed to evaluate the clinical characteristics and pathological features of benign splenic tumors and to explore the feasibility and safety of laparoscopic splenectomy in children.
Methods The clinical data of all patients who were diagnosed with benign splenic tumors and admitted to our center between January 2014 and December 2020 were analyzed retrospectively. Factors that were documented included demographic criteria, clinical manifestations, preoperative examinations, surgical methods, histopathological characteristics, postoperative complications and outcomes.
Results Totally, 24 consecutive patients with a mean age of 10.21±2.59 years were operated laparoscopically. Nine patients presented with recurrent abdominal pain, vomiting or backache. The remaining 15 cases were asymptomatic and were identified incidentally. Laparoscopic total splenectomy (LTS) was performed in 12 cases, laparoscopic partial splenectomy (LPS) in 9 cases and deroofing of splenic cyst in 3 cases. No significant differences were observed in operation time, intraoperative bleeding and postoperative abdominal drainage between the LTS and LPS groups. Histopathology examination reported 12 cases of splenic epithelial cyst, 5 cases of splenic lymphangioma or lymphatic malformation, 3 cases of splenic hamartoma, 3 cases of splenic littoral cell angioma and 1 case of splenic hemangioma. No postoperative complications and tumor recurrence were observed.
Conclusions It is still difficult to precisely diagnose the splenic tumor preoperatively. Laparoscopic splenectomy is safe and feasible in treating the benign splenic tumors, and partial splenectomy is of great significance in preserving the immune function in children.
- Child Health
Data availability statement
Data are avaliable from the corresponding author upon resonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Benign splenic tumors are relatively rare in children. The pathological features of pediatric splenic tumor have not been fully clarified, and there is still a lack of universally accepted management strategies.
WHAT THIS STUDY ADDS
The results demonstrated that the pathological findings of this disease are diverse and that laparoscopic splenectomy is safe and effective in children. Partial splenectomy is of significant importance in the treatment of localized splenic tumors while preserving splenic immune function.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study may improve the diagnostic accuracy and provide evidence-based solutions for laparoscopic splenectomy of splenic tumors in children.
Introduction
Primary splenic tumors are uncommon in children and only account for 0.64% of the whole body tumors.1 They encompass both congenital and proliferative lesions, as well as benign and malignant tumors, with the majority being benign tumors. There is no consensus on tumor classification owing to complex tissue origins and varied pathological types. Morgenstern et al proposed classifying spleen tumors into four categories: tumor-like lesions, vascular tumors, lymphoid tumors and non-lymphoid tumors.2 Splenic hemangioma is the most common solid benign tumor, while lymphoma is the most common malignant lesion of the spleen in children. Other less common lesions include lymphangioma, hamartomas, littoral cell angioma, fibroma, lipoma, angiosarcoma, and lymphangiosarcoma.3 4 However, the clinical and pathological characteristics of splenic tumors in children remain partially understood owing to the relative rarity of the disease, which affects the formulation of individualized diagnosis and treatment strategies.
Some controversy in managing splenic tumors in children remains.5 Surgical resection is the first choice for treatment of splenic tumors, while debate exists as to whether the lesion can be left alone and with regular follow-up. With the development of minimally invasive technology and a deep understanding of spleen immune function and complications after total splenectomy, more and more attention has been paid to the laparoscopic splenectomy, especially laparoscopic partial splenectomy (LPS) in children. However, only a few reports exist on the laparoscopic treatment of splenic tumors in the literature. Therefore, more evidence is required for the safety and effectiveness of laparoscopic splenectomy in children.
This article study summarizes our experience in laparoscopic treatment of primary benign splenic tumors in children. The clinical, pathologic, and radiologic features may allow a more accurate diagnosis and individualized management of children’s splenic tumors.
Methods
A retrospective study was conducted on pediatric patients diagnosed with splenic tumor admitted to the Children’s Hospital of Zhejiang University School of Medicine between January 2014 and December 2020. Patients with benign splenic tumor and treated by laparoscopy were included in this study; while patients with malignant splenic tumors, operated with the open approach, managed by intervention methods or conservative treatment, were excluded from this study. We recorded the data of demographic characteristics, clinical manifestations, details of preoperative examination, the surgical procedure performed, intraoperative findings, histological results, short-term and midterm complications, and outcomes. The follow-up period ranged from 6 months to 5 years.
All data were processed using descriptive statistical procedures for calculating means, SDs, frequencies, and percentages. Statistical analysis was completed using the SPSS (V.19.0) to perform Student’s t-test. P<0.05 was considered statistically significant.
Results
General clinical data
Totally, 24 children (12 boys and 12 girls) were diagnosed with a benign splenic tumor in our department. The patient’s age ranged from 6.25 to 14.50 years (mean 10.21±2.59 years). Among them, 9 cases were diagnosed by abdominal ultrasonic examination due to intermittent abdominal pain, vomiting, backache or abdominal mass; 2 cases were found during hospitalization because of ‘erythrocytosis’ and ‘precocious puberty’; the remaining 13 cases were asymptomatic, found accidentally during outpatient ultrasonography. No obvious hematological disorder, such as anemia or thrombocytopenia, was found. However, the masses gradually increased in size during the observation period. In one case of splenic cyst complicated with infection, percutaneous drainage and antibiotics treatment were performed initially and laparoscopic splenectomy was postponed for 6 months later. Two cases of splenic cyst underwent ultrasound-guided percutaneous ethanol perfusion; no obvious regression was obtained, and they resorted to surgery.
Imaging examination
Preoperative workup included sonographic examination in all patients, CT in 19 cases and MRI in 12 cases. The imaging revealed a splenic cyst in 12 cases, hemangioma in 9 cases, hamartoma in 1 case and unidentified results in 2 cases (figure 1). The diagnostic rate of preoperative imaging was 58.33% (14 of 24) only, as proven by histopathological results. The tumors were located in the upper pole of the spleen in 7 cases, the lower pole in 10 cases, diffusely distributed in 5 cases and close to the splenic hilum in 2 cases. The average diameter of the tumor was 9.04±3.77 cm, and the median volume of the tumor was 242.12 cm3 (ranging from 86.40 cm3 to 2601.76 cm3).

Imaging examination of splenic tumor. (A–C) Splenic cyst (asterisk). (A) Sonography demonstrated a huge anechoic mass with internal septations and intraocular echogenic debris in the spleen; (B) CT scan showed a thin-walled hypoattenuating, well-defined splenic mass, without contrast enhancement; (C) MRI showed a hyperintense area with sharp margin and uniform homogeneous signal on T2-weighted image. (D–F) Splenic hamartoma (arrowhead). (D) A hyperechoic mass with increased blood flow in the lower pole of spleen was detected on color Doppler images; (E) a well-circumscribed round mass with marked enhancement on CT scan; (F) a well-marginated mass with slightly hyperintense on T1-weighted MRIs. (G–I) Splenic littoral cell angioma (asterisk). (G) A well-circumscribed homogeneous and hypoechoic mass with hypervascular signal was seen in the lower pole of spleen; (H,I) a well-defined mass with obvious enhancement and mottled area can be seen in the lower pole of spleen on contrast-enhanced CT. (J–L) Splenic lymphangioma (arrowhead). (J) Various sized masses with isoechoic and homogeneous signal were detected under sonography; (K) multiple thin-walled low-attenuation masses with sharp margins and no significant contrast enhancement were seen on CT scan; (L) multiple heterogeneous masses with slightly long T2-weighted signals and focal short T2-weighted signals under MRI. Asterisks and arrowheads indicate lesions.
Surgical methods
Laparoscopic total splenectomy (LTS) was performed in 12 patients with giant masses, multiple occupying lesions, unknown tumor nature, or tumors located near the splenic hilum. LPS was performed in nine patients with localized lesions in the upper or lower pole of the spleen. LPS was difficult to perform in three cases as splenic cysts were located near the splenic hilum; thus, they underwent cyst deroofing.
After general anesthesia, the patients were placed in semilateral right decubitus and slightly reversed Trendelenburg position. A 12 mm periumbilical optical port was positioned by the Hasson technique. The other two 5 mm ports (8 mm ports in robotic-assisted laparoscopy) were placed in the upper middle abdomen and parallel to the umbilicus in the left mid-clavicular line. A traction stitch was sewed when necessary. LPS (including two cases performed under the da Vinci surgery system) was performed on nine patients (figure 2). The perisplenic ligaments were dissected to mobilize the resecting pole of the spleen. After carefully dissecting and exposing the splenic hilum, the splenic lobar vessels going towards the pathologic lesion of the spleen were selectively ligated with hemolock or silk thread. A harmonic scalpel (Ethcion, New Jersey, USA) was used to transect the splenic parenchyma within 1 cm of the well-defined demarcation line of the ischemic zone. Hemostasis of the cutting surface was obtained using electrocauterization (Covidien, Missouri, USA). A total of 12 cases of LTS were performed. The perisplenic ligaments were dissected, and the splenic pedicle was exposed and ligated by silk thread or clamped by hemolock near the splenic hilum while being careful to avoid damage to the distal pancreas. Finally, the splenophrenic ligament was transected. Three cases of splenic cysts were performed with cyst deroofing, which were unsuitable for partial splenectomy. The cyst wall and septum were removed as much as possible, and the inner membrane of the residual cyst was destroyed by electric cauterization. The spleen was morcellated within the specimen bag and was removed through the slightly enlarged umbilical incision. A closed suction drain was placed routinely in the splenic fossa.

Da Vinci robot-assisted laparoscopic partial splenectomy. (A) A splenic cyst located in the middle and upper pole of the spleen. (B) A clear demarcation of ischemic zone was seen after ligation of the blood vessels to the upper pole of the spleen. (C) The splenic parenchyma was divided within 1 cm of the ischemic line by harmonic scalpel. (D) Adequate blood supply of the reserved middle and lower pole of the spleen.
Histopathological examination
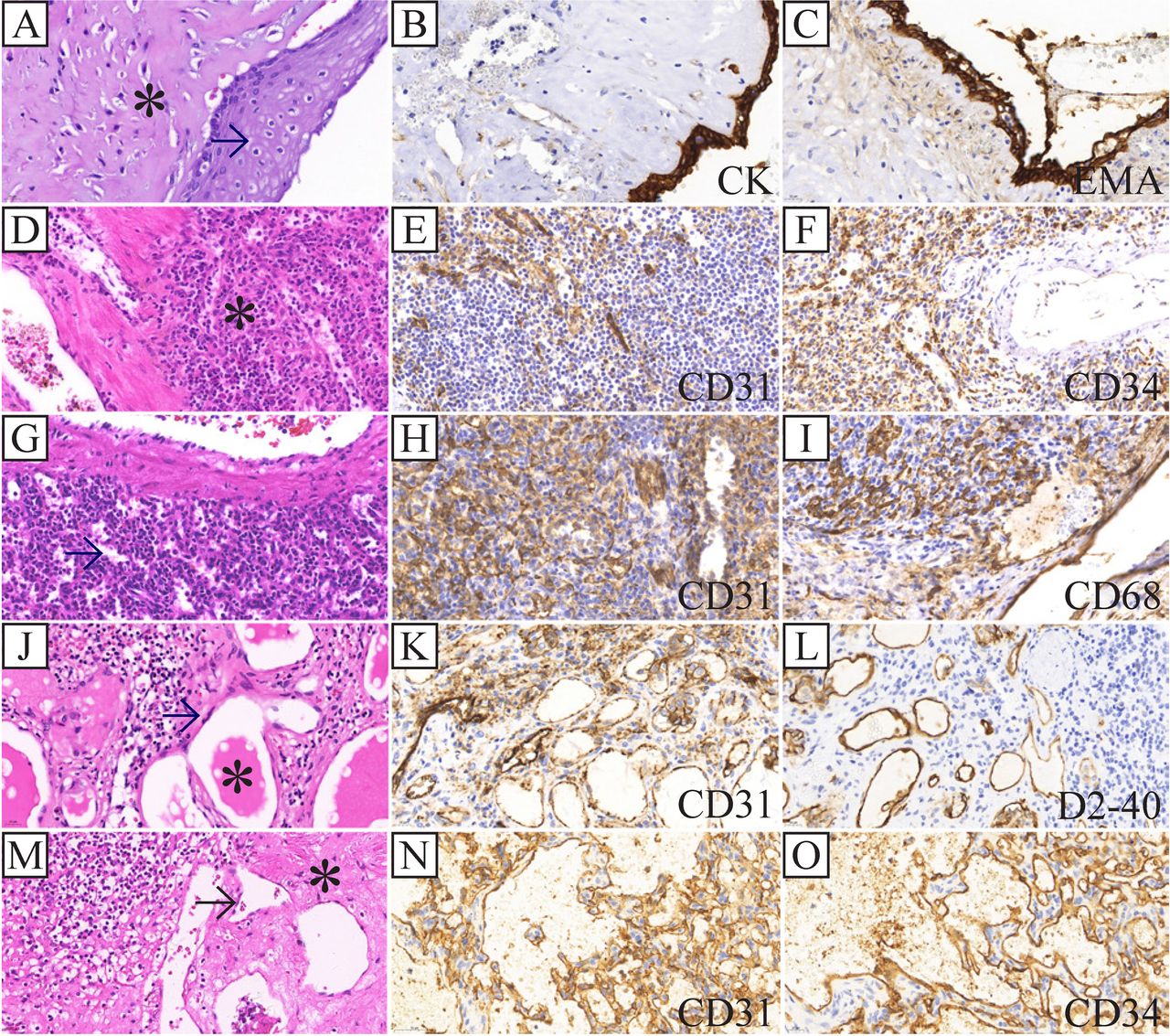
Postoperative histopathology staining (H&E) or immunohistochemistry (IHC) was performed routinely. The pathological results reported 12 cases of splenic cyst (figure 3A–C): 2 cases of splenic hamartoma and 1 case of benign splenic proliferative nodule with foreign body granuloma, which was considered hamartoma with foreign body granuloma (figure 3D–F); 3 cases of splenic littoral cell angioma (figure 3G–I); 5 cases of splenic lymphangioma (including 3 cases of splenic cavernous lymphangioma; 1 case of splenic nodular lymphangioma; 1 case of splenic vascular tumor, which was considered lymphangioma under IHC) (figure 3J–L); and 1 case of cavernous vascular malformation (figure 3M–O).

{kind=link}
{kind=link}
{kind=link}
Pathological and immunohistochemical staining of splenic tumor (×400). (A–C) Splenic cyst. The cyst is lined with squamous epithelium (arrow), with collagen deposition in the cyst wall (asterisk), and positive expression of CK and EMA. (D–F) Splenic hamartoma. The normal structure of spleen was substituted by unorganized vascular channels and hyperplasic red pulp (asterisk), and positive expression of CD31 and CD34. (G–I) Splenic littoral cell angioma. Irregular dilated spongelike vascular spaces (arrow), lined with endothelial cells, and positive expression of CD31 and CD68. (J–L) Splenic lymphangioma. Multiple microcysts are lined with a single layer of flattened endothelium (arrow), filled with eosinophilic proteinaceous material (asterisk), and positive expression of CD31 and D2-40. (M–O) Splenic hemangioma. Multiple different sized lumens lined with flat epithelium (arrow), with interstitial degeneration (asterisk), and positive for CD31 and CD34.
Intraoperative results and postoperative outcomes
All the surgeries were performed successfully under laparoscope, without conversion to laparotomy and intraoperative blood transfusion. There was no significant difference observed in operative time (142.15±32.22 min vs 126.63±30.76 min, p=0.440) or intraoperative bleeding (46.15±13.09 mL vs 57.50±23.90 mL, p=0.371) between LTS and LPS groups. There was less postoperative drainage in the LTS group than in the LPS group (89.25±33.76 mL vs 110.54±43.72 mL), but no significant difference was observed (p=0.090). Compared with the basic platelet count before the surgery, the postoperative platelet level in the LTS group was elevated significantly more than that in the LPS group (2.93±1.11 vs 1.30±0.35 times, p<0.001). After total splenectomy, platelets were routinely monitored for about 2 weeks. The postoperative hospital stay in LTS group (12.46±3.10 days) was significantly longer than that in LPS group (8.75±1.98 days, p=0.020).
Benzathine penicillin was administrated once a month for 1 year to prevent overwhelming post-splenectomy infection (OPSI), and the patients were recommended for vaccination against Streptococcus pneumoniae, Haemophilus influenzae and meningococci. The patients were followed up from 6 months to 5 years, with a median follow-up period of 31 weeks. The platelet level was monitored routinely every 2 weeks for 3 months after operation, and sonography was performed every 3–6 months. No postoperative complications, such as bleeding, pancreatic injury, subphrenic abscess, vascular embolism, intestinal obstruction and severe infection, were observed. There was no tumor recurrence after LTS or LPS. In one case of the deroofed splenic cyst, the residual cyst was slightly enlarged 1 year after surgery and was still under observation.
Discussion
Primary splenic tumors are rare in children, with 60%–76% being benign, whereas splenic cysts and vascular tumors are common.6 Controversy remains in the diagnosis and management of this disease. Surgical resection is indicated for symptomatic or complicated forms, but no guidelines are available for the standard treatment. Total splenectomy has been considered to be the gold standard for the treatment of splenic tumors. Still, it is associated with a risk of serious infectious complications, especially the infection of encapsulated microorganisms.7 OPSI is the most serious complication after total splenectomy. It can occur in as many as 4.4% of the patients with splenectomy and carries a mortality risk of approximately 50%~80%.7–9 With the increased understanding of the spleen’s immunologic function, various parenchyma-preserving procedures are becoming the preferred approach for most pediatric surgeons. However, this approach carries the risk of relatively high tumor recurrence rate.
The primary splenic epithelial cyst is the most common type of splenic cyst observed in children. Most patients are asymptomatic and incidentally diagnosed during abdominal imaging or physical examination. Spontaneous resolution of the small splenic cyst has been reported, and conservative management with close observation has been proposed.10 11 However, medical intervention is recommended when the cyst is symptomatic or larger than 5 cm. Percutaneous aspiration with and without sclerotherapy has been proposed but requires repeated procedures under general anesthesia; moreover, the recurrence rate remains high.12 13 Other reports demonstrated encouraging results for partial cystectomy or deroofing procedures, with short operating times and low complication rates. Nevertheless, the recurrence rate was as high as 60%.14 15 In these 12 cyst cases, 2 cases underwent percutaneous ethanol-based sclerosis and 1 case once deroofing, but no obvious reduction or residual cyst enlargement was observed thus resorted to splenectomy. Three cases of cyst deroofing were performed in this group. The cyst wall was removed as much as possible, the fibrous septa were removed, and the endothelium of the cyst was destroyed by argon beam coagulator or electrocautery to achieve adequate drainage while minimizing the risk of recurrence. Sonography demonstrated small residual asymptomatic cysts remained postoperatively, and one of them was slightly increased in size at 1-year follow-up. Therefore, for giant splenic cysts, total splenectomy should be considered when no obvious splenic parenchyma remains. For localized splenic cysts, partial splenectomy should be the most suitable choice; while for cysts located close to the hilum and unsuitable for partial splenectomy, sclerotherapy or partial cystectomy should be considered.
There is still lack of consensus on treating splenic vascular tumors in children. For asymptomatic masses smaller than 5 cm, close observation is recommended as an appropriate management strategy.16 Many parenchyma-preserving methods have been proposed as well. Satisfactory results have been reported using aspiration, drainage, and irradiation treatment for splenic lymphangiomas and using embolization and antiangiogenic treatment for hemangiomas.17–19 Whether it can maintain long-term remission is still uncertain. However, the biologic behavior of vascular tumors has not been well characterized, and several studies have reported littoral cell angioma with malignancy.20 21 Diagnostic difficulties influence the treatment of splenic vascular tumors, especially for multiple occupying lesions, which cannot be clearly distinguished from malignant lesions. Complete surgical resection is generally accepted as the best choice for splenic tumors with splenectomy or partial splenectomy. The surgical procedure selection must be considered based on the site and size of the tumors, the patient’s age and immune function. For focal lesions with well-defined margins, partial splenectomy or simple tumor resection is a reasonable choice. Total splenectomy is generally required for huge lesions, multiple bulging nodules, tumors with unclear boundaries or unknown properties, and tumors located close to the hilum.
With a better understanding of the spleen’s immunologic function and the end-vascular distribution of intrasplenic vessels, parenchyma-preserving surgical procedures have attracted more and more attention, especially for children with immature immune systems.22 Growing evidence supports that preservation of 25%–30% of the splenic parenchyma with adequate perfusion was sufficient to preserve the immunologic function of the spleen.23 24 Partial splenectomy is an effective method to prevent post-splenectomy infections, but it is often associated with a bleeding risk while separating the parenchyma.22 25 According to the anatomy of splenic vessels, the spleen has distinct segments, where each segment has its artery supply and venous drainage, with an avascular zone between segments. Ligation of splenic artery branches can lead to an ischemic demarcation zone clearly seen on the spleen surface. Dissection of the splenic parenchyma within the ischemia line by LigaSure energy platform or harmonic scalpel can significantly reduce intraoperative bleeding. In our study, nine cases of LPS were performed, with no significant differences in intraoperative hemorrhage, postoperative intraperitoneal drainage and postoperative complications as compared with those of LTS. The postoperative platelet level was significantly lower than LTS, which could significantly reduce postoperative complications, such as vascular embolism and pulmonary hypertension.26 There was no tumor recurrence during the follow-up period. LPS is as safe and effective as LTS for benign splenic tumors. The splenic slices autograft is recommended as an alternative method to preserve the function of the spleen, but in regard of spleen tissue regeneration, blood filtration, reticuloendothelial tissue clearance and immune function preservation, and autologous splenic slices transplantation are not as effective as partial splenectomy.
Laparoscopic splenectomy in the pediatric age group is generally accepted as a technically demanding procedure owing to the limited abdominal space, the fragility of spleen tissue and the relative rarity of splenic disease, especially the splenic tumors.27 Feng et al evaluated the efficacy and complication profile of laparoscopic splenectomy in children during a decade. They concluded that laparoscopy was safe and provided similar outcomes without undue increases in morbidity, duration of stay and mortality and with less traumatic and better cosmetic outcomes.28 A total of 21 consecutive splenic benign tumor cases underwent LTS or LPS in our group, without conversion to laparotomy. After the superior/inferior lobar vessels going toward the lesions were dissected and ligated, parenchymal transection within the ischemia line and careful cauterizing of the residual spleen’s cut surface significantly reduced the intraoperative bleeding. Additionally, the volume of abdominal drainage after LPS was even less than that of LPS. When performing LTS, splenic hilar dissection was carefully performed. First, the splenic artery and vein were ligated in order. Specific attention was paid to the gastrosplenic ligament and the splenophrenic ligaments while performing perisplenic ligament dissection, as the site had insufficient exposure and was prone to bleeding. Owing to the advantages of improved three-dimensional high-definition visualization, enhanced refined movements and additional df, robot-assisted laparoscopic surgery can provide more accurate manipulation than traditional laparoscopic surgery, especially while dealing with the subdiaphragmatic area. Robot-assisted laparoscopic surgery will be a good indication for splenectomy and partial splenectomy.29 30
In conclusion, a definite diagnosis of splenic tumors is still difficult in children, and comprehensive evaluation with various diagnostic methods, including pathological examination, is necessary. LPS does not increase the operation time and intraoperative bleeding, while having advantages in preserving spleen function and reducing postoperative complications. Thus, it should be selected as the preferred method for treating benign splenic tumors in children.
Data availability statement
Data are avaliable from the corresponding author upon resonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee (EC) of Children’s Hospital of Zhejiang University School of Medicine (EC approval number: 2022-IRB-016).
References
Footnotes
Twitter @gzg2k
Contributors CQ—conceptualization, methodology, software, investigation, formal analysis and writing (original draft). LW—data curation and writing (original draft). XC—statistics and investigation. YZ—resources and supervision. LZ—data curation and statistics. KZ—data curation. QX—visualization and writing (review and editing). ZG—conceptualization, resources, supervision and writing (review and editing).
Funding This study was supported by the Natural Science Foundation of Zhejiang Province Programs (grant number LY20H030007).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.