Article Text

Abstract
Objective Pectus excavatum is a congenital deformity characterized by a caved-in chest wall. Repair requires surgery. The less invasive Nuss procedure is very successful, but postoperative pain management is challenging and evolving. New pain management techniques to reduce opioid reliance include the erector spinae plane (ESP) block. We retrospectively examined opioid consumption after Nuss procedure comparing three pain management techniques: ESP block, thoracic epidural (TE), and patient-controlled analgesia (PCA).
Methods This retrospective cohort study compared pain management outcomes of three patient groups. Seventy-eight subjects aged 10–18 years underwent Nuss procedure at our institution between January 2014 and January 2020. The primary outcome measure was opioid consumption measured in morphine milligram equivalents. Secondary measures included pain ratings and length of stay (LOS). Pain was quantified using the Numeric Pain Rating Scale. Analysis of variance was performed on all outcome measures.
Results Average cumulative opioid use was significantly lower in the ESP block (67 mg) than the TE (117 mg) (p=0.0002) or the PCA group (172 mg) (p=0.0002). The ESP block and PCA groups both had a significantly shorter average LOS (3.3 and 3.7 days, respectively) than the TE group (4.7 days). ESP block performed best for reducing opioid consumption and LOS. Reduced opioid consumption is key for limiting side effects. This study supports use of ESP block as a superior choice when choosing among the three postoperative pain management options that were evaluated.
Conclusion ESP resulted in reduced opioid consumption postoperatively and shorter LOS than TE or PCA for patients undergoing the Nuss procedure for surgical repair of pectus excavatum.
- analgesia
- pain
- pediatrics
- thoracic surgery
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Pectus excavatum is a congenital chest wall deformity in which the cartilage connecting the ribs and the sternum does not form properly and results in a large depression in the center of the chest. This condition is commonly found in children, especially males, and often progresses rapidly during puberty. The main indicator for operative repair normally is the correction of the physical deformity. Quantification of defect severity can be performed with multiple imaging modalities or external thoracic measures; severity is most commonly quantified by the Haller index or pectus correction index. These two measures provide a measure of the chest based on cross-sectional imaging, most commonly CT scans. In extremely rare occasions, severe pectus excavatum can result in increased work of breathing due to compression of the lungs, as well as cardiovascular complications due to lateral displacement of the heart.1 Children with pectus excavatum often cannot maintain the same activity level as their peers. When necessary, surgical repair is possible to correct pectus excavatum.1
Although originally corrected through an open surgical approach, since the 1990s, surgeons have performed on a widespread basis a more minimally invasive repair of pectus excavatum, known as the Nuss procedure. In the Nuss procedure, a curved bar is fed through the anterior mediastinum and flipped 180 degrees, immediately correcting the concave curvature of the chest by pushing the sternum and ribs into position. The Nuss procedure has quickly become the favored technique for surgical correction of pectus excavatum, with surgeons generally recommending the operation between the ages of 12 and 14 years.2
Despite its success and benefit of being less invasive, the Nuss procedure is associated with high levels of postoperative pain. When compared with previous open surgical techniques, such as the Ravitch method, the Nuss procedure results in higher pain ratings and greater opioid use in the days immediately following surgery.3 For this reason, many analgesic approaches have been proposed and used postoperatively with the goal of minimizing pain, recovery time, opioid use, and adverse side effects. Some of these approaches include using patient-controlled analgesia (PCA), continuous thoracic epidural (TE) infusions, multimodal analgesia, subcutaneous catheters, intercostal blocks, and cryotherapy.4 5 Despite extensive research on the subject, no single method has yet been deemed indisputably superior for pain management following pectus excavatum, and methods vary widely among individual hospitals and groups.
A relatively new analgesic method, the erector spinae plane (ESP) block, has recently been used for pain management in a wide range of pediatric thoracic and abdominal procedures. This regional method involves continuously infusing local anesthetic in a plane below the erector spinae muscles to work at the origin of the spinal nerves. Recently, the ESP block has been used for pain management following pectus excavatum surgery, with a variety of goals including decreasing opioid use and length of stay (LOS).
Methods
Participants and procedure
A retrospective chart review was performed to compare opioid use, numeric pain ratings, and LOS between three patient groups who underwent the Nuss procedure for correction of pectus excavatum. The three groups were divided into those who received ESP block, TE infusion, and PCA. When used for pain management after the Nuss procedure at our institution, ESP catheters are placed bilaterally with the tips at the mid-thoracic (T4–T6) level. A urinary catheter is not required as urinary retention is exceptionally unlikely. At our children’s hospital in Florida, the most commonly used local anesthetic for this purpose is ropivacaine 0.2% with 1 μg/mL of clonidine. The local anesthetic is administered via programmed intermittent bolus to maximize the spread of local anesthetic in the plane of injection. Programmed intermittent bolus has shown convincing advantages over continuous infusion for epidural anesthesia5 and could be expected to also be beneficial for the block, which relies on spread of local anesthetic in an interfascial plane. The use of bilateral ESP blocks for pain management after the Nuss procedure using programmed intermittent bolus has been reported previously.6 7 Because bilateral ESP block uses two catheters, the set up and ongoing management does require additional time investment on the part of the pain service.
This study included patients who underwent the Nuss procedure for pectus excavatum at our children’s hospital for a period of 7 years from January 1, 2014 to January 31, 2020. All patients were between the ages of 9 and 18 years. This study included healthy patients with an American Society of Anesthesiologists score of 1 or 2. Exclusion criteria were those patients with an American Society of Anesthesiologists score of 3 or higher, or if they received two or more other analgesic options.
Outcomes
The primary outcome for this study was opioid use after surgery. All opioids consumed after surgery and before discharge were converted to morphine milligram equivalents (MME) for each patient. Next, total opioid use was calculated for each patient for the following time frames: 0–6 hours, 6–12 hours, 12–24 hours, 24–48 hours, 48–72 hours, and 72+ hours after surgery. In addition, cumulative opioid use throughout the entire hospital stay was calculated for each patient.
The secondary outcomes for this study were LOS, numeric pain ratings, emergency department visit (ED visit), readmissions, and refills of opioids. The LOS was defined as the time between the end of surgery and the patient’s discharge from the hospital. Pain was quantified using the Numeric Pain Rating Scale (NPRS) and was scored on a scale of 0 to 10, with 0 equals no pain, 5 moderate pain, and 10 worst possible pain. Pain ratings were averaged for each patient during the following time frames: postanesthesia care unit arrival (0 hours) up to 6 hours later, then 6–12 hours, 12–24 hours, 24–48 hours, 48–72 hours, and >72 hours after surgery. In addition, pain level was averaged for each patient throughout the entire hospital stay. We looked at the Haller index of each patient, calculated the mean on each pain group, and compared the difference of index between groups of different outcomes (opioid consumption, LOS, pain scores, readmission, ED visits, or refills). The Haller index is calculated by dividing the transverse diameter of the chest by the anteroposterior diameter of the chest at the axial level with the shortest distance between the sternum and the anterior vertebral body.
Statistical analysis
We compared the difference of characteristic and outcomes of patients among groups by Student’s t-test (two groups) or χ2 test (three groups) for categorical variables and analysis of variance (ANOVA) analysis for continuous variables, respectively. Shapiro-Wilk test and Levene’s test were performed to assess normality of the data and homogeneity of variances of each group, respectively. For variables that are fewer than five patients in the subgroup, Fisher’s exact test was applied for analysis. When significant differences were found between groups using ANOVA, post hoc Tukey’s Honest tests were performed to assess which groups differed significantly. The relationship between the Haller index and opioid consumption, LOS, and average pain level was analyzed using Pearson’s correlation.
Results
Patient characteristics
Seventy-eight patients were included in this study, including 67 males and 11 females. Nineteen patients received an ESP block, 41 received a TE, and 18 received PCA. There was no significant difference in the relative number of males and females (p=0.122) or age (p=0.505) among groups (table 1). There were two readmissions from the total of 78 patients, a 2% readmission rate. Female patients had higher rate of readmission than male patients (2/19 vs 0/67, p=0.019).
Demographic characteristics and outcomes among three groups who received erector spinae plane (ESP) block, thoracic epidural (TE), and patient-controlled analgesia (PCA)
Primary outcome
All assumptions for use of ANOVA were met. For the primary outcome of cumulative opioid use as well as the secondary outcomes of average pain level and LOS, the Shapiro-Wilk test and Levene’s test failed to reject the null hypothesis of normality of data and homogeneity of variance, respectively, with all p values being >0.05.
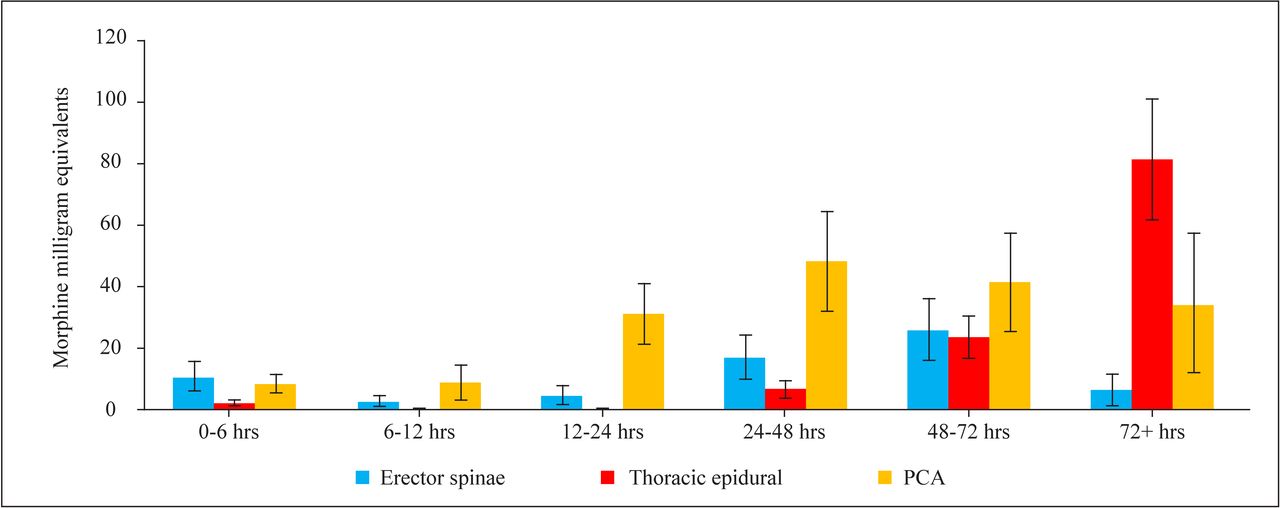
Cumulative opioid use was found to be significantly different among all three groups (p<0.001). Patients who received ESP block had significantly lower average cumulative opioid use (66.9 MME) than those who received TE (117.0 MME) and PCA (172.1 MME) (table 1). The ESP block resulted in a significant reduction in average opioid use >72 hours after surgery (6.3 MME), especially when compared with patients receiving a TE (81.4 MME) (figure 1).
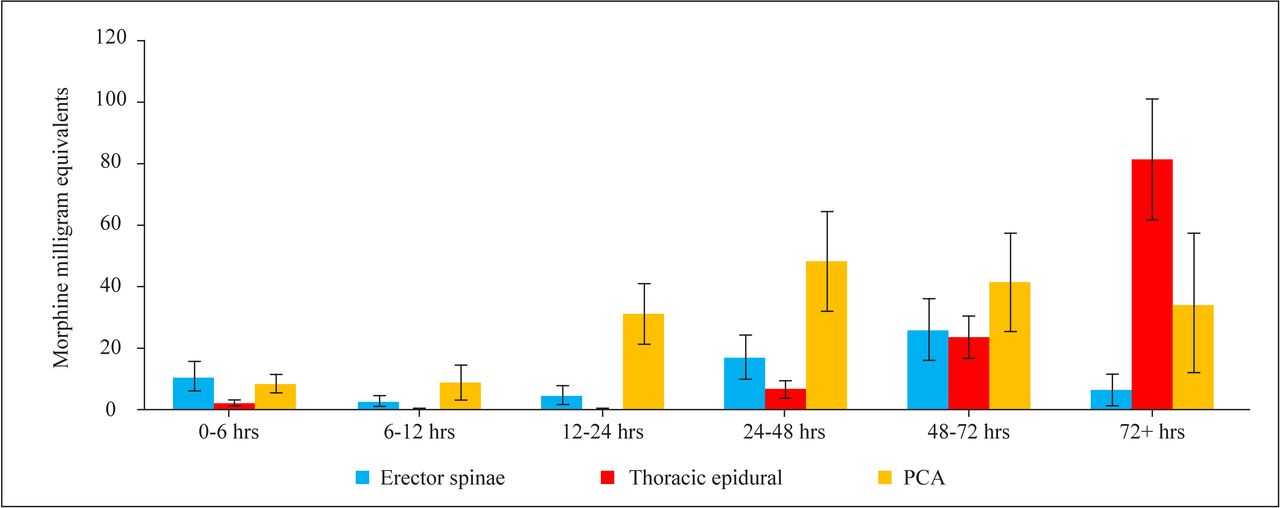
Average opioid use over time in patients receiving an erector spinae plane block, thoracic epidural, or patient-controlled analgesia (PCA) with error bars showing 95% CIs.
Secondary outcomes
Average LOS of patients was found to be 3.3 days in ESP group, 4.7 days in TE group, and 3.7 days in PCA group, respectively. The ESP group had the shortest LOS of all three groups, and it was significantly shorter than the average LOS for the TE group (p<0.001) but not significantly shorter than the PCA group (p=0.307). Average overall pain ratings were found to be 4.5 for the ESP group, 3.4 in the TE group, and 4.1 in the PCA group. The ESP group had the highest overall average pain rating, and it was significantly higher than the TE group (p=0.032) but not significantly higher than the PCA group (p=0.746). There was no significant difference found between the groups with regard to number of ED visits (p=0.616), readmissions (p=0.563), or refills of opioids (p=0.995).
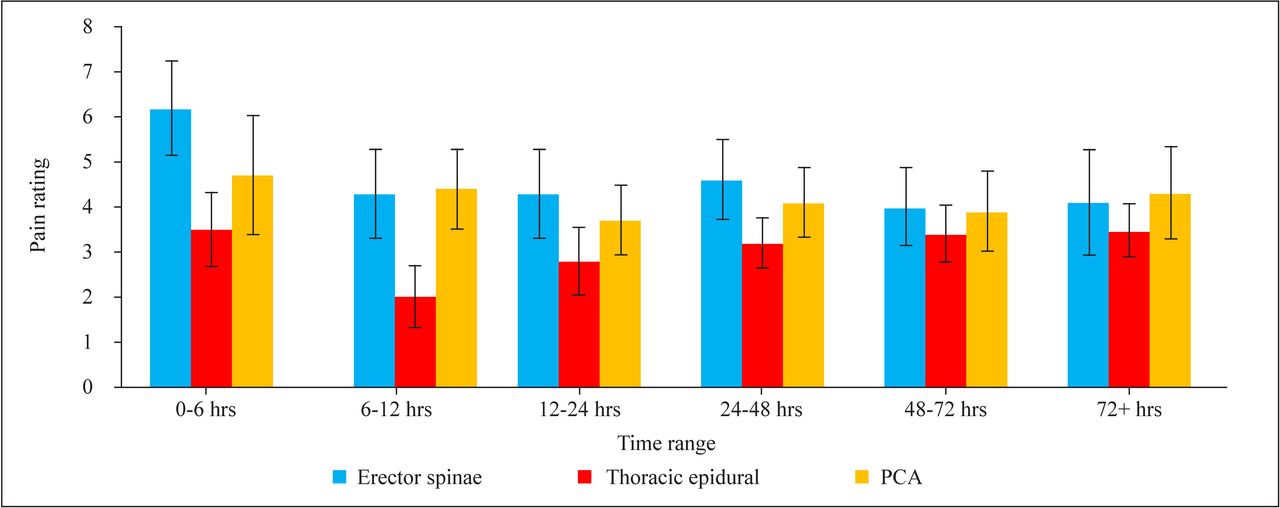
Average pain level varied over time in patients in each group as shown in figure 2. Between 0 and 48 hours after surgery, patients in the ESP group had significantly higher average pain ratings than patients in the TE group. There was no statistically significant difference in pain levels between any of the groups >48 hours after surgery.
{kind=link}
{kind=link}
Average pain ratings over time in patients receiving an erector spinae plane block, thoracic epidural, or patient-controlled analgesia (PCA) with error bars showing 95% CIs.
Finally, we decided to look at the Haller index of all patients, compare the difference between groups with different treatments and outcomes of readmissions, ED visits, and refill requests and explore its correlation with opioid consumption, LOS, and average pain level. The mean Haller index was 5.7 across all patients. There was no statistical difference in Haller index between each treatment group and groups with different outcomes (table 2). Haller index was found to be positively correlated with LOS (r=0.266, p=0.022), that is, the larger the Haller index, the longer LOS duration of patients in the hospital. No correlation was found in Haller index and cumulative opioid use or average pain levels.
Difference of Haller index in patients with different sex and outcomes (ED visit, readmission, refill of opioids)
Discussion
Postoperative analgesia after the Nuss procedure for repair of pectus excavatum is challenging. There are advantages and disadvantages to each of the three pain management approaches evaluated in this study.
Difference in total opioid consumption, which is objectively measurable and arguably of great importance from a clinical perspective, was the primary outcome measure. Limiting opioid consumption will reduce the myriad of complications associated with its use, such as nausea, vomiting, constipation, respiratory depression, opioid induced hyperalgesia, and tolerance.8 9 Additionally, reducing opioid use is also beneficial from the standpoint of reducing the potential for addiction, an important consideration, vis-à-vis the opioid epidemic.10 11 In the present study, we found 20 patients who received opioid refills. This finding had no statistical significance with any particular pain management study group, or any relationship with the LOS opioid consumption inpatient or pain scores. The opioids refills patients also had no relationship with the Haller index.
PCA is relatively easy to implement and does not require any advanced technical skills. There is a risk of respiratory depression,12 which is mitigated as the patient needs to be alert enough to press the PCA button to trigger a dose of opioid. Nevertheless, when used, a continuous basal rate of narcotic could lead to opioid accumulation. Close monitoring is important, and at our institution this includes continuous pulse oximetry.
TE have been very successful in reducing postoperative pain after the Nuss procedure.2 3 Placement of the epidural requires considerable technical skill, and there is a risk of complications. Spinal cord damage,13 although rare, is the most feared potential complication and has resulted in rejection of this pain management option by some centers, including a center that pioneered this surgical technique.14
ESP block, which has the potential to be helpful for pain management after the Nuss procedure, is a more recently developed procedure.15 The block is performed under ultrasound guidance and is relatively easily mastered owing to the usually superficial bony (transverse process) target. Complications are extremely uncommon,16 and because of the greater distance from the neuraxis, damage to the spinal cord is highly unlikely. The first publication evaluating ESP block in Nuss repair was published by Bliss et al, where they found good feasibility and decreased LOS compared with thoracic epidural analgesia.17 We conducted a PubMed search and did not find any reports of permanent neurological sequalae due to ESP blocks. Pneumothorax18 and local anesthetic systemic toxicity19 are significant complications, which (although rare) need to be considered. In a pooled review of 242 ESP blocks published in 2018,20 a single pneumothorax was the only reported complication. In 2020, a meta-analysis of randomized controlled trials of ESP blocks evaluated 679 patients with no block-related complications reported.21
The PCA group had the highest cumulative opioid consumption (figure 1). Confirming one of our hypotheses, there was less cumulative opioid consumption in the ESP group than the TE group. More detailed analysis explained this outcome by elucidating that the TE group had considerable opioid consumption after epidural withdrawal (figure 2). Most acute pain clinicians will agree that there is a challenge of transitioning postoperative patients off their epidurals. Epidurals often provide outstanding postoperative analgesia,2 3 even beyond what is reflected by the NPRS. Unfortunately, this seems to create an unrealistic pain-free expectation from patients, and weaning the epidural often results in rebound pain and ensuing robust opioid demand. Figure 2 clearly shows how there is a marked increase in opioid use at the 72+ hours interval in the thoracic epidural group. Admittedly, the 72+ hours period represents on average a longer time in the TE group because their LOS was about 1 day longer than the other two groups (see figure 2). Nevertheless, it was because of difficult pain control (requiring intravenous opioids) after epidural discontinuation that the TE group had a longer LOS.
Assessing the efficacy of analgesic techniques is complex, and the NPRS has limitations.22 Pain, by its very nature, is a subjective experience and assigning a number to it can be influenced by many factors. The NPRS may be more helpful to track changes in pain perception over time in a specific patient and less helpful for comparing the pain experience between patients.2 Keeping in mind the limitations of the NPRS, we note that our study did show a statistically significant lower NPRS in the TE group (3.4) vs the ESP group (4.5) between 0 and 48 hours after surgery (p=0.032). This finding is what we would expect based on our own subjective observation of these patients. Patients with a TE in place generally appear more comfortable to the clinician observer than the NPRS that they report. There was not a statistical difference in NPRS between the ESP group and the PCA group.
It is noteworthy that average hospital LOS was statistically significantly shorter in the ESP group (3.3 days) and PCA group (3.7 days) when compared with the TE group (4.7 days). Ability to ambulate and independence from the need for intravenous analgesia are key requirements for discharge home. There are likely several underlying possible reasons for a shorter LOS in ESP and PCA patients, which include the following:
The TE patients are usually very comfortable while the epidural is in place; however, transitioning off the epidural is challenging as mentioned before.
It has been our practice at Nemours Children’s Hospital, Florida to initially keep indwelling urinary catheters in place postoperatively.23 While a urinary catheter is not absolutely required with a thoracic epidural, the rationale behind this practice is a desire to avoid unpleasant, unscheduled insertion of a urinary catheter for urinary retention in an awake adolescent. It is the impression of the authors that an indwelling urinary catheter may slow down mobilizing the patient because of reluctance to ambulate with it in place, thus perhaps contributing to an increased LOS.
The ESP plane and PCA groups of patients did not have indwelling urinary catheters postoperatively, and it is our impression that they ambulate more readily and quickly postoperatively. Other reasons for quicker ambulation may also exist. For example, TE patients may have some extremity weakness even though we strive to avoid this.
It has been our practice at Nemours Children’s Hospital, Florida to offer patients with ESP blocks the option of discharge home with the ESP catheters still in place and ongoing continuous infusion using a disposable elastomeric pump. This option will allow patients to continue to receive the benefits of their block for another 2–3 days after discharge home. We remain in close telephone contact with such patients after discharge until the catheters are self-removed at home.
This study is retrospective and, as such, all limitations of this design are applicable. The patient groups were not randomly assigned. The pain management technique selected was determined mostly based on patient and parent preference. We did not have a matched cohort control study group as it was not feasible given the small number of patients in the ESP block group. The ESP block was introduced to Nemours Children’s Hospital, Florida in the summer of 2019. Prior to this, families were counselled regarding TE (risks and benefits), and the families decided whether they wanted a TE for pain management after pectus repair. If the TE was declined, the patient would have PCA postoperatively by default. In the summer of 2019, the bilateral thoracic ESP block was introduced as an option. Because of perceived advantages of the ESP block (no urinary catheter, no risk of severe neurological injury, option of outpatient infusion), it emerged as the primary alternative to PCA.
In conclusion, immediate postoperative opioid consumption after the Nuss procedure is low in patients with a TE in place, but the total cumulative opioid consumption is substantially higher than patients managed with bilateral thoracic ESP blocks. Rebound pain after epidural discontinuation results in substantial opioid demand. The availability of home local anesthetic infusion via ESP catheters allows for earlier discharge home and lowers cumulative opioid consumption. In addition, ESP catheters have a favorable risk profile when compared with TE. If the goal is to minimize opioid consumption and to decrease the hospitalization days, this study strongly supports bilateral ESP blocks over TE and PCA for pain management after the Nuss procedure.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study has been approved by the Institutional Review Board of Nemours Children’s Health, Florida. The study was performed according to the Declaration of Helsinki.
Acknowledgments
We would like to thank our Pediatric Surgery colleagues, especially Drs Andre Hebra and William Adams, for supporting the quest for better analgesic techniques and for being open to exploring the use of newer techniques to benefit our patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LS was involved in the conceptualization; acquisition, analysis, or interpretation of data for the work; drafting the article and revising the work critically for important intellectual content. JD was acquisition, analysis, or interpretation of the data for the work; drafting the article. NFC acquisition, analysis, or interpretation of the work; revising the work critically for important intellectual content. LS, JD, NFC all approved the final version and are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.