Article Text

Abstract
Objective To establish reference intervals (RIs) for fetal and neonatal small and large intestinal lengths.
Methods Linear measurements on small and large intestines were made upon postmortem examination of 131 preterm and term infants with gestational ages between 13 and 41 weeks. All cases were referred from the Eastern Ontario and Western Québec regions to a tertiary care hospital. Age and sex partitions were considered and RI limits were estimated.
Results Data consisted of 72 male (54.96%) and 59 female (45.04%) fetuses and neonates with mean gestational age of 25.6 weeks. Results showed that small and large intestinal lengths increased linearly with gestational age. RIs for small intestinal length (cm) of fetuses and neonates aged 13–20 weeks were (21.1, 122.4); of those aged 21–28 weeks were (57.7, 203.8); of those aged 29–36 weeks were (83.6, 337.1); and of those aged 37–41 weeks were (132.8, 406.4). RIs for large intestinal length (cm) of fetuses and neonates from the same four age groups were (5.1, 21.4), (12.7, 39.7), (32.4, 62.4), and (29.1, 82.2).
Conclusions Establishing accurate RIs for premature and term infants has clinical relevance for pathologists performing postmortem analysis and for surgeons planning postoperative management of patients. The results of this study reaffirm that fetal small and large intestinal lengths increase linearly with gestational age irrespective of sex. Future studies should aim to further investigate the role of possible confounders on growth of fetal intestinal length, including maternal factors such as age and substance use during pregnancy.
- pathology
- fetal medicine
- fetal development
- multiple births
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Research into fetal and neonatal intestinal lengths is frequently decades old and may not reflect current fetal growth patterns in a Canadian population.
Reference intervals (RIs) are derived from ‘normal’ defined populations and distinguish normal versus abnormal cases in a population.
RIs are used in the postmortem examination of fetuses and infants.
The primary objective of this study was to establish fetal and neonatal RIs for small and large intestinal lengths.
What this study adds
This study provided age-specific RIs for normal small and large intestinal lengths of fetuses and neonates.
The results reaffirm that fetal small and large intestinal lengths increase linearly with gestational age irrespective of sex.
Future studies should aim to investigate the role of possible confounders on growth of fetal intestinal length.
How this study might affect research, practice or policy
Pathologists can compare our data to other studies that have established reference standards for normal intestinal length.
Surgeons can communicate how much intestine is remaining in infants with parents and plan postoperative management accordingly.
Further research can explore the impact of gestational weight on intestinal length and can compare such results to established RIs.
This will aid in better understanding of the differences in intestinal length between normal and pathological fetuses.
Introduction
At present, normal growth for fetal and neonatal intestinal lengths is reported in the literature1–4; however, this research is frequently decades old and may not reflect current fetal growth patterns in a Canadian population.5 Moreover, there seems to be less evidence investigating the impact of factors, such as intrauterine growth restriction (IUGR),6 7 multiple gestation and chromosomal defects, on infant gastrointestinal length as opposed to bowel length.8 Small bowel length is estimated to be 250±40 cm at birth. While its growth has initially been thought of as linear, the small bowel grows rapidly in the last 15 weeks reaching its maximal growth during the first year of life.3 4 Given such rapid changes in fetal bowel growth, the application of reference intervals (RI) based on gestational age in a clinical setting has a significant value.
Creating reliable RIs may have relevance in assisting surgeons to appropriately prognosticate and to form postoperative plans for infants undergoing bowel resection for conditions such as Hirschsprung’s disease and necrotizing enterocolitis.3 9 Length of small bowel, for example, can predict the need for bowel transplantation in infants with small bowel syndrome.10 Determination of normal fetal measurements is additionally important for pathologists conducting fetal postmortem examination and assessing fetal growth and development. Creating reliable RIs may assist pathologists in guiding further screening for congenital anomalies associated with small bowel syndrome11 and in properly defining pathological bowel length, which is often defined in terms of rough estimates without accounting for the gestational age of the fetus.11–13
Statistically, RIs are derived from ‘normal’ defined populations and communicate two limits (upper and lower limits) to distinguish normal versus abnormal cases in a population.14 They are used to examine organ and body weights including linear measurements, which are particularly important during the postmortem examination of fetuses and infants.15 16 The Clinical and Laboratory Standards Institute (CLSI) has established guidelines to ensure accuracy of RIs. The purposes of these guidelines are to identify reference subjects, to provide guidance on statistical methods, to discuss options for detecting and removing outliers, and to describe partitioning according to age, sex or other relevant categories.17 18 Specific challenges in establishing pediatric RIs arise owing to the changing physiology of infants, the confounding relationship between gestational age and body size on intestinal length, and limitations in sample size.19–21 A recent paper, which focused on evaluating optimality of the various statistical methods for estimating RIs, showed that the choice of statistical methods in RI estimation is crucial in ensuring accuracy and precision and that researchers should consider the distribution, sample size and heterogeneity of data in making the optimal choice.21 In the present study, we followed the recommendations provided as well as the steps provided in the CLSI guidelines.
The primary objective of the present study was to establish fetal and neonatal RIs for small and large intestinal lengths using data on the Eastern Ontario and Western Québec population. Sensitivity analysis was applied to correct for a variety of fetal factors and pregnancy complications.
Methods
Study population
Data were obtained from the Children’s Hospital of Eastern Ontario (CHEO), where samples from March 2015 through December 2018 were evaluated. All autopsies were performed at the Department of Pathology at CHEO (Ottawa, Canada). An experienced pathologist followed strict, standardized protocols when conducting placental examinations and perinatal autopsies. Clinical and ultrasound imaging data were reviewed and verified intracorporeally and extracorporeally to confirm the presence or absence of gastrointestinal anomalies or disease.
Intestinal length measurements comprised the regular postmortem examination. As part of the routine postmortem procedure, each organ (eg, the small and large intestines) was eviscerated individually.3 The only additional procedure performed for this study included measurement of the small and large intestinal lengths. Clinical data in terms of the estimated gestational age, determined by the date of the last menstrual period, foot length, crown-heel length, and weight, were abstracted from chart reviews.22 Degrees of maceration (grades 0–III) were used to estimate timing of fetal death in order to adjust the gestational age.23 Data on the sex and ethnicity of the patient as well as their weight and crown-heel length also were abstracted from charts.
Sample collection
Linear measurements of intact small intestine and colon were obtained at autopsy. The cohort includes all autopsies from 2015 to 2018. The gastrointestinal tract was removed from the esophagogastric junction to the pelvic floor and the anal verge. The esophagus and stomach were opened and carefully dissected. Small intestine and colon were measured twice in centimeters using a measuring tape and/or plastic ruler. The small intestines were very convoluted; thus, the pathologist (DED) laid the specimens on a moist plastic surface, stretched them out and pinned them. There were no loops or curves after specimen stretching. The small intestinal length was defined as the distance between the ligament of Treitz and the ileocecal valve,2 whereas the colon length was measured as the distance from the beginning of the appendix to the anal verge.
Statistical analysis
We followed the steps provided in the CLSI guidelines in establishing the RIs provided in this paper, where partitioning with respect to age and sex was considered.18 We also followed the recommendation provided by Daly and colleagues in selecting optimal statistical methods for estimating the reference limits within each of the partitions.20 As such, for each partition, we first evaluated the distribution of intestinal length using formal statistical tests as well as graphical investigations using scatter plots and probability plots. Variability and skewness of data as well as sample size within each partition were considered in choosing an optimal method for estimating both the lower and upper reference limits of each partition.
Sex partitioning was initially considered, but the results showed no difference in intestinal length between males and females. To maximize sample size, and hence to provide more precise estimates, we provided RI estimates for the combined population. For both the small and large intestines, we observed that the measurements increased linearly with respect to gestational age, which indicated that narrow age partitions were required. Therefore, we created narrow partitions as data permitted. For comparison purposes, we also provided RI estimates for wider partitions. The partitions we considered included: 13–20, 21–28, 29–36, and 37–41 weeks, and we also considered smaller intervals within them when possible. Sensitivity analysis also was performed with respect to congenital and gastrointestinal anomalies, as well as other predefined factors.
Prior to partitioning, data were visually inspected using scatter plots and smooth curves, as an initial guidance into outlier detection and partitioning. Formal outlier detection was performed using the technique discussed in the CLSI guidelines and described by Horn and colleagues.24 Outliers were removed from RI estimation as appropriate. We also examined the data within each partition to identify potential outlying data that could have an impact on RI estimates. Descriptive statistics also were used to summarize patient characteristics and other relevant variables collected as part of this study. Frequencies and percentages were used to summarize categorical variables, and continuous variables were summarized using mean and standard deviation (SD) or median and inter-quartile range (IQR). All analyses were performed using the R statistical software.25
Results
Study population
Data consisted of a total of 131 human fetuses and neonates, of whom 55% (n=72) were males and 45% (n=59) females. Gestational age ranged from 13 and 41 weeks, with a median of 24 weeks and IQR of 20–32 weeks (table 1). About 20% (n=26) of the fetuses had IUGR and 3.1% (n=4) were large for gestational age (LGA). Congenital anomalies were present on 26.7% (n=35) of the fetuses and neonates, and 13.0% (n=17) had gastrointestinal anomalies, such as Meckel’s diverticulum, bowel malrotation and diaphragmatic hernias. There were 10.7% (n=14) fetuses and neonates from multiple pregnancies (table 1).
Population characteristics and clinical measurements (n=131)
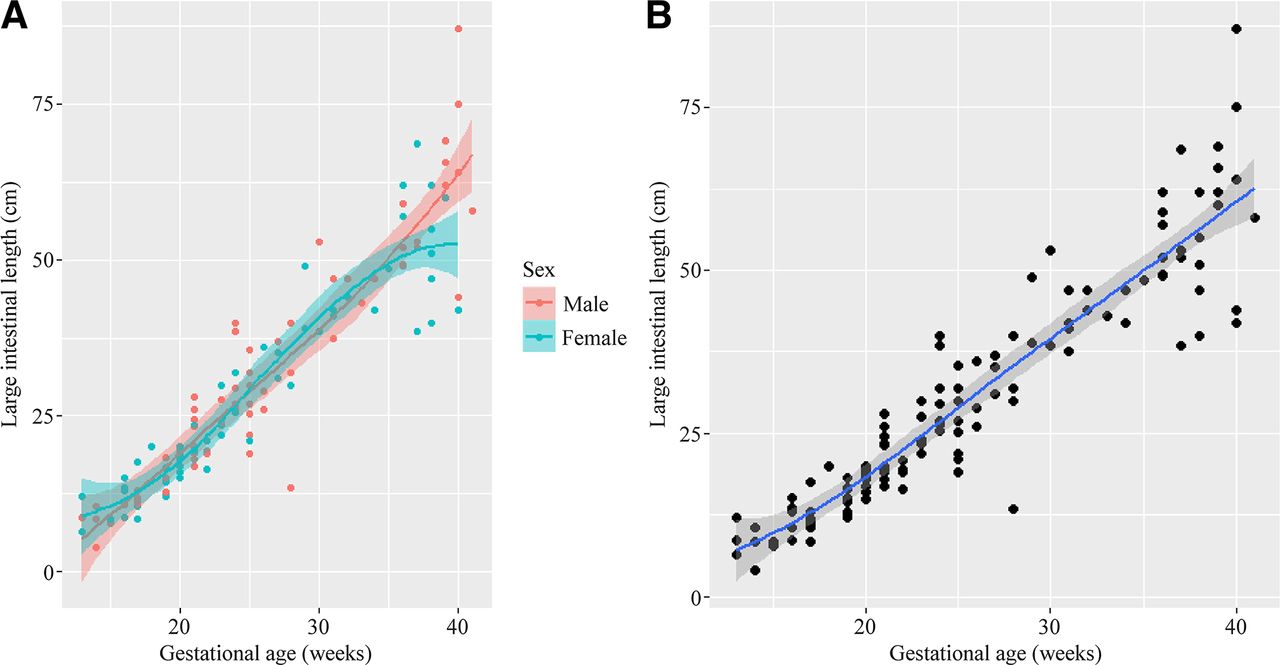
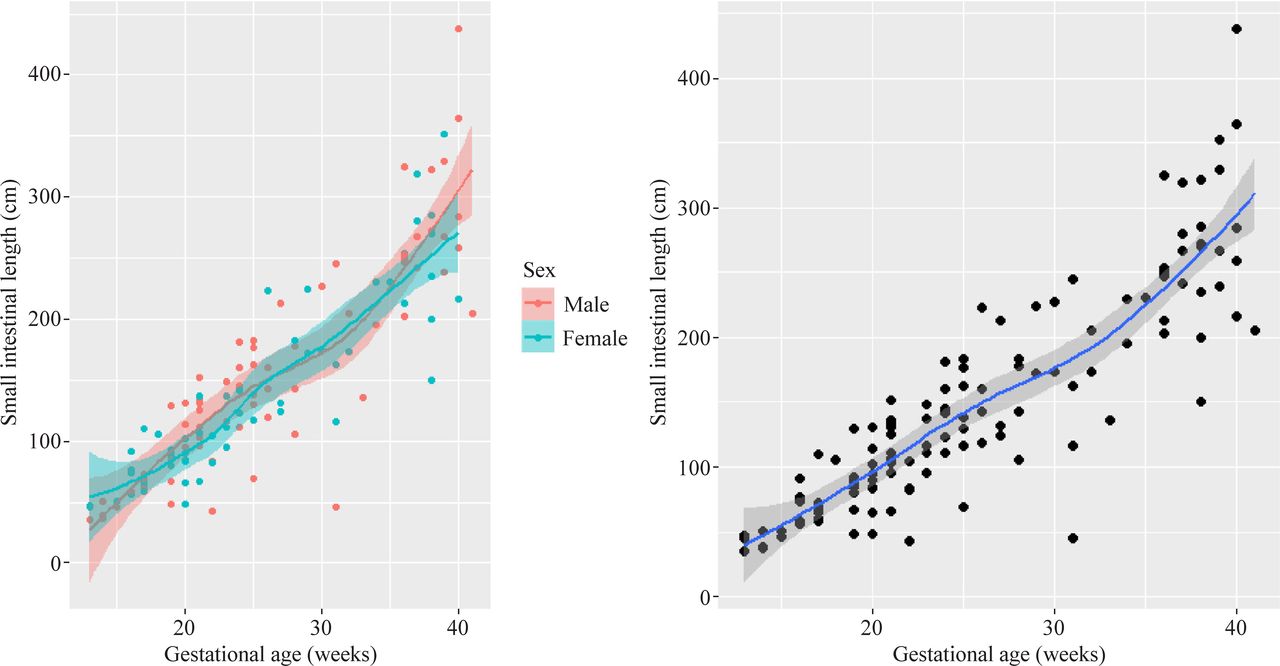
The average length of the small intestine was 147.7 cm (SD=82.7) in comparison to 30.6 cm (SD=17.7) for colon length. It is worth noting that both measurements are highly variable as shown by the value of their corresponding SDs. This is attributed to the wide range of gestational ages and to linear growth of intestinal length with respect to age (figures 1 and 2).

Plot of small intestinal length by gestational age for male and female (left) and for the combined population (right).
{kind=link}
{kind=link}
Plot of large intestinal length by gestational age (A) for male and female (B) combined data.
RIs for the small and large intestines
Our results show that both the small and large intestinal lengths increase linearly with respect to gestational age (figures 1 and 2). The figures also show that there is no difference between males and females; hence, we established the RIs based on the combined data, allowing use of the maximum possible sample size. Age-partitioned RIs with the corresponding 90% confidence intervals (CIs) are provided in table 2.
Age-specific reference intervals for fetal small and large intestinal lengths
The estimates also show that both the lower and upper limits of the RIs, for both small and large intestines, increase as gestational age increases, which is to be expected as a natural process of growth. The lower reference limits for small intestine ranged from 21.1 cm (for 13–20 weeks of gestational age) to 132.8 cm (for 37–41 weeks of gestational age). The upper reference limits ranged from 122.4 to 406.4 cm. For the large intestine, the lower reference limits ranged from 5.1 to 29.1 cm, while the upper reference limits ranged from 21.4 to 82.2 cm. Table 3 provides the ratio of the lower and upper limits for small versus large intestinal lengths.
Ratio of fetal small intestinal length to large intestinal length for lower and upper reference limits
Examining the ratio of the lower limits, apart from 21 to 24 and 29 to 36 gestational ages, the lower limit of the small intestine was four times larger than the lower limit of the large intestine. With respect to the upper limits, the small intestine was five times larger than the large intestine, except for gestational ages at 13–20 and 17–20 weeks, where it was nearly six times larger. Carefully examining the lower and upper reference limits for both the small and large intestines, we can see that there is considerable overlap in subsequent RIs, suggesting high level of heterogeneity within the partitions.
Sensitivity analysis
Table 4 provides the RIs and the corresponding 90% CIs for small intestine, where we analyzed only fetuses and neonates without congenital anomalies or gastrointestinal anomalies, not part of multiple pregnancy (ie, single pregnancy), not LGA (ie, below the 90th percentile), absence of IUGR and absence of maceration.
Reference intervals of small intestinal length by gestational age in subgroups of children (8-week partitions)
The results show that these RIs are similar to those with the full data, except for small changes that might be due to natural variation or other factors.
Discussion
We have established age-specific RIs for small and large intestinal lengths of fetuses and neonates using data in the Eastern Ontario and Western Québec regions. In comparison to our study, prior literature also demonstrates a positive, linear relationship between age and intestinal length RIs.1 2 This holds true for both the length of individual sections of the intestinal tract as well as the total intestinal length. In keeping with other studies, no differences in intestine length were found between sexes, and hence we combined data for males and females to maximize the sample size.4 22 23
Sensitivity analysis showed that the absence of congenital anomalies, gastrointestinal anomalies, maceration, as well as IUGR and LGA fetuses did not influence intestinal length RIs. Unique to our study were findings that fetuses from multiple pregnancies did not impact small intestinal length. The relationship between singleton pregnancies and the quantifiable impact on fetal intestinal length remains largely unanswered. Evidence suggests that fetuses from twin pregnancies are susceptible to a variety of intrauterine complications, such as IUGR, with the incidence of IUGR approximating 25%–35%.26 27 Whether IUGR impacts fetal intestinal length remains equivocal,3 4 and in our analysis IUGR did not have any impact on intestinal length. Similar to prior literature,4 maceration did not appear to have an impact on the growth of small intestinal lengths, and is in keeping with prior literature demonstrating that maceration does not alter all body measurements.15 The presence of congenital anomalies did not alter the small intestinal length. Though prior literature has demonstrated a reduction in length in Trisomy 21 fetuses,4 we included a range of congenital anomalies, such as Turner syndrome and vermian hypoplasia, in addition to Trisomy 21. Combining the congenital anomalies may have attenuated the veritable impact of Trisomy 21 on fetal intestinal growth. Unfortunately, due to sample size limitations, a subgroup analysis was not possible and represents an area of further research.
Capturing fetal intestinal length as early as 13−41 weeks is useful for both surgeons and pathologists to visualize intestinal length across a wide range of gestational ages. From a clinical standpoint, access to intestinal length RIs across a range of ages may assist in refining prognosis and treatment plans for preterm or term patients where intestinal resection is necessary, such as for Hirschsprung’s disease. Pathologists analyzing biopsies for transition zone between aganglionic and ganglionic cells can communicate residual bowel length to surgeons,28 which could assist surgeons in further planning postoperatively. Residual small bowel length may allow surgeons, for example, to predict the ability of an infant with short bowel syndrome (SBS) to wean from total parenteral nutrition following bowel resection.29 Furthermore, defining accurate small bowel length may provide benefit to pathologists conducting postmortem examinations. As mentioned earlier, there is currently a wide range of definitions being applied to SBS in fetuses and neonates, and establishing RIs may help apply this definition more precisely among this population based on age. Additionally, intervals may assist pathologists in identifying the pathological bowel length and in deciding when to screen for genetic anomalies, such as the CLMP gene in congenital SBS.11 13
Owing to limitations of sample size, determining reliable estimates for intestinal length is difficult. Wide variability in intestinal length observed within partitions in our data may indicate the need for a per-week analysis to capture minute differences over time because intestinal growth can vary widely in fetuses. Marnerides et al established fetal intestinal length intervals in the second trimester and found considerable differences across weekly partitions.4 To overcome these challenges, reference curves may be fitted to data and normal ranges can be obtained by using the functional form of the estimated curves at a given gestational age. We plan to pursue this approach in a subsequent study.
There are several limitations associated with this study. First, bowel measurements were made postmortem after removal of the bowel from the abdomen. Postmortem measurements can overestimate bowel length due to initial muscle contraction shortly after death, when relaxation and loss of tone occur as autolysis begins6; however, we did examine intestinal length in the sensitivity analysis without maceration to account for this. We did not find any impact of maceration on intestinal growth. In contrast, use of silk sutures to measure intestinal length in live infants provides a promising method to accurately measure intestinal length in vivo, although this methodology requires further external validation.19 We also followed a routine protocol as described in similar studies1 by laying out specimens on a moist plastic surface to minimize ‘stretch artifact’, and the same experienced perinatal pathologist measured each specimen twice to reduce error in measurement. Hence, the variations in gut length are not likely to be attributed to measurement inaccuracy. An additional limitation involves our population of study because the results are based on postmortem fetuses. Our results are thus not truly representative of the normal fetus population. However, the RIs could still be applicable to postmortem populations with similar characteristics.4 Further, to develop statistical models that account for the effects of age, sex, congenital anomalies, and other covariates, the Hoq et al’s method could have been used to estimate RIs as a function of age.30 The methods we used by Daly et al21 were valid but did not exploit the linear relationship between age and intestinal length. We also partitioned the age categories in a narrow manner because measurements increased linearly with respect to gestational age. However, this approach may be seen as subjective and contingent on the sample size available in each age category. We will use the discrete age groups commonly reported in the Hoq et al’s30 systematic review to address this limitation in a future study.
To conclude, this study has provided age-specific RIs for normal small and large intestinal lengths of fetuses and neonates. Pathologists can compare our data to other studies that have established reference standards for normal intestinal length. From a surgery perspective, understanding the expected or normal intestinal length might aid surgeons to communicate how much intestine is remaining in infants with parents and to plan postoperative management and prognosis accordingly. Following the standard protocols for conducting linear measurements of gastrointestinal contents,2 31 future studies are encouraged to replicate the study methodology at other health centers for cases in their catchment areas to enable comparisons across provincial institutions. More importantly, further research can be conducted to examine additional factors, such as gestational weight on intestinal length, using the Hoq et al’s30 method and to compare such results to established RIs. This will aid in better understanding of the differences in intestinal length between normal and pathological fetuses.
Lastly, coordination of multicenter, nationwide efforts to collect small and large intestinal length data (eg, similar to the Canadian Laboratory Initiative on Pediatric Reference Intervals)32 and to establish RIs in accordance with CLSI guidelines is needed.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study has obtained the Children’s Hospital of Eastern Ontario Research Ethics Board (CHEOREB 15/63X) approval.
References
Footnotes
Contributors CB contributed to investigation, validation and writing original draft. DED and AN contributed to guarantor, conceptualization, methodology, supervision, validation, writing, review and editing. IO contributed to writing, review and editing. MM contributed to data curation, administration and validation. AA, JSH, DR and NBcontributed to data analysis, validation, writing, review and editing. JdN contributed to data curation, project administration, resources, writing, review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.