Article Text

Abstract
Objective Infantile hypertrophic pyloric stenosis (IHPS), which causes gastric outlet obstruction and hypochloremic hypokalemic metabolic alkalosis, could pose a risk of postoperative apnea in patients. The aim of this study is to evaluate the incidence of postoperative apnea in babies admitted to a tertiary-level pediatric surgical center in Milano, Italy with diagnosis of IHPS in 2010–2019. The secondary objective is to evaluate the risk factors for postoperative apnea.
Methods This is a single-center, retrospective, observational cohort study. All patients admitted to our institution with diagnosis of IHPS during the study period were enrolled. Demographic and surgical variables, along with blood gas parameters, were obtained from the population. Postoperative apnea was defined as a respiratory pause longer than 15 s or a respiratory pause lasting less than 15 s, but associated with either bradycardia (heart rate <120 per minute), desaturation (SatO2 <90%), cyanosis, or hypotonia. Occurrence was obtained from nursing charts and was recorded as a no/yes dichotomous variable.
Results Of 122 patients, 12 (9.84%) experienced apnea and 110 (90.16%) did not. Using univariate analysis, we found that only postoperative hemoglobin was significantly different between the groups (p=0.03). No significant multivariable model was better than this univariate model for prediction of apnea.
Conclusions Postoperative anemia, possibly due to hemodilution, increased the risk of postoperative apnea. It could be hypothesized that anemia can be added as another apnea-contributing factor in a population at risk due to metabolic changes.
- Anesthetics
- Intensive Care, Neonatal
- Pediatrics
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Postoperative apnea is a recognized risk in young infants, particularly ex-preterm infants.
Infantile hypertrophic pyloric stenosis (IHPS) can cause metabolic alkalosis as a result of hydrogen loss from vomiting.
Babies with IHPS are theoretically more exposed to the risk of apnea since metabolic alkalosis can affect respiratory drive.
WHAT THIS STUDY ADDS
In a cohort of babies affected by IHPS, the incidence of postoperative apnea was 9.84%.
The pH of the apnea group did not differ from the non-apnea group.
Hemoglobin value (postoperative) was the only factor associated with postoperative apnea.
Low hemoglobin value acts as a contributing factor to apnea per se; the degree of hemoglobin modification preoperatively to postoperatively was not correlated with apnea.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Because both open and videolaparoscopic surgical corrections of IHPS yield minimal blood loss, a component of postoperative anemia could be attributed to intraoperative fluid administration.
Prospective trials are needed to better understand the hemoglobin cut-off values for apnea and the best fluid replacement therapies.
Introduction
Postoperative apnea is a recognized risk in young infants, particularly ex-preterm infants.1 2 Infantile hypertrophic pyloric stenosis (IHPS) is a rather common cause of gastric outlet obstruction in infants. Its definitive treatment is pyloromyotomy, which is often undertaken under general anesthesia. Theoretically these babies are particularly exposed to the risk of postoperative apnea since the hallmark of IHPS is projectile vomiting, which results in hypochloremic hypokalemic metabolic alkalosis, which could affect respiratory drive.3 The incidence of postoperative apnea as well as the risk factors in infants undergoing IHPS are still not clear.
The aim of this retrospective study is to evaluate the incidence of postoperative apnea in babies admitted to our hospital (a tertiary-level pediatric surgical center in Milano, Italy) with a diagnosis of IHPS and treated with pyloromyotomy in 2010–2019. The secondary aim is to evaluate the possible role of demographic and surgically related variables, along with blood gas parameters, in predicting the occurrence of postoperative apnea.
Methods
This single-center, retrospective, observational cohort study adheres to the standards of STrengthening the Reporting of OBservational studies in Epidemiology statement (STROBE).4
Patients and study design
We retrospectively reviewed the clinical charts of all patients admitted to our tertiary-level pediatric surgical center with a diagnosis of IHPS and treated with pyloromyotomy between January 1, 2010 and December 31, 2019. We considered only patients with a diagnosis of IHPS confirmed during surgery. Patients were excluded if pyloromyotomy was performed as part of a more complex surgical treatment.
Demographic data including gender, postconceptional age (PCA) at birth, birth weight, chronological age, and weight on admission were recorded, as well as medical history, intraoperative variables with regard to anesthetic and surgical duration, surgical technique (open vs laparoscopic), and intraoperative opioid administration. Standard intravenous hydration (4 mL/kg/hour balanced crystalloid) was applied to all patients. Only six experienced senior anesthesiologists were in charge of these procedures at all times. Patients were then monitored in the pediatric intensive care unit (PICU) according to institutional protocol.
Postoperative records were reviewed for total recovery time, duration of postoperative PICU monitoring, total hospital length of stay, and occurrence of adverse events.
We considered the blood gas analyses (BGA) obtained at three time points:
Admission BGA: obtained at the emergency department or on the ward in the first 6 hours from admission.
Preoperative BGA: obtained within 6 hours before surgery.
Postoperative BGA: obtained within 6 hours after surgery.
BGA has been obtained from venous and rarely from arterial samples and analyzed with non-portable BGA analyzers (Radiometer ABL90 FLEX Plus, Radiometer 800 Flex, Radiometer 700, Siemens Rapidpoint 500e), which have changed during the years. During a single period, the same blood gas analyzer was used in the hospital for all samples so that there is no risk of difference in the analysis of a single patient. BGA data included in our analysis were pH, Partial Pressure of Carbon Dioxide in blood (pCO2), Serum Bicarbonate (HCO3), Base Excess (BE), Serum Sodium (Na), Serum Potassium (K), Serum Chloride (Cl), Blood Hemoglobin (Hb), and serum lactate.
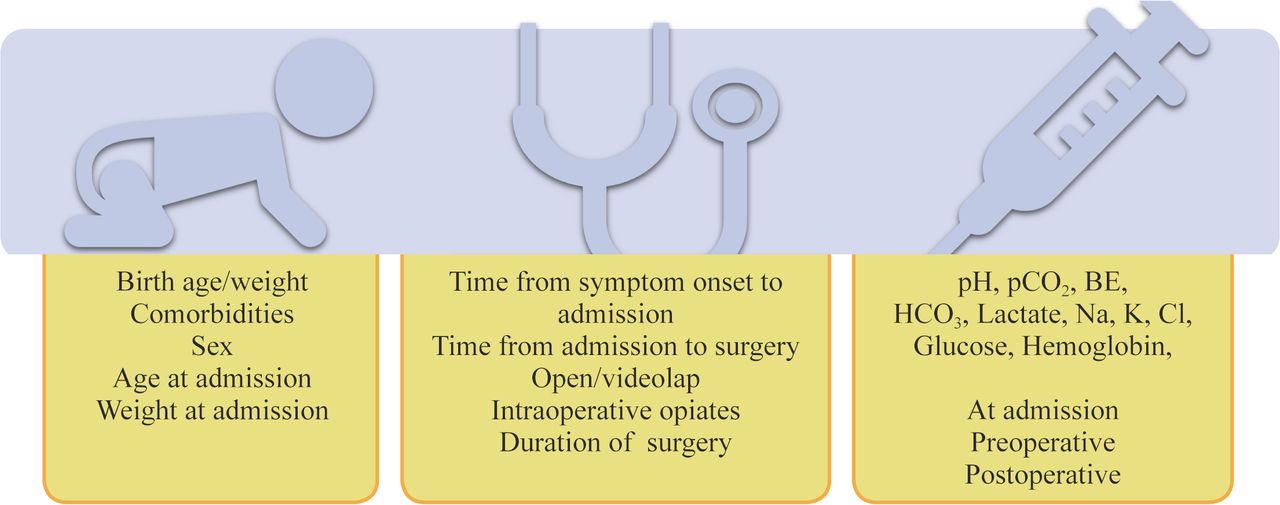
Postoperative apnea was defined as a respiratory pause lasting more than 15 s or a respiratory pause lasting less than 15 s, but with either bradycardia (heart rate <120 per minute), desaturation (peripheral oxygen saturation (SatO2) <90%), cyanosis, or hypotonia5 requiring tactile stimulation or positive pressure ventilation. Occurrence of apnea in the postoperative period (12 hours) was obtained from nursing charts and recorded as a no/yes dichotomous variable. Factors and parameters analyzed in this study are illustrated in figure 1. Patientswerethen discharged home when fullyrefed.
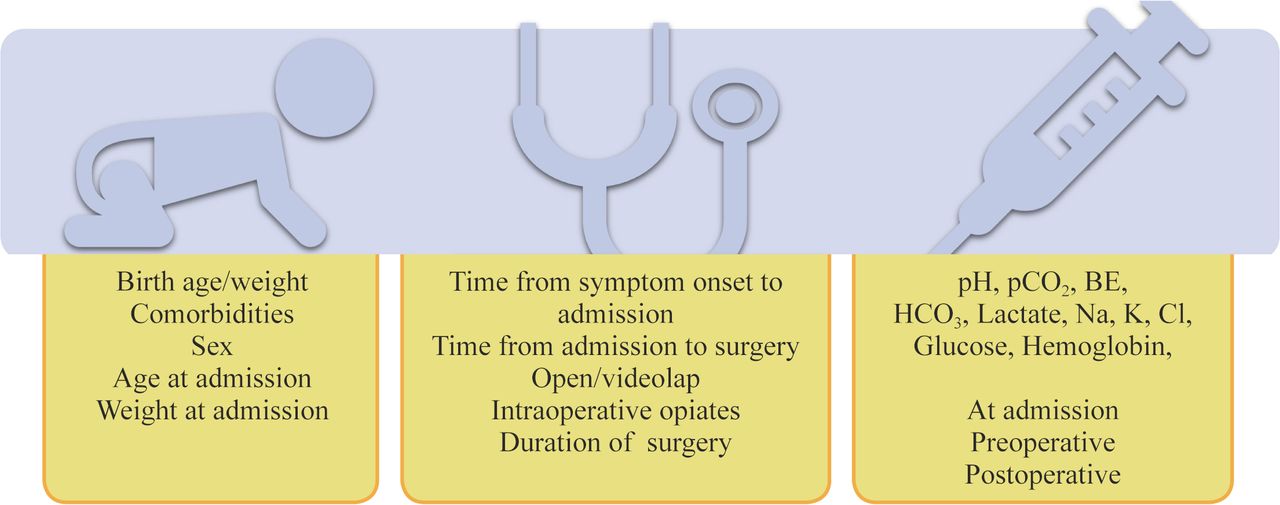
Parameters analyzed in the study. BE, base excess; Cl, serum chloride; Hb, blood hemoglobin; HCO3, serum bicarbonate; K, serum potassium; Na, serum sodium; pCO2, partial pressure of carbon dioxide in blood.
Statistical analysis
Continuous data are reported as mean±Standard (SD) [median, Interquartile range (IQR)]. Categorical data are reported as number (percentage). To build a multiple logistic regression model to evaluate possible predictive factors for the occurrence of apnea (as defined above), variable selection was performed with a univariable analysis (likelihood ratio test), using p<0.25 to select candidates for the multivariable model. All variables included were tested in the variable selection. Differences in hemoglobin between postoperative samples and admission and preoperative samples were also tested in the variable selection.
In building the final model, p<0.05 was considered statistically significant. The variables included in the final model were checked for multicollinearity by variance inflation factor (VIF) evaluation, and the linearity in the logit of continuous variables was assessed by visual inspection of the logit plot. Possible final models were evaluated comparing their respective Akaike information criterion and Bayesian information criterion.
Data were analyzed with R V.4.0.4 software (February 15, 2021), ‘Lost Library Book’ [The R Foundation for Statistical Computing Platform: R Core Team (2021), R: A language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/]. Regression analysis was performed with base R, except for graph and data management for which the ‘tidyverse’ package6 was employed and for VIF evaluation for which the ‘car’ package7 was used.
Results
During the 10-year study period (from January 1, 2010 to December 31, 2019), 123 patients were admitted to our hospital with a diagnosis of IHPS. One patient (0.81%) was excluded from the study due to pyloromyotomy being part of the surgical treatment of a complex intestinal malformation. Of the remaining 122 patients, 12 (9.84%) experienced apnea in the postoperative period (apnea group) and 110 (90.16%) did not (no apnea group). No patient experienced serious adverse events related to apnea, which always resolved with simple tactile stimulation. A clinically significant preoperative dehydration was not apparent in any of our patients.
Demographic data of the study cohort were comparable between patients with apnea and without apnea (table 1). In addition, there are no difference of times elapsed between onset of symptoms and hospital admission and surgery characteristics (table 2). Data on serum electrolytes are presented in online supplemental file 1.
Supplemental material
Demographic characteristics of the population in object (all patients, patients affected by postoperative apnea, and patients not affected by postoperative apnea)
Surgery-related data in the two populations
In the univariate analysis, eight variables with p<0.25 were considered in building a multivariable model. No significant multivariable model was better than postoperative hemoglobin alone, which was significantly different between the groups: 9.23±1.66 g/dL (9.00, 8.45–9.60 g/dL) in the apnea group and 11.98±2.88 g/dL (11.70, 9.67–14.00 g/dL) in the no apnea group (p=0.03) (table 3). It should be noted that postoperative hemoglobin variations with respect to admission or preoperative values were not predictive of apnea.
Blood gas, glucose, lactate, and hemoglobin values in the preoperative and postoperative periods in the two populations
Discussion
Our series exhibits a rather high incidence of postoperative apnea after pyloromyotomy (9.84%), consistent with the results of a recent review on IHPS which found postoperative apnea rates between 0.2% and 16%.8 This wide range is possibly explained by lack of robust studies.
The problem of postoperative apnea in newborns has been recognized long ago when rates as high as 49% have been reported, mainly in the preterm population; the incidence of apnea and bradycardia after anesthesia in term infants has not been described extensively but appears to be less than that of preterm infants,2 9–11 ranging from 0% to 10%.10 12 Indeed, the ventilatory response to carbon dioxide (CO2) increases with advancing postnatal and gestational age, so that the ex-premature population is at higher risk of postoperative apnea than the term population.13 Postoperative apnea rates similar to the one in our cohort have been reported after general anesthesia in preterm babies operated before 60 weeks of PCA.10 14 15
Anesthesia acts as a triggering event for apnea because anesthetic agents, either inhalational or intravenous, produce a dose-dependent depression of ventilatory control. Opioids, which also produce a dose-dependent respiratory depression with decreased responsiveness to CO2 and a right shift of the CO2–response curve, interfere with the periodicity of breathing and may cause respiratory pauses, periodic breathing, and apnea.14 In our series, patients with postoperative apnea neither exhibited longer exposure to anesthetic agents nor received more opioid drugs. Also, patients who did not receive any intravenous opiate did not show any significant reduction in apnea occurrence. Careful titration of anesthesia by experienced anesthesiologists could account for these results.
Actually, IHPS itself is believed to contribute to the risk of apnea, either preoperatively or postoperatively.16–18 In IHPS apnea is possibly caused by ventilatory drive inhibition by the ongoing alkalotic state.18–21 Control of ventilation is primarily dependent on the partial pressure of carbon dioxide (PaCO2) and secondarily on the partial pressure of oxygen in the blood (PaO2). PaCO2 impacts minute ventilation by altering the hydrogen ion concentration or pH in the cerebrospinal fluid (CSF), while the impact of PaO2 results from a peripheral effect on chemoreceptors in the aorta and carotid artery. Increased PaCO2 rapidly diffuses into the CSF, thereby immediately decreasing the pH and leading to ventilatory stimulation. Generally, a decrease in the partial pressure of arterial oxygen (PaO2) also stimulates minute ventilation. However, neonates and infants manifest a paradoxical reaction to low PaO2, resulting in depressed central control of ventilation. This response continues for about 3 weeks in term newborns, but the mean admission age of our population was beyond this period.22 Within the neonatal and infant population, PaCO2 therefore represents the primary stimulus for ventilation, which is altered in non-acute metabolic alkalotic states, when minute ventilation is suppressed to increase PaCO2 to compensate for the increased pH.23
Our apnea and no apnea groups did not differ in BGA pH at any time point and pH was not alkalotic. A possible explanation for this is that the hydrogen ion loss was accompanied by a tendency for acidemia due to dehydration. Besides, medical therapy was started precociously in our series given the early diagnosis of IHPS.23
Postoperative anemia increases the risk of apnea in our series. Current literature reports conflicting results on the effect of anemia on breathing. Cotè et al,24 in their combined analysis of available studies on the effects of anesthesia on postoperative apnea in preterm babies, suggest that anemia is a significant risk factor and packed red blood cell transfusion significantly improves cardiorespiratory variables in preterm infants with anemia.25 Other studies do not show significant changes in the frequency, severity, and/or duration of apnea, bradycardia, or desaturation following transfusion in preterm infants, and more recently anemia was not identified as an independent risk factor for postoperative apnea in term babies.10 26
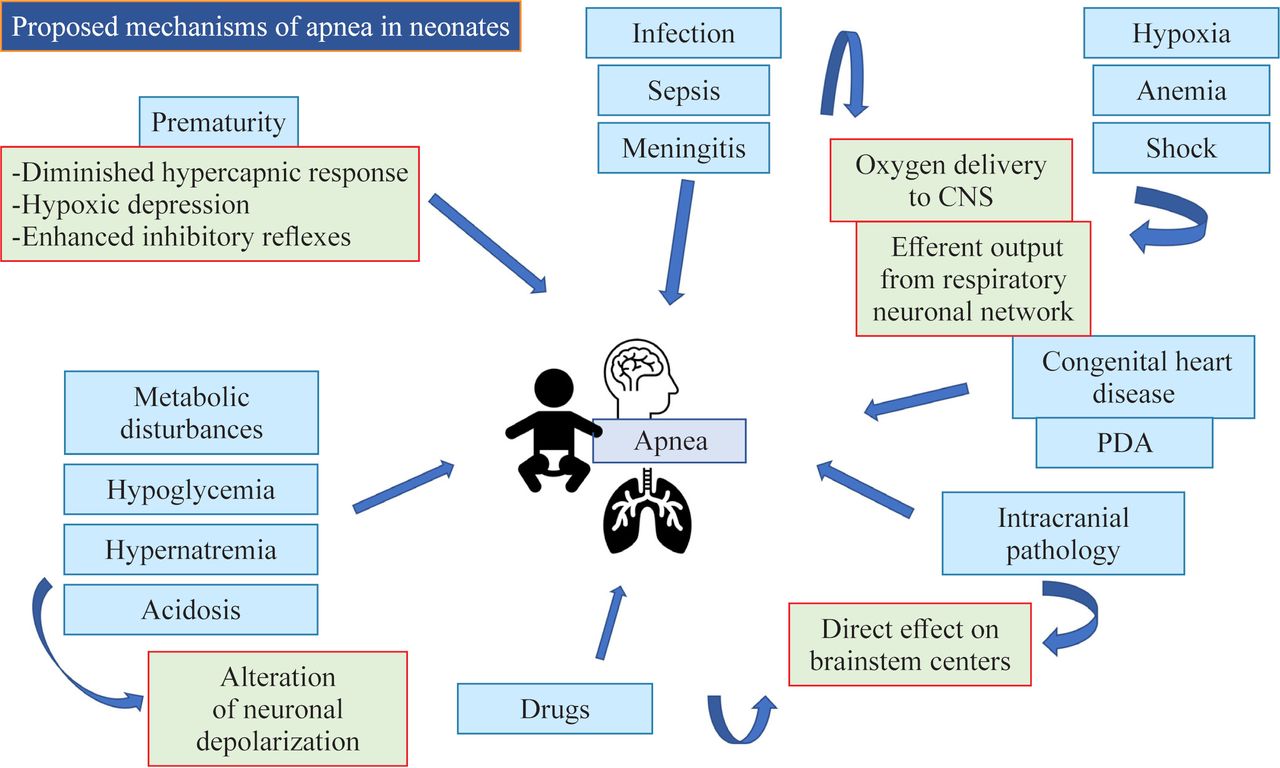
Postoperative hemoglobin level was the only factor associated with apnea in our cohort. Although hemoglobin levels in the apnea group were not extremely low (9.23±1.66 (9.00, 8.45–9.60) mg/dL), and although surgery-related Hb reduction was more prominent in patients with apnea, neither the difference between postoperative and admission hemoglobin nor the difference between postoperative and preoperative hemoglobin was a significant predictor of postoperative apnea. This suggests that a lower hemoglobin absolute value is an apnea-contributing factor per se, whereas changes in hemoglobin do not play a role in this setting. Anemia, by decreasing oxygen-carrying capacity, may result in decreased oxygen delivery to the central nervous system, causing decreased efferent output of the respiratory neuronal network. This and the other potential mechanisms underlying apnea in neonates are presented in figure 2.

{kind=link}
{kind=link}
Potential mechanisms of apnea in newborns. CNS, central nervous system; PDA, patent ductus arteriosus.
Minimal blood losses were recorded in both laparoscopic pyloromyotomy (the majority of our patients) and in open surgery. Hence, postoperative low hemoglobin values could sometimes be attributable to some degree of hemodilution associated with intraoperative crystalloid administration. Unfortunately we cannot quantify the relative contribution of hemorrhage and hemodilution in our cases, which is a limitation of our study.
Another limitation of our study is its single-center and retrospective design. Moreover we could not differentiate ‘central’ apnea (due to respiratory drive depression) and ‘peripheral’ apnea (due to airway obstruction) from the available clinical charts. On the other hand, the standardization of apnea registration at our center according to a precise, clinically sound definition limits the effect of such biases.
A further limitation is the relatively small sample size. In dealing with logistic regression models, the number of events per variable (EPV) is a critical issue. In the medical literature, an EPV of 10 is widely used as the lower limit for developing prediction models that predict a binary outcome, although this value has been variably criticized.27 Because we reported only 12 cases of apnea and the result of our secondary endpoint evaluation (possible predictive variables for apnea) is based only on a single univariate likelihood ratio test, caution should be exerted in interpreting this result. The relationship we observed between postoperative apnea and hemoglobin level should not be interpreted as a causal relationship, but rather as a possible association. Moreover, the low EPV could have hampered our capability to infer other possible potential predictors owing to lack of sufficient power. However, to our knowledge, no other study has investigated the possible risk factors for postoperative apnea in patients affected by IHPS.
In conclusion, in our series the incidence of postoperative apnea was 9.84% among infants undergoing pyloromyotomy. We found the association between lower postoperative hemoglobin and apnea. Prospective studies are needed to better define the risk factors associated with postoperative apnea in these patients.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This single-center, retrospective, observational cohort study was approved by our local institutional review board (2021/ST/204).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LaCampo4
Contributors AC: conceptualization, methodology, supervision, writing - original draft, writing - review and editing. VD: conceptualization. EZ, SR, FT, LMGE, VC, GP: investigation, data curation. MG: supervision, formal analysis, writing - original draft, writing - review and editing. AC is the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.