Article Text

Abstract
Objective Circumcision is often performed in neonates and is associated with significant pain. This study was conducted to compare the anesthetic efficacy of two methods of local anaesthesia for neonatal circumcision: topical eutectic mixture of local anesthetics (EMLA) cream and dorsal penile nerve block (DPNB) with lidocaine.
Methods Male neonates who presented for circumcision and met the eligibility criteria were recruited for the study and were randomly assigned to one of the two methods of anesthesia before the procedure. Anesthetic efficacy was compared by pain assessment during four standardized steps of the procedure (clamping, crushing, tying, and cutting of the foreskin, respectively) using the modified Neonatal Infant Pain Scale (NIPS), changes in transcutaneous oxygen saturation (SpO2), heart rate (HR), and preoperative and postoperative salivary cortisol levels. Patients also were evaluated after 24 hours to assess for complications.
Results Totally, 138 babies were recruited. Significantly higher NIPS scores were observed among babies who had EMLA cream during tying (p=0.019) and cutting (p=0.043). The rise in mean HR from baseline was statistically significant throughout the procedure in the EMLA group. In the DPNB group, there was no significant rise in mean HR during crushing (p=0.919) and cutting (p=0.197). There was a significant decrease in mean SpO2 from baseline in both groups. Salivary cortisol showed significant increase in mean levels in both groups. No significant untoward effects were observed.
Conclusion DPNB with lidocaine has a better pain control compared with EMLA cream during neonatal circumcision. Both methods are safe in neonates.
- Pediatrics
- Anesthetics
- Analgesia
- Child Health
- Neonatology
Data availability statement
Data are available on reasonable request. Individual participant data that underlie the results reported in this article after deidentification (text, table, figures, and appendices).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Circumcision is a painful experience for neonates.
There are several methods of pain control during the procedure.
Dorsal penile nerve block (DPNB) with lidocaine and eutectic mixture of local anesthetics (EMLA) cream are effective.
What this study adds
DPNB and EMLA cream are comparably safe and effective for neonatal circumcision.
How this study might affect research, practice or policy
Improvement in the approach to pain control during neonatal circumcision with increased use of topical agents, thus reducing the need for invasive techniques.
Introduction
Circumcision, the surgical removal of the prepuce, is one of the oldest and most frequently performed surgical procedures.1 2 It is performed for different reasons, such as sociocultural, religious, and medical reasons.3 4 When it is performed for sociocultural and religious reasons, it is done often on healthy neonates. However, in certain societies where applicable, medical and nursing staff may engage in public health campaigns to advise against routine circumcision of their newborns.
More importantly however, little attention is often paid to the pain experienced by these infants during the procedure. The use and choice of anesthesia remains an issue of debate and research.5 In our experience, in most clinical settings where routine neonatal circumcision is done, anesthesia is often not provided. The assumed absence of pain perception in the neonates, unfamiliarity with the use and side effects of analgesics and anesthetics in neonates, and the belief that the pain from the injection of anesthetics is as bad as the pain of the procedure itself are some of the reasons attributed to this practice.6 7
The neural pathways related to painful stimuli, including the cortical and subcortical centers at which level pain is perceived are now known to be functional at birth.8 9 Neonatal circumcision produces physiological changes, behavioral changes and adrenal cortical response that have been attributed to the pain response.10–12 These form the basis of pain assessment. Several scoring systems validated for measuring pain in neonates have been developed based on these indicators. Most studies comparing the efficacy of local anesthetic agents for circumcision in neonates use the Neonatal Infant Pain Scale (NIPS) composed of six indicators of pain (facial expression, cry, breathing patterns, arms, legs, and state of arousal.11 13 14 Cortisol is particularly an important biochemical marker for stress in neonates because its salivary level can be used. In addition, its level begins to rise within 5 min after exposure to a stressor and therefore can be used for evaluation of acute pain in term and preterm neonates.15–17
Several methods to provide analgesia for circumcision include the use of sucrose pacifiers, immediate postoperative administration of systemic opioids or acetaminophen, dorsal penile nerve block (DPNB) with 1% or 2% lidocaine and topical local anesthetics, such as eutectic mixture of local anesthetics (EMLA)—an eutectic mixture of 2.5% lidocaine and 2.5% prilocaine hydrochloride.18 19
Local anesthetic infiltration for procedures in neonates still poses a challenge.20 With the advent of topical agents that have been reported to be equally effective with less morbidity,8 this study comparing DPNB with lidocaine and EMLA cream during circumcision was intended to determine the best option for neonates in our setting.
The outcome measures for the anesthetic efficacy of these methods were the NIPS scores, heart rate (HR), and oxygen saturation (SpO2) changes during the procedure, as well as the preoperative and postoperative salivary cortisol changes. Our null hypothesis was that there was no statistically significant difference in anesthetic efficacy between DPNB with lidocaine and EMLA cream during neonatal circumcision.
Methods
Study population
This prospective comparative study was done in the Paediatric Surgery Unit of the University of Benin Teaching Hospital, Benin City, Nigeria, from April 2017 to September 2017.
The sample size was based on one of the outcome variables—the average NIPS scores. From previous studies, the assumption made was that infants receiving a somewhat effective anesthetic would score between 3 and 4, and infants receiving very effective anesthetic would score between 0 and 2. Using a significance level of 5% and 90% power, our sample size was calculated to be 138. To be included in the study, the patients met the following inclusion criteria: they were healthy term neonates or preterm with corrected gestational age ≥37 weeks, they had no penile or preputial anomalies, and the parents/guardians gave consent. Neonates circumcised with methods other than Plastibell and those who had evidence of dermatitis, abrasions, or other skin conditions involving the groin/genital area were excluded.
Study protocol
All neonates who presented electively for circumcision were reviewed in the preceding clinic days. Patients who met the eligibility criteria were then recruited consecutively for the study (figure 1). Mothers were advised to breast feed the babies up to 2 hours before the procedure. Recruited neonates were assigned to one of two groups to be circumcised using either EMLA or DPNB with lidocaine as a local anesthetic. This was done by simple randomization using the Program for Epidemiologists V.11.65 for Windows (WinPEPI).21 EMLA cream (AstraZeneca) with a concentration of 5% and lidocaine ampoules (Rotex Medica, Germany) were used throughout the duration of the study. K-Y jelly (UK Johnson and Johnson) was used as a placebo cream for the DPNB group.

CONSORT (Consolidated Standards of Reporting Trials) flow diagram of study population. DPNB, dorsal penile nerve block.
On the day of circumcision, sociodemographic details were obtained and the patients were weighed by the team nurse. While in the mother’s arms, each patient’s baseline HR and SpO2 were recorded. The baseline NIPS score also was assessed.
Neonates randomized to receive EMLA cream had 1 g applied 1 hour before the circumcision. The cream was directly applied over the distal half of the penis and prepuce and was covered with an occlusive dressing supplied with the cream by the manufacturer that prevents dissolution of the cream in the event of voiding before the procedure.22 Neonates randomized to have DPNB with lidocaine had K-Y Jelly applied as placebo, covered with the same occlusive dressing 1 hour before the procedure to blind the pain assessor. Thus, every neonate had cream and dressing applied to the penis 1 hour before the circumcision. Both EMLA and K-Y Jelly looked similar on removal of dressing. This was done at the theatre reception area, while in their mothers’ arms.
Following this, saliva was obtained from the neonates for cortisol estimation using a light plastic pipette. The pipette was given to the mothers to place on the inside of the cheeks for about 10–20 min during the 1 hour waiting period until about 0.5–1 mL of saliva was obtained. Saliva obtained was immediately refrigerated before transport to the chemical pathologist. Cortisol estimation for the entire study was done by the same chemical pathologist using the same ELISA kit to ensure standardization.
After 1 hour following application of the EMLA or K-Y Jelly, DPNB with 1 mL of 1% lidocaine (prelabeled syringe B) was done for neonates with K-Y Jelly cream and 1 mL of normal saline (prelabeled syringe A) for neonates with EMLA cream dressing by the researcher. This was done in the anesthetic room before transfer of the neonate to the operating room for the circumcision.
The neonates were swaddled with warm clothes from waist to shoulder and restrained by an assistant and a pulse oximeter probe was placed on the patient’s foot, while an assistant spread the lower limbs apart for the surgeon. All neonates were circumcised using the Plastibell method. The procedure was started 3 min after the DPNB and was divided into four standard steps for the purpose of comparison: application of artery forceps and separation of adhesions between prepuce and glans penis (clamping), crushing of the prepuce with hemostat/dorsal preputial incision (crushing), insertion of the Plastibell and tightening of encircling ligature (tying), and excision of prepuce (cutting).
Pain assessment
During the procedure, pain was assessed and scored by a team member who had remained in the operating room during the administration of creams and DPNB, thus was blinded to the groups. The NIPS was used in this study to assess pain scores. This scale is composed of six indicators of pain (facial expression, cry, breathing patterns, arms, legs, and state of arousal), five behavioral and one physiological. Each indicator scored 0–1 except cry which is scored 0–2. A score of <3 indicates no pain; 3–4, mild to moderate pain; and >4, severe pain.23
In this study however, the NIPS was modified in that five of the six components were used: facial expression, crying, breathing patterns, leg movements, and state of arousal (table 1). Arm movements were omitted because the infant’s arm was wrapped within the swaddle cloth. This was done in a similar study by Butler-O'Hara where leg movements were omitted as the infant’s legs were strapped to the circumcision board during the procedure.11 Thus, the modified NIPS score, SpO2, and HR were assessed and recorded during each standard step of the procedure. The duration of surgery also was recorded.
Modified Neonatal Infant Pain Scale
At the conclusion of the procedure, each infant was taken to the recovery room and was kept under observation for 1 hour. A second saliva sample was obtained for postoperative cortisol estimation 20 min after the procedure. On discharge, all babies had paracetamol prescribed for them. Babies were evaluated after 24 hours, and complications, if any, were recorded. Babies who had complications were given further appointments for review.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) V.20.0 software. χ2 tests of association were used to test for statistical association between study groups and presence of complications post-circumcision. An independent sample t-test was used to compare means of physiological parameters and NIPS scores in infants in EMLA and DPNB groups. A paired sample t-test was used to compare the baseline means of physiological parameters and NIPS scores against means of physiological parameters and NIPS scores at each step of the procedure. A p-value of <0.05 was considered as significant.
Results
A total of 138 neonates were recruited for this study. All patients were available for the 24-hour postoperative evaluation and therefore concluded the study. Sample characteristics of both groups were similar (table 2).
Sociodemographic characteristics of study population
Mean changes from baseline in NIPS scores were observed during the steps of the procedure (figure 2). Overall, although the mean score during the entire procedure was not significantly less in the DPNB group (2.971) compared with the EMLA group (3.552), the mean NIPS score in the DPNB group reflected no experience of pain (<3) whereas in the EMLA group, it was that of mild to moderate pain (3–4) based on the NIPS categorization.
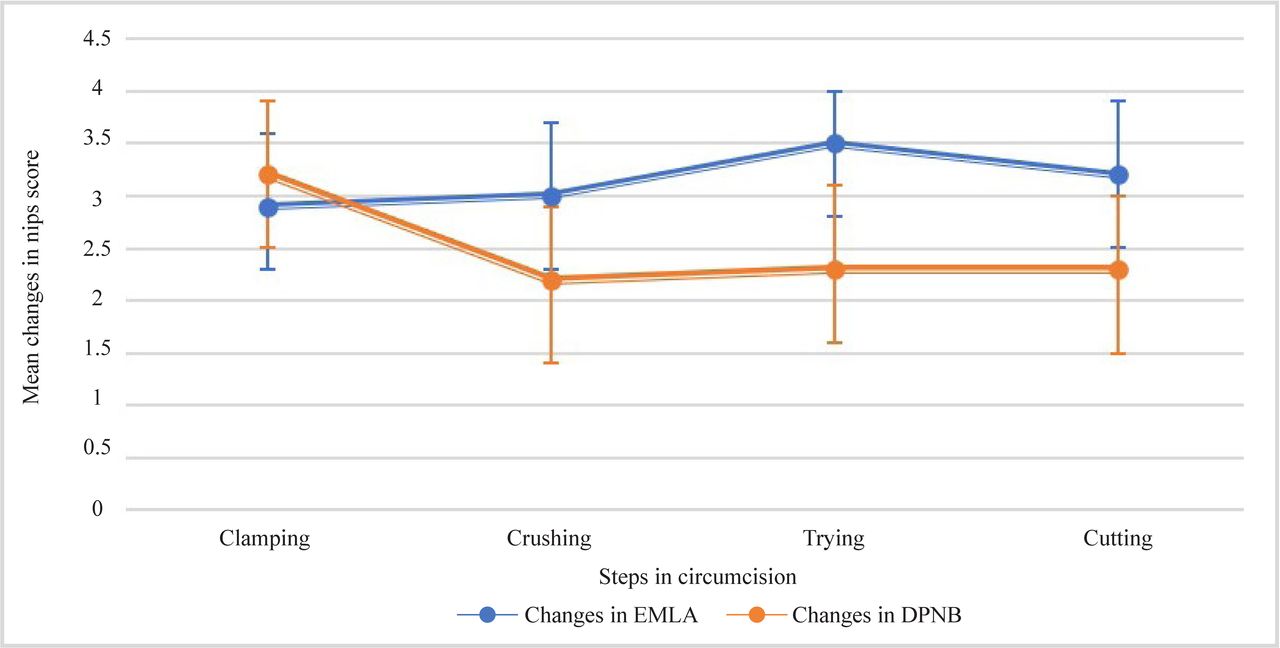
Mean changes from baseline NIPS score as well as the 95% CIs (represented by the error bars above and below each mean value) in both groups during each step of the procedure. Except during clamping, consistently less changes from baseline score were observed in the DPNB group. CI, confidence interval; DPNB, dorsal penile nerve block; EMLA, eutectic mixture of local anesthetics; NIPS, Neonatal Infant Pain Scale.
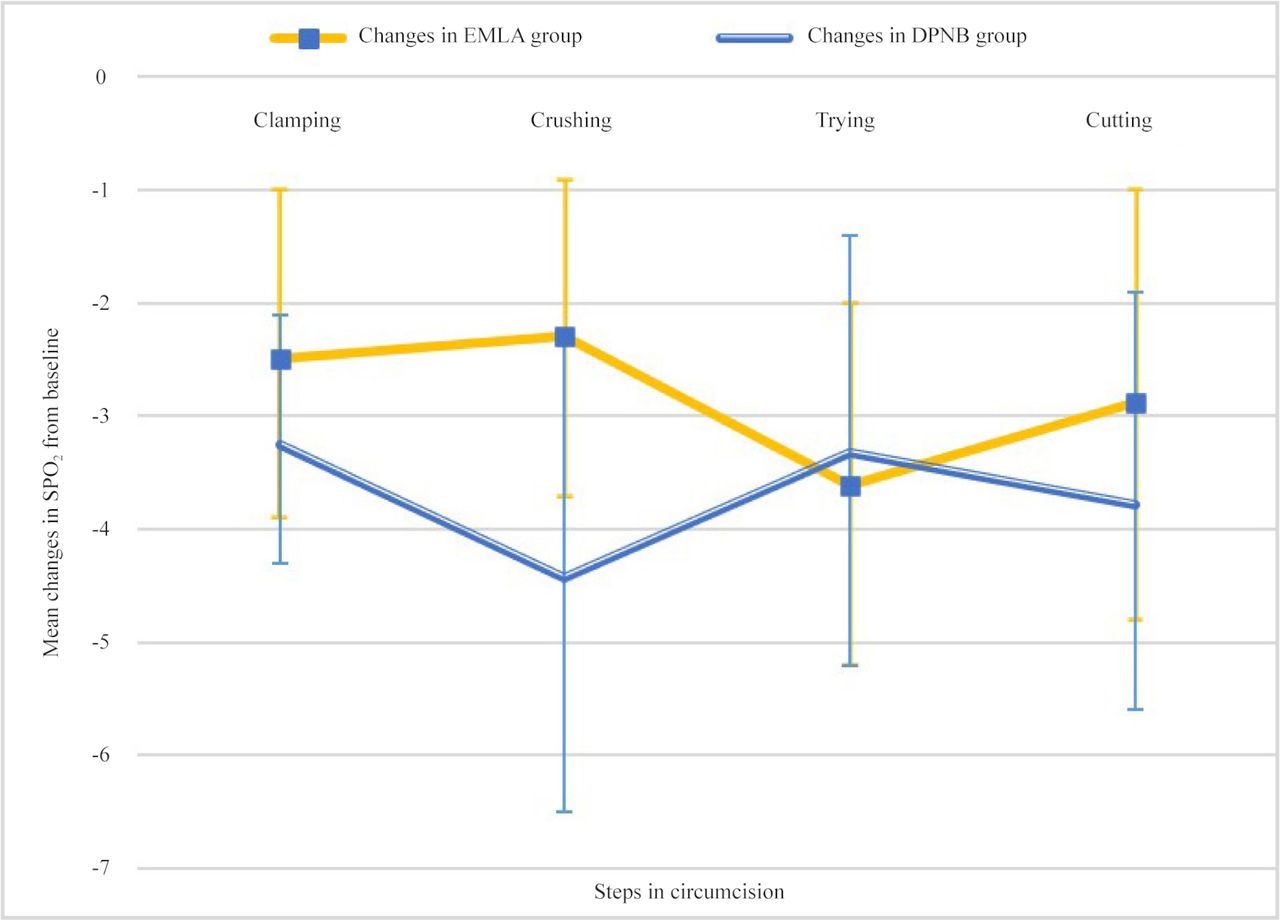
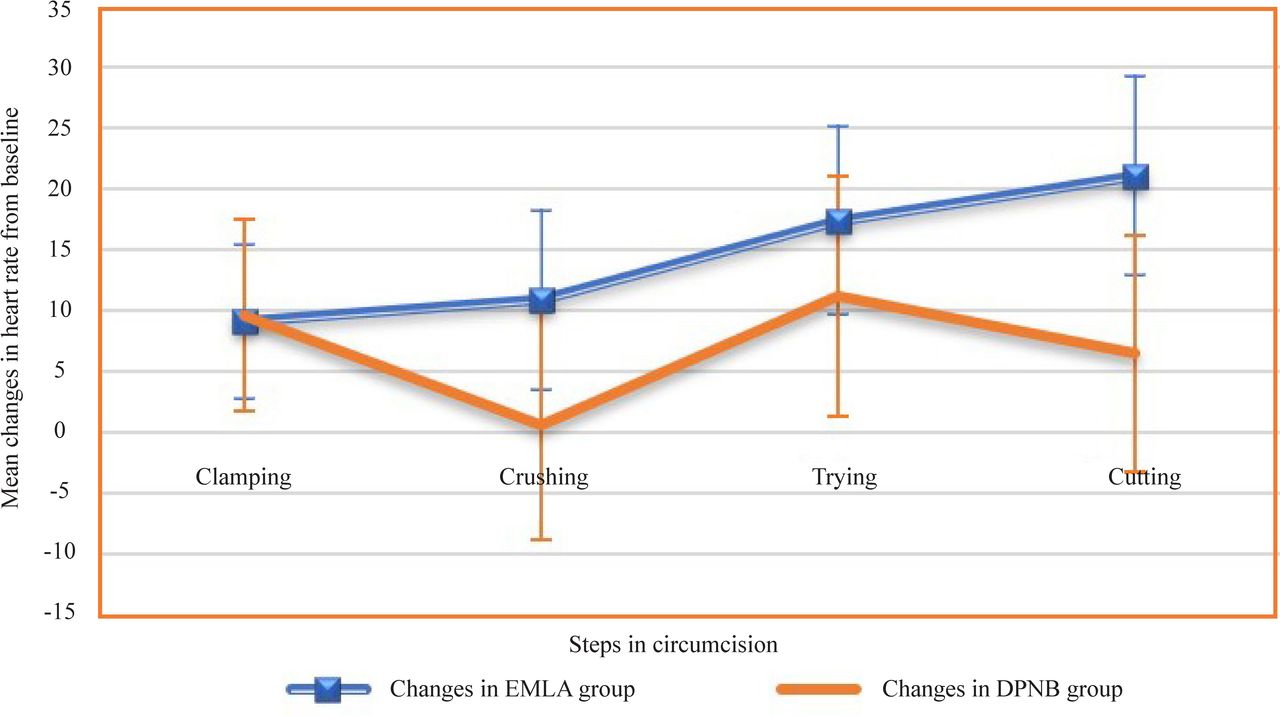
For the EMLA group, there was a statistically significant increase in mean HR in all the steps of the procedure compared with the baseline values. In the DPNB group, significant increase in mean HR was only observed at clamping (9.594 beats per minute (bpm); p=0.022) and tying (6.434 bpm; p=0.029) (figure 3). With respect to SpO2 changes, in both groups, there was statistically significant difference in mean SpO2 between baseline values and all the steps of the procedure (figure 4).
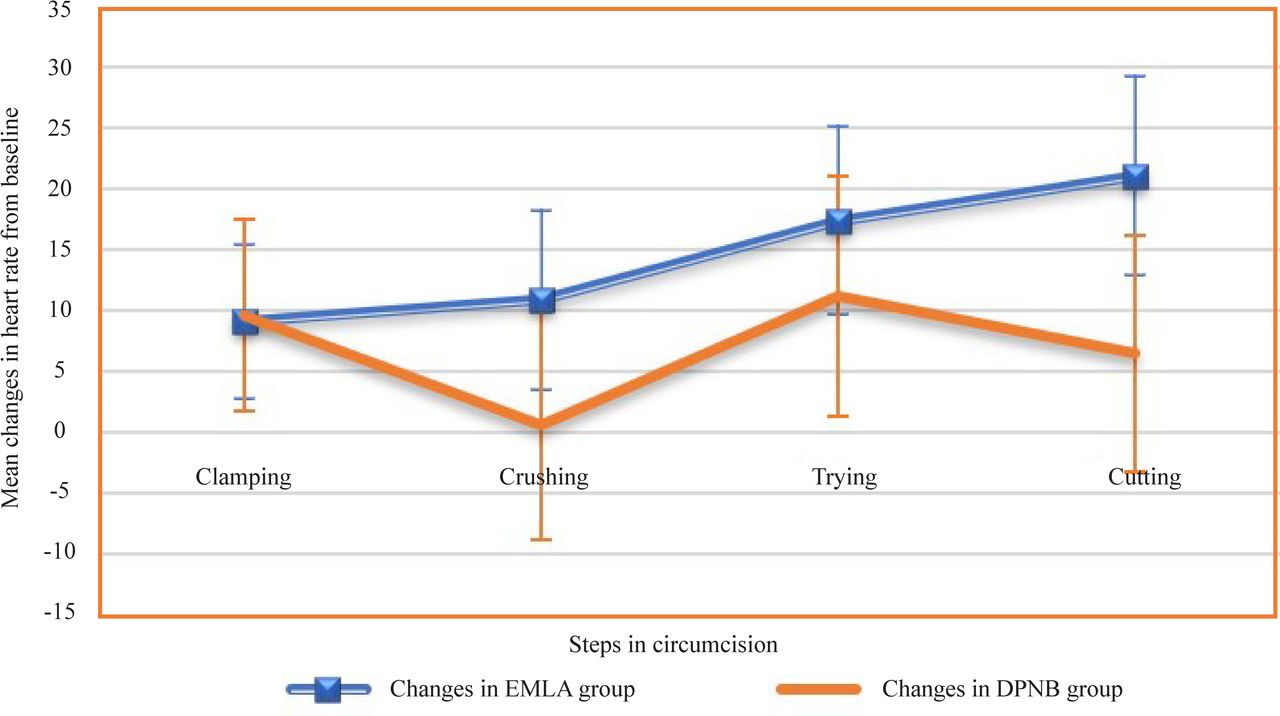
Figure shows the mean changes in heart rate from baseline as well as the 95% CI (represented by the error bars above and below each mean value) in the EMLA and DPNB groups during each step of the procedure. CI, confidence interval; DPNB, dorsal penile nerve block; EMLA, eutectic mixture of local anesthetics.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pattern of mean changes from baseline in oxygen saturation (SpO2) in both groups during each step of the procedure (95% CIs are represented by error bars). Both groups showed significant changes throughout the procedure. CI, confidence interval; DPNB, dorsal penile nerve block; EMLA, eutectic mixture of local anesthetics.
There was an increase in the mean levels of cortisol in both EMLA and DPNB groups. The mean postcircumcision salivary cortisol in the EMLA group was 6.933 ng/mL±6.208 ng/mL with a mean difference of 4.958, which was statistically significant (p<0.0001). Similarly, in the DPNB group, the mean postcircumcision cortisol was 6.294±5.849 ng/mL with a mean difference of 4.543, which was also statistically significant (p<0.0001). Comparing the mean cortisol level after the procedure between both groups however, there was no statistically significant difference (p=0.535).
A few complications were observed in this study (table 3). One patient (1.4%) in the EMLA group had penile erythema. Only 2.9% of infants in the EMLA group had penile edema as a complication compared with 5.8% in the DPNB group. Overall, there was no statistically significant difference in complication rate between neonates in either EMLA or DPNB group.
Observed complications
Discussion
Circumcision is a surgical procedure often performed in neonates. Mitigation of pain associated with this procedure has remained a subject of debate and controversy. Nevertheless, good pain control during circumcision contributes significantly to the overall safety of the procedure.1 8 24
The revised American Academy of Paediatrics 2012 policy statement highlights that elective circumcision of male newborns is well tolerated when performed by trained professionals with appropriate pain management and has considerably lower complication rates than when performed later in life.25 Many techniques have been described for attenuating the pain associated with neonatal circumcision. DPNB with lidocaine and EMLA cream application evaluated in this study have been shown to be safe and effective during the procedure.11 24 Use of oral sucrose, which is cheap, also has been shown to be effective and is sometimes added to any of the above methods. This addition was not used in this study.
Pain assessment in neonates is also challenging. A combination of behavioral, physiological, and biochemical parameters that are altered during the procedure are used for objective assessment.11 12 17 26 27
One hundred and thirty-eight patients recruited for this study had similar demographic characteristics. The majority of the patients in both groups were aged between 8 and 14 days, which is the preferred age of presentation of newborns for circumcision in Nigeria for religious and sociocultural reasons, as highlighted in the study by Ekwunife et al.28
The average NIPS score was >3 in the EMLA group indicating mild/moderate pain experienced by those neonates, whereas the DPNB group had an average score of <3 which indicates no pain based on the NIPS categorization.29 This finding was similar to that of Butler-O’Hara et al11 who observed an average NIPS score of 4.8 in the EMLA group and 2.3 in the DPNB group. Howard et al30 also compared EMLA and DPNB for neonatal circumcision using the Brazelton distress score and noted significantly higher scores among patients who had EMLA cream.
During the procedure, there were variations in the NIPS score with respect to the four designated steps of clamping, crushing, tying, and cutting of the prepuce. Significantly higher distress was noted among neonates in the EMLA group based on persistently higher NIPS scores observed especially during tying and cutting. This result is similar to the finding by Butler-O’Hara et al11 who noted significantly higher NIPS scores among the patients who had EMLA cream during lysis of adhesions and tying. However, a different observation was made by Sabeen Mujeeb et al8 who noted significantly higher NIPS scores during crushing and cutting among patients who had DPNB with lidocaine. These differences may be attributed to interobserver variability in scoring as well as to the fact that the behavioral changes assessed in the NIPS may be affected by factors other than pain, such as hunger or discomfort due to restraint.
Changes in HR and levels of transcutaneous SpO2 have been studied in neonates experiencing pain and have been found to correlate. HR has been documented to increase and SpO2 to decrease in response to acute procedural pain in infants.10 31 32 We observed that the HR was comparatively lower in the DPNB group than in the EMLA group during crushing, tying, and cutting, but the difference was not statistically significant. This result is similar to the finding by Howard et al30 who noted lower HR in all the surgical steps among the patients in the DPNB group with statistical significance only seen during the postoperative observation. However, compared with the baseline, a statistically significant increase from the baseline HR was seen in all the surgical steps in the EMLA group and the trend showed a steady rise. The lowest mean rise in HR was 9.0725 bpm observed at clamping, and the highest was 21.1449 bpm during cutting. Crushing, tying, and cutting are steps associated with more tissue damage compared with clamping. The continuous rise in HR observed in this study is similar to the findings of Taddio et al33 who noted that although EMLA decreased the pain associated with circumcision, its effectiveness was considerably less during steps associated with extensive tissue damage.
In the DPNB group, a statistically significant increase in HR was seen only in clamping and tying. During crushing and cutting (which are associated with more tissue damage), the increase in HR was not statistically significant, indicating good pain control. The highest mean rise in HR was 11.246 bpm observed at tying while the lowest was 0.492 bpm at crushing. These findings correlate with reviewed literature where higher increase in HR from baseline was noted among infants who had EMLA cream.
In the present study, the changes in SpO2 were similar to the findings of Sabeen Mujeeb et al8 who also noted a decrease in SpO2 throughout the procedure without any statistically significant difference between both groups. Michael Holliday34 et al who compared DPNB with lidocaine versus placebo also noted a similar decrease in SpO2 in both groups. These findings may be attributed to a known fact that movement produces artifactual desaturation on pulse oximeter readings. This is a limitation in the use of pulse oximetry in determining SpO2 in moving subjects.35 36
Postoperative salivary cortisol levels were significantly elevated in both groups of patients when compared with the baseline, indicating some level of stress experienced by the neonates during the procedure. However, overall, the higher mean increase in salivary cortisol observed with the EMLA group compared with the DPNB group probably indicates better pain control with DPNB as the rise in salivary cortisol correlates with the degree of stress or pain. The difference between the groups was not statistically significant indicating that the stress associated with the procedure was not completely eliminated. This finding is similar to the observation by Masciello37 where the rise in serum cortisol between patients who had DPNB with lidocaine and patients who had placebo prior to circumcision were compared. Both groups of patients demonstrated a significant rise in cortisol. Though the group who had placebo had a higher rise, the mean difference between the groups was also not statistically significant. The probable explanation for this finding is the fact that adrenocortical response is triggered through different pathways, the afferent nerve pathway being one. If this is adequately blocked by regional or topical anesthesia, cortisol levels may still rise via the epinephrine-mediated pathway, which may be triggered in infants by the restraints, handling, and discomfort during the procedure.
Use of EMLA cream results in additional waiting time. EMLA cream requires at least 45 min to 1 hour following application before its anesthetic effect is achieved.22 38 In addition, the degree of absorption cannot be entirely predicted as it depends on factors such as skin thickness and amount of ointment applied. For example, in a previous study by Hymes and Spraker39 investigating racial differences in the effectiveness of EMLA cream, black subjects had a smaller reduction in pain than whites, presumably because of the increased density of the stratum corneum observed in blacks. In contrast, the anesthetic effect of lidocaine given via needle infiltration is observed within 3 min.11 37 In this study, a 1 hour waiting time was observed for both groups because of the EMLA cream.
Complication rate was low in this study. Mild erythema of the penile shaft was noted in one patient (1.4%) in the EMLA group and none in the DPNB group. Rana Sharara-Chami et al38 and Sabeen Mujeeb et al8 did not record any untoward effect in their patients who had EMLA cream. In contrast, Butler-O’Hara et al11 noted that 3 of his 25 patients (12%) who had EMLA cream developed penile erythema, while Lehr et al31 also noted erythema in 2 out of the 17 patients (11.7%) in their study. The lower percentage observed in this study compared with the latter studies may probably be due to the fact that erythema is less obvious on a black skin compared with a Caucasian skin as these studies were done on Caucasian patients. However, the penile shaft erythema among patients in this study was self-limiting and was completely resolved within 72 hours, similar to the observations in compared studies. No pallor or blister formation, which have been reported in some studies, was seen.25 34 Three of the patients in the DPNB group and one in the EMLA group who developed penile edema were noted to have had long durations of procedure (>10 min), which may have contributed to the edema seen. However, these patients all resolved spontaneously within 1 week postclinic visit. No hematoma was seen in any of the patients, which is similar to the findings in some previous studies.31 34 Overall, there was no significant difference in complication rate between the two groups.
We acknowledge some limitations with this study. The duration of circumcision as well as the interval between the designated steps is relatively short to measure the changes in physiological parameters. Thus, there may have been overlap in parameters measured during the steps. In addition, being a single center study, conclusions based on a single population may not be accurate as pain perception and sensitivity varies among individuals, races, and ethnic groups.40
In conclusion, better pain control and less stress are achieved with use of DPNB with lidocaine during neonatal circumcision compared with EMLA cream. In addition, both methods are safe. Finally, all neonates undergoing circumcision should have the benefit of anesthesia.
Data availability statement
Data are available on reasonable request. Individual participant data that underlie the results reported in this article after deidentification (text, table, figures, and appendices).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University of Benin Teaching Hospital Ethics and Research Committee. Reference number–ADM/E 22/A/VOL.VII/260. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This study was culled from the dissertation of the corresponding author submitted to the West African College of Surgeons as part of the Fellowship examinations in Pediatric Surgery. Special thanks to Dr Ndubuisi Mokogwu for his immense and invaluable input in the data analysis during the preparation of this manuscript.
References
Footnotes
Twitter @victorcemordi
Contributors VCE is the guarantor of the study and contributed to conceptualization, data curation, formal analysis, methodology and writing original draft. DOO contributed to Methodology, resources, writing, review and editing and supervision. IE contributed to writing, review and editing and supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.