Article Text

Statistics from Altmetric.com
Biliary atresia (BA) is a rare life-limiting fibro-obliterative disorder of the bile ducts that can advance to end-stage liver disease, with an incidence of approximately 1:8000–1:18 000.1 BA is characterized by the onset of persistent cholestatic jaundice during the neonatal period, yet the underlying etiology is not well understood. However, about 10% of infants with BA exhibit other congenital anomalies—a distinctive subgroup commonly referred to as biliary atresia splenic malformation (BASM) syndrome and others such as polysplenia or polysplenia syndrome.2 The incidence of the syndromic form of BA is lower in Japan and South Asia.3
Over 80% of infants affected with this syndrome have splenic abnormalities (eg, polysplenia, double spleens, asplenia) with or without situs inversus, preduodenal portal vein, absent inferior vena cava, malrotation, and cardiac anomalies.4 These disturbed vascular anatomies and structural abnormalities indicate that BASM syndrome may occur in the embryonic development stage.5 Currently, BA is uniformly fatal without timely Kasai operation and eventually requires liver transplantation. Timely Kasai operation is the standard treatment for BA, so infants with BASM syndrome usually also undergo intraoperative cholangiography and subsequent surgery. In terms of etiology and clinical manifestations, BASM seems to be a distinct subgroup, compared with the largest subgroup of non-BASM, isolated BA, with a different timing of onset and a worse prognosis in BASM population.6 Recently, with the indepth study of the disease, BASM has been reported to be comparable with patients with isolated BA in terms of native liver and overall survival rates.7 In fact, the outcomes of patients with BASM after a Kasai operation are still not clear. The aim of this study was to compare the outcomes of infants with and without BASM after a Kasai operation. We sought to speculate on the prognostic significance of the Kasai operation in BASM syndrome.
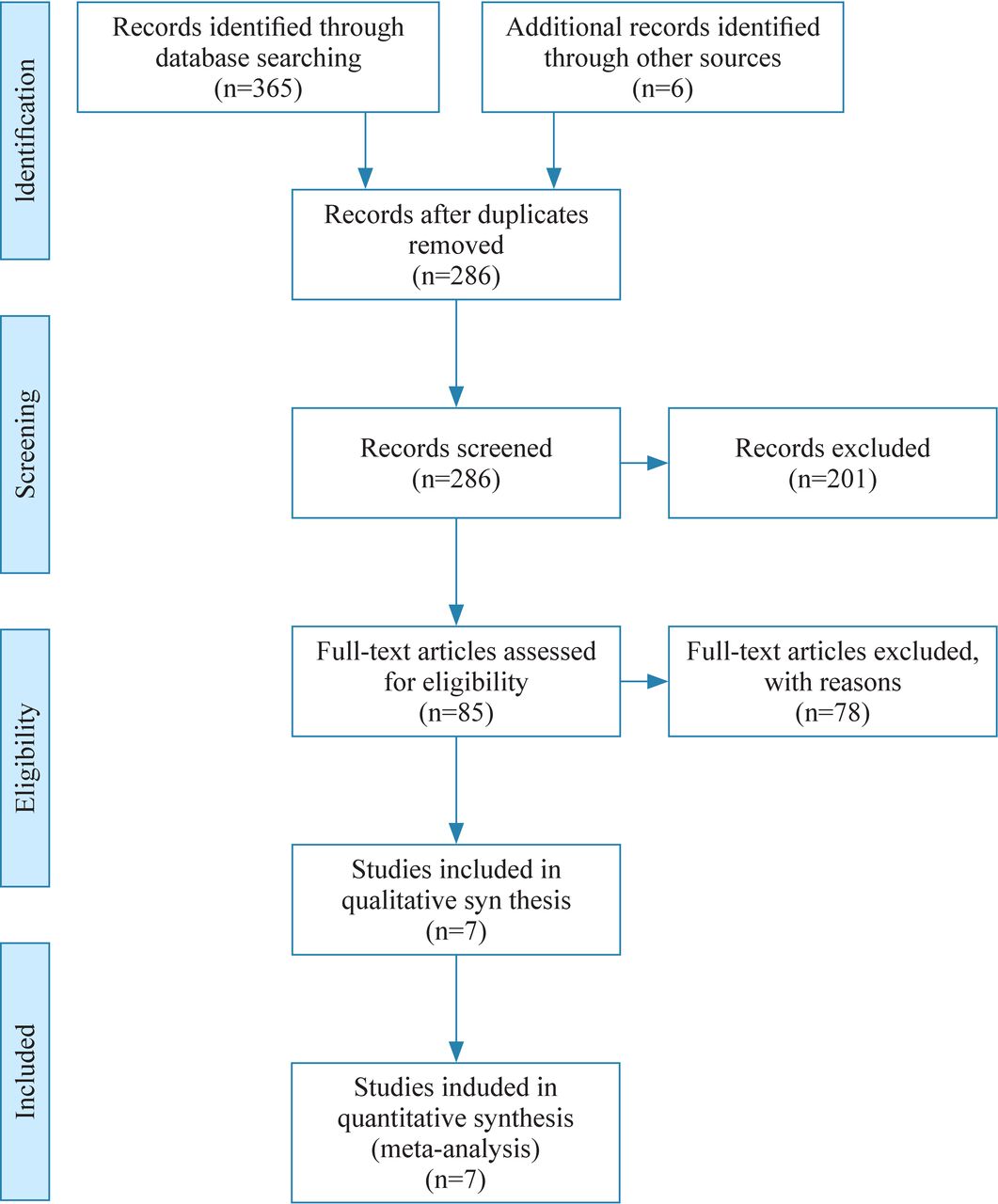
The study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (figure 1). The electronic databases PubMed, Embase, and Cochrane Library were searched to find studies up to the present that are eligible for the meta-analysis. The literature was not restricted by year of publication, but the language needed to be in English. The following were the keywords used: [“Biliary Atresia” [Mesh]] OR (Biliary Atresia) OR (Atresia, Biliary) OR (Intrahepatic Biliary Atresia) OR (Atresia, Intrahepatic Biliary) OR (Biliary Atresia, Intrahepatic) OR (Biliary Atresia, Extrahepatic) OR (Atresia, Extrahepatic Biliary) OR (Extrahepatic Biliary Atresia) OR (Idiopathic Extrahepatic Biliary Atresia) OR (Familial Extrahepatic Biliary Atresia) OR (biliary atresia) OR (bile duct atresia) AND [“Splenic Malformations” [Mesh]] OR (Splenic Malformation) OR (Malformation, Splenic) OR (Splenic Anomalies) OR (Anomaly, Splenic) OR (Splenic Anomaly) OR (Polysplenia Syndrome) OR (Polysplenia Syndromes) OR (Syndrome, Polysplenia) OR (Syndromes, Polysplenia) OR (Asplenia Syndrome) OR (Asplenia Syndromes) OR (Syndrome, Asplenia) OR (Syndromes, Asplenia).

Flow chart of the study selection process.
The inclusion criteria were (1) clinical controlled studies comparing the outcomes of patients with and without BASM after a Kasai operation; and (2) studies that included at least one of the following outcomes: ‘jaundice clearance’ (JC) and ‘native liver survival’ (NLS). If cases in two or more studies overlapped, the overlapping cases were not included in the same set of effect indicators for comparison. Case reports, review articles, letters, conferences, and poster abstracts were excluded from the present meta-analysis. Eligibility for inclusion in the analysis was assessed independently by two researchers. Disagreements in study selection were resolved by consensus, and then one of the authors reviewed the results and approved the selected studies according to the above criteria.
Once the database search was completed, all duplicates were removed. The titles and abstracts of all retrieved publications were reviewed, and the selected studies were further reviewed in full text. All the contents of each selected article, including relevant papers in the reference list, were thoroughly reviewed and examined. We used the term BASM as suggested by Davenport 4 to encompass all variants of splenic malformation. The following information was extracted from each selected study: year of publication, investigators, country, study period, number of patients, age at Kasai operation, JC, and NLS.
All analyses were performed using RevMan software (V.5.3; Cochrane Collaboration). Odds ratio (OR) with 95% CI was computed according to the reported number of total and events. For continuous outcomes, mean differences (MD) were calculated and pooled using the inverse-variance method. When continuous variables were reported by the sample median, a novel approach proposed by McGrath et al8 was used to estimate the sample mean and standard deviation (SD) through the web page https://smcgrath.shinyapps.io/estmeansd, performing quantile estimation method or the Box-Cox method. Heterogeneity was assessed using I2 statistics, where I2 >50% was deemed to be of substantial heterogeneity. A random-effects model was employed and leave-one-out sensitivity analyses of exclusion were performed in the presence of substantial heterogeneity. Subgroup analyses were used to assess independent variables. P<0.05 was considered statistically significant.
The flow chart of the search results is shown in figure 1. In total, 365 studies (189 on PubMed, 130 on Embase, and 46 on Cochrane Library) were identified by our search strategy. After removal of duplicates, 286 studies remained for initial screening by titles and abstracts. Further, 85 full-text articles were selected for full-text assessment and 78 were excluded (without full text, without sufficient data, or with irrelevant content). Finally, seven articles met the inclusion criteria. The characteristics of the studies included in the meta-analysis are shown in table 1.
Characteristics of the studies included in the meta-analysis
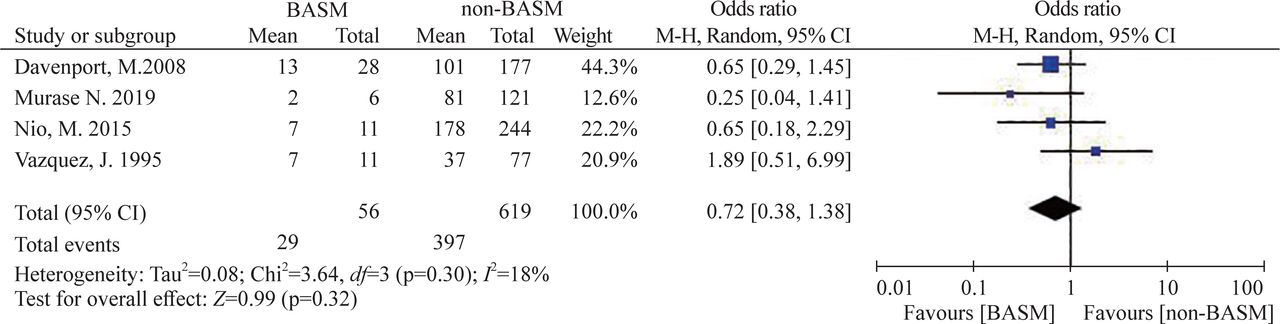
All included studies were retrospective studies in English, published between 1995 and 2019. JC was described in four selected articles and NLS was described in six articles. Cholangitis and hepatopulmonary syndrome (HPS)/portopulmonary hypertension (PPH) were found only in one article, which could not be processed. Three studies,7 9 10 with a total of 564 patients (BASM=65, non-BASM=499), recorded the age at Kasai operation. The pooled result showed a significant difference in age at surgery between the two groups (MD=−11.23 days, 95% CI −16.95 to −5.52 days; p=0.0001), with no heterogeneity (I2=0%) (figure 2). Four studies,7 9 11 12 including a total of 675 patients (BASM=56, non-BASM=619), reported clearance of jaundice. In terms of JC, there was no significant difference between the two groups (OR=0.72, 95% CI 0.38 to 1.38; p=0.32), with low heterogeneity (I2=18%) (figure 3).

Forest plot of age (days) at Kasai operation in BASM and non-BASM group. BASM, biliary atresia splenic malformation; IV, inverse-variance.
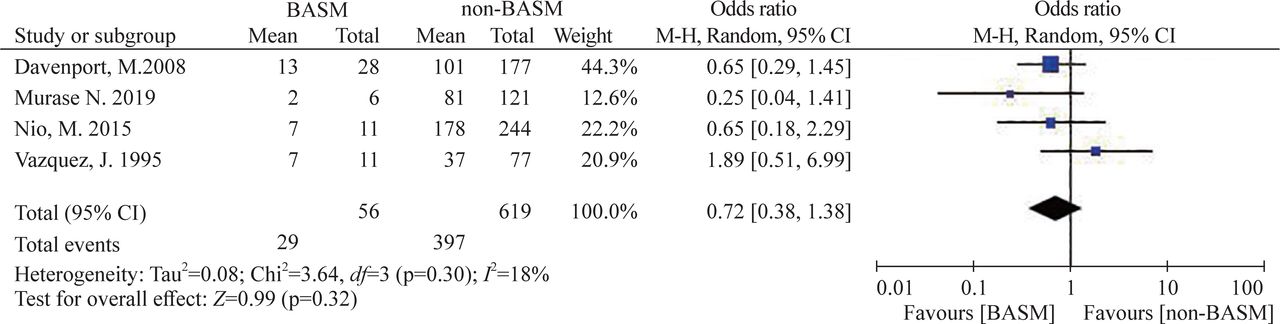
Forest plot of jaundice clearance after Kasai operation in BASM and non-BASM group. BASM, biliary atresia splenic malformation; M-H, Mantel-Haenszel.
Six studies,7 9–11 13 14 with a total of 2017 patients (BASM=184, non-BASM=1833), described the rate of NLS. The pooled result was not clearly different between the two groups (OR=0.76, 95% CI 0.46 to 1.26; p=0.28), with low heterogeneity (I2=24%) (figure 4). In the subgroup analyses, the pooled OR was 0.40 (95% CI 0.09 to 1.77; p=0.23) in studies that described 2-year NLS. The OR was 0.55 (95% CI 0.11 to 2.85; p=0.48) in the study that described 1-year NLS, 0.78 (95% CI 0.21 to 2.86; p=0.71) in the study that described 4-year NLS, and 1.16 (95% CI 0.64 to 2.08; p=0.63) in the study that described 20-year NLS (figure 5).

Forest plot of native liver survival after Kasai operation in BASM and non-BASM group. BASM, biliary atresia splenic malformation; M-H, Mantel-Haenszel.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of native liver survival after Kasai operation in BASM and non-BASM group according to the follow-up time. BASM, biliary atresia splenic malformation; M-H, Mantel-Haenszel.
We included seven articles that described the outcomes between patients with and without BASM and that analyzed the data on their prognostic indicators. Apparently, Kasai operation was performed at an earlier age in BASM compared with non-BASM. Although the BASM group had a trend of worse outcomes, there was no significant difference between these two groups in terms of JC and NLS.
BASM syndrome is a special subgroup of BA. This form has been termed syndromic BA (<20%), in contrast to non-syndromic BA (>80%), because it is considered as a result of the pathological process during the embryological phase of organ development, that is, the first trimester.6 15 16 Furthermore, the probability of having major extrahepatic anomalies is higher in patients with early-onset BA.5 In these infants, a small proportion of patients may have underlying genetic defects. Mutations in a small number of ciliopathy and laterality genes, including cryptic family 1 (CFC1) and polycystic kidney disease 1 like 1 (PKD1L1), have been suggested as a potential factor for BASM syndrome.17 18 In addition to the genetic factors that contribute to the pathogenesis of BASM syndrome, some cases of BASM seem to have been due to abnormal intrauterine environment, such as maternal diabetes.6 Therefore, it is worth exploring whether there are differences in the outcomes between the BASM and the non-BASM group.
BASM itself has been reported as a possible preoperative predictor of prognosis after a Kasai operation.19 Previously, authors of several studies believed that patients with BASM had a higher incidence of postoperative complications and an inferior prognosis to infants without BASM.6 10 20–22 Therefore, it has been believed that BASM is characterized by a subset of patients with BA with poorer prognosis. It is reported that the impaired prognosis in the BASM group may be due to the difficulty of Kasai operation when the BA is complicated by situs inversus, malrotation, and vascular anomalies.16 Moreover, the prognosis of patients with BASM seems to depend on the presence of associated cardiac defects.7 Because the prognosis is poor, BA with malformations may influence the choice of surgery.
However, several articles have provided conflicting data on patient outcomes. Studies have shown that the postoperative outcomes of patients with BASM are comparable with those without BASM.7 16 23 24 While surgical procedures are challenging in these patients, the anomalies do not prevent successful biliary reconstruction using Kasai operation.16 Although important factors affecting prognosis have been recognized, such as the presence of laterality features, age at the time of surgery, and experience at the surgical center, the postoperative conditions of individual patients are largely unpredictable as there may be many other factors that simultaneously determine the progression of the disease. Moreover, many articles have less case data and the conclusions are inevitably biased. Perhaps an increased cohort size will allow us to further study important questions about the prognosis of this important subgroup of patients with BA.
It is generally believed that the onset of BASM is earlier than that of non-BASM, and this study confirmed that the age at Kasai operation was significantly different between the two groups. We speculate that children with BASM have an early onset of biliary obliterans and are more likely to be diagnosed and to accept Kasai operation at an earlier age.10 After a Kasai operation, many patients present with postoperative complications associated with BA, indistinguishable from those with BASM, namely jaundice, cholangitis, HPS, and portal hypertension with variceal bleeding. These factors may affect the survival of patients. For NLS in children with BA, the follow-up time varied among studies. Therefore, a subgroup analysis of the different follow-up times was performed in our study. The overall results confirmed no significant difference in NLS between patients with and without BASM. The same situation also occurs in JC. Therefore, patients with BASM should continue to be offered the potential benefits of a Kasai operation.
Cholangitis is often considered a risk factor for poor outcome after surgery, but data are incomplete and difficult to be included in the present study. HPS and PPH are less frequent but no less possibly devastating late complications of BA; both occur in a setting of portal hypertension.25 Compared with other chronic liver diseases, patients with BA had a higher risk of developing HPS, regardless of severity of liver disease and/or portal hypertension.26 The association of HPS and PPH with BASM has been reported previously, but the underlying mechanisms were unknown.7 This may be due to the higher prevalence of anatomical pulmonary arteriovenous malformations, which may be an intrinsic part of the syndrome, yet rarely documented.6
Notably, in addition to splenic anomalies, patients with BASM may also have other concomitant defects, such as cardiovascular and laterality defects.27 28 BA may also have any of the other several structural anomalies, and splenic dysplasia syndrome is not necessarily the most common deformity.3 A Canadian research found that a large proportion of BA with deformity only had congenital cardiac malformations and another large proportion included all intra-abdominal vascular abnormalities lacking splenic abnormalities.27 Therefore, the term BASM only stands for structural deformity with splenic malformation, which may lead to deviations in the understanding and analysis of the disease.
The limitation of this study was the small number of included articles that met the inclusion criteria, mainly due to the need for specific prognostic data on BASM and non-BASM. In addition, all studies included in this meta-analysis were retrospective studies and the low level of evidence will affect the results. NLS in the study is a time-dependent event and is more suitable for analysis using time-to-event analysis, such as a Kaplan-Meier analysis or a Cox regression analysis. However, in the few included studies, none described sufficient data for analyses. In particular, it is biased to compare the survival of native liver according to different lengths of observation time after surgery. Subgroup analysis was performed to verify the results. Although we have tried our best to extract research variables of the same standard, there are still some undefined criteria for JC in the studies, which may lead to data bias. Despite initial recognition of the prognosis of BASM, the prognosis of each patient will most likely be unpredictable. Many factors may affect disease progression, so whether different deformities will lead to a different prognosis is worthy of further discussion.
In conclusion, our data suggest that the outcomes of BASM syndrome were not significantly different from those of non-BASM, except for the earlier age at surgery in BASM. Thus, it is necessary to perform Kasai operation in time after BASM diagnosis, and full clinical management should not be simply attenuated. However, the potential for poor prognostic trends is cautionary and may require careful follow-up of patients with BASM. Additional studies may allow us to enhance our understanding of BASM syndrome and to develop a more comprehensive view of other BA-associated malformations.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
XX and RD contributed equally.
Contributors XX contributed to writing original draft. RD contributed to data curation. SZ contributed to data curation. JFZ contributed to formal analysis. QG contributed to formal analysis. LW contributed to investigation. JHZ contributed to writing, review and editing.
Funding This study was supported by grants from Xinjiang Uygur Autonomous Region Science Foundation Projects (grant numbers 2019D01A12 and 2021D01A38).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.