Article Text

Statistics from Altmetric.com
Acute upper airway obstruction (UAO) in children is a common disease in the emergency department. It is life-threatening and usually caused by laryngospasm or laryngeal edema owing to infection, allergy, or a foreign body.1 In addition, pediatric UAO can also be the result of laryngopharyngeal space-occupying lesions, such as laryngeal papilloma, lymphangioma, hemangioma, or cyst. Malignancy is uncommon.
Inflammatory myofibroblastic tumor (IMT) is a mesenchymal tumor consisting of differentiated spindle fibroblast cells with plasma cells and/or lymphocytes infiltration. The most common sites of IMT are the lungs, gastrointestinal tract, urogenital tract, abdominal cavity, viscera, central nervous system, upper respiratory tract, and soft tissue. IMT in the head and neck region accounts for only 14%–18% of extrapulmonary lesions, of which the orbit and nasal sinus are common locations.2–4 According to the reported cases of laryngeal IMT (fewer than 50 cases), it is usually confined to the glottic region. A lesion with supraglottic and hypopharyngeal involvement is extremely rare and only five cases have been reported in the hypopharynx to date. These cases occurred in adults, including only one female patient.5–9 We describe an extremely rare case of giant IMT in the hypopharynx of a female child with respiratory distress as the initial symptom.
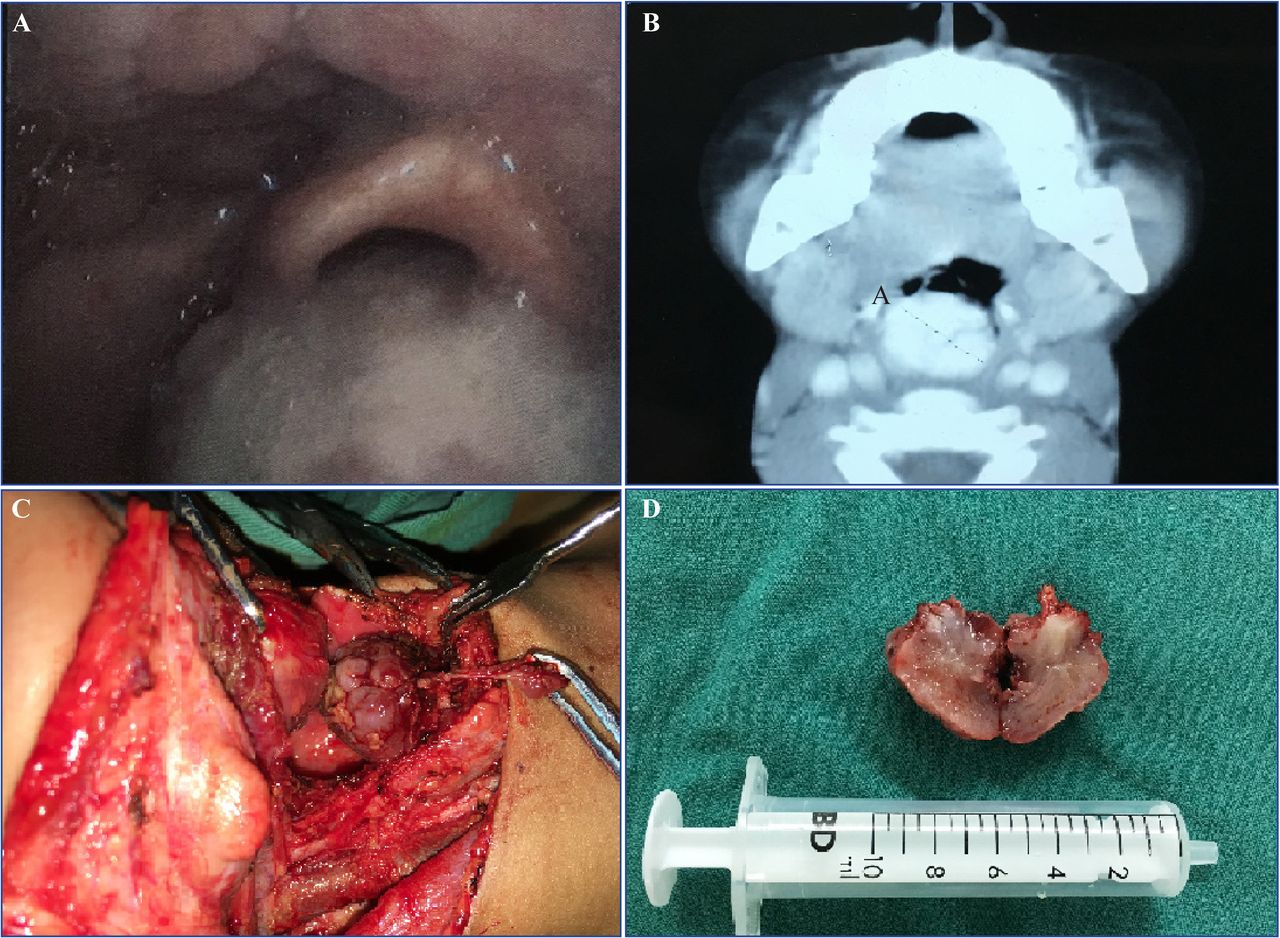
A 6-year-old girl was referred to the emergency department of our hospital with progressive dyspnea, stridor, cyanosis, and dysphonia. Hoarseness was not obvious, but a change in her voice and snoring had been present for 4 months. Acute upper respiratory infection, anaphylaxis, and airway foreign body were excluded following detailed postadmission medical inquiries. Compared with children of the same age, she showed stunted growth. Oxygen therapy did not completely relieve her dyspnea, and transient loss of consciousness was observed; therefore, tentative intubation was conducted but failed. A huge lump blocking the glottis was found during attempted intubation; thus, an emergency tracheotomy was performed. Subsequent laryngoscopy showed an exophytic tumor located in the right piriform sinus partially covering the laryngeal entrance (figure 1A). Contrast-enhanced CT revealed a 30 mm×20 mm×20 mm mass with evident homogeneous enhancement occluding the entrance to the larynx (figure 1B). Routine laboratory tests showed no abnormalities suggestive of infection or immune disorders. The preliminary diagnosis was malignancy of the hypopharynx. The patient underwent surgical exploration and an ill-defined tumor was found occupying the right piriform sinus and esophageal inlet. The cricoarytenoid joint was also involved. The tumor and the involved larynx were excised with the help of frozen sections to determine the safe margin (figure 1C). Ipsilateral enlarged cervical lymph nodes were also observed. The patient’s postoperative recovery was uneventful.
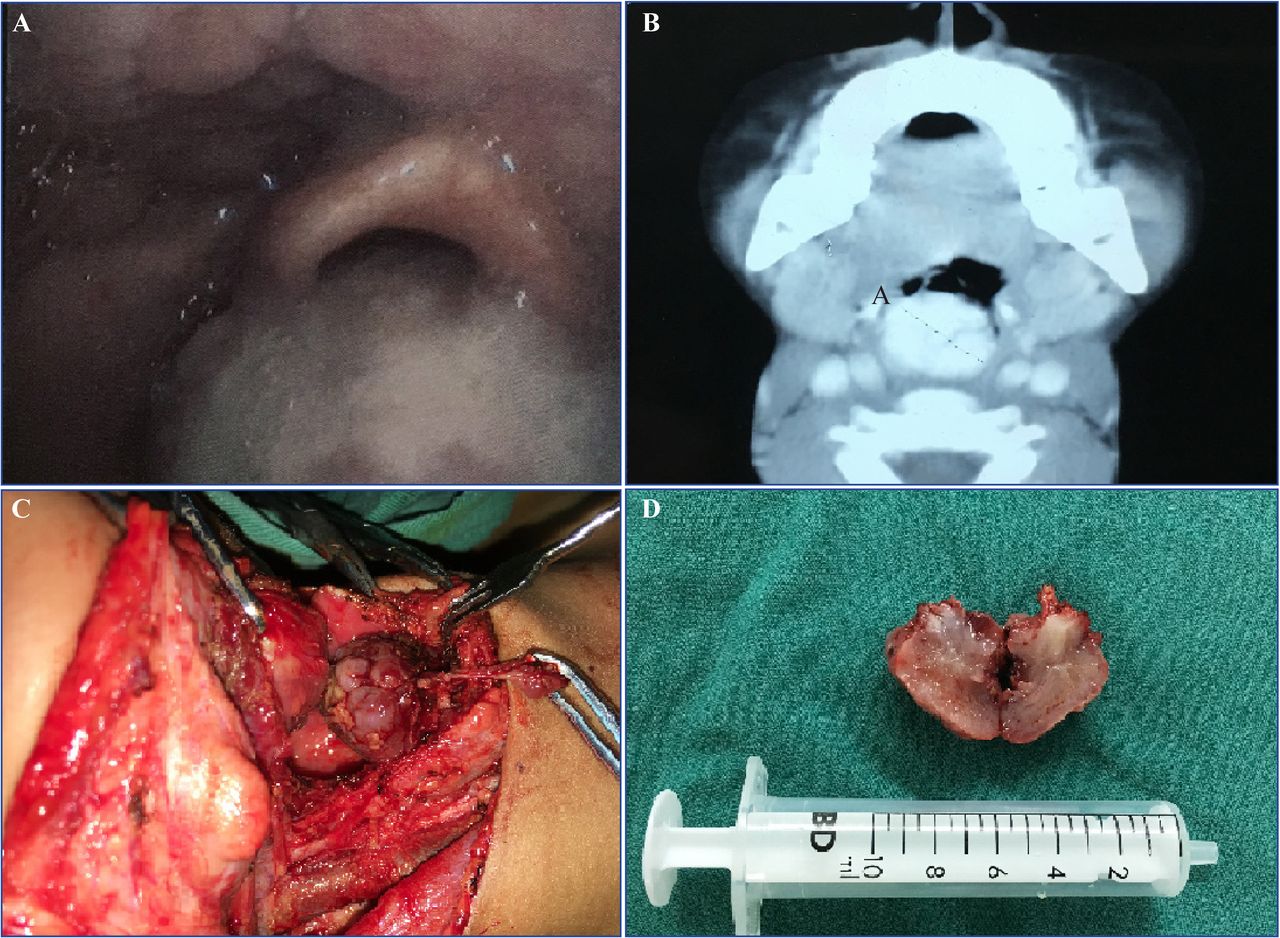
Laryngoscope, operative field and contrast-enhanced CT. (A) Endoscopic view demonstrated a mass obstructing the laryngeal entrance. (B) CT revealed a giant tumor occluding the pharynx at the same level in A. (C) The tumor was exposed through a suprahyoid transcervical incision. (D) Cross-section of the tumor revealed a white to tan appearance.
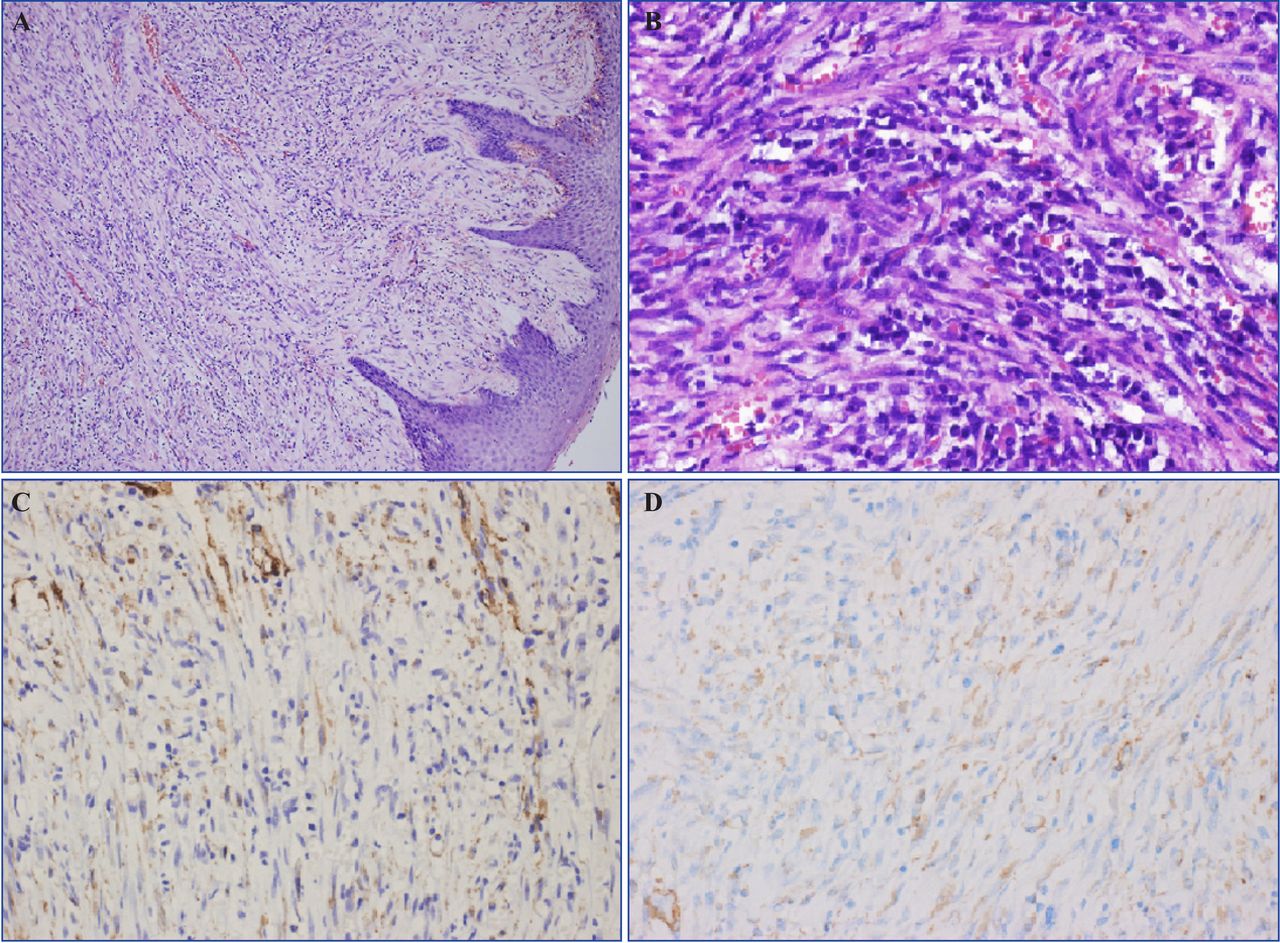
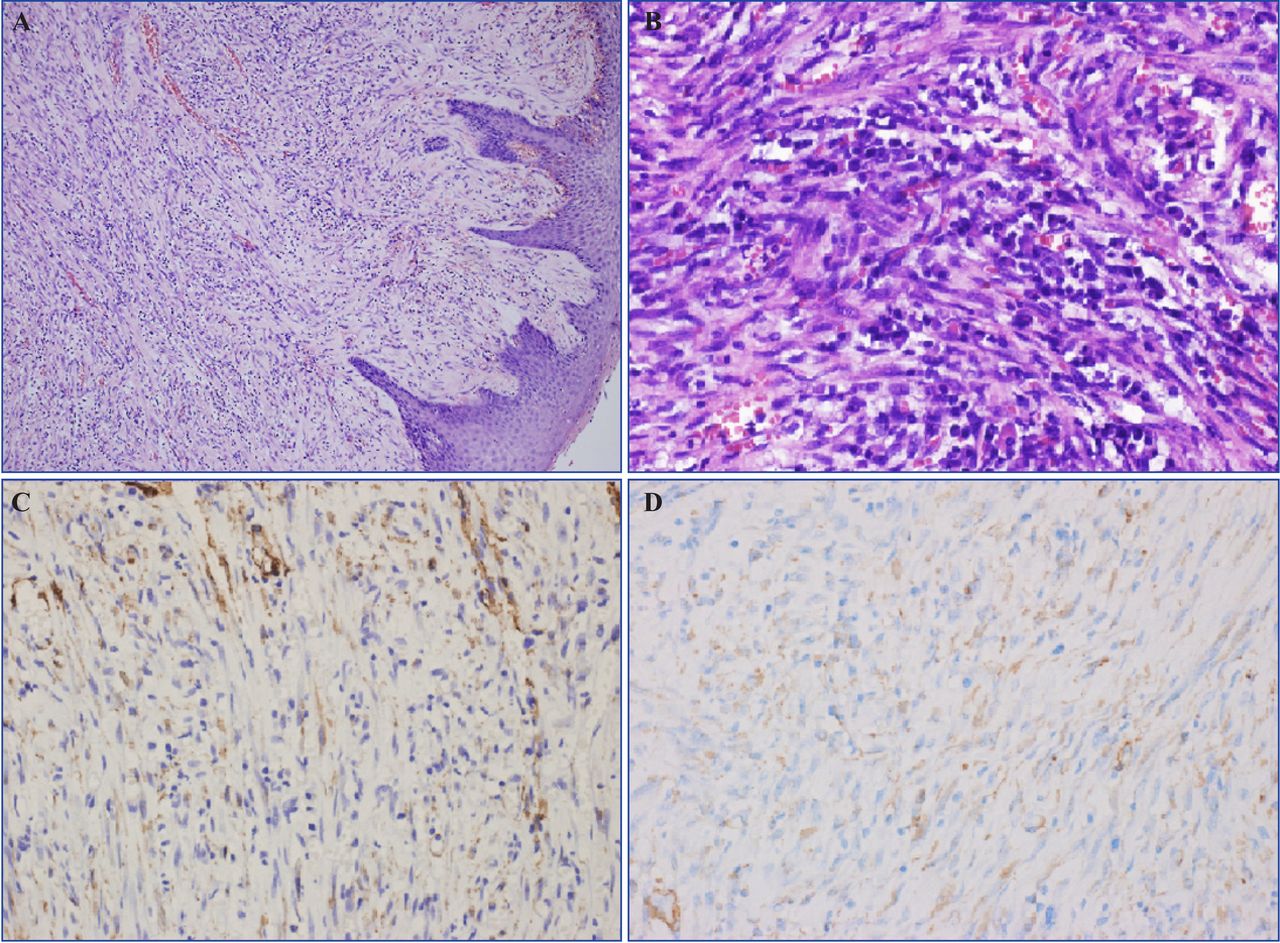
Macroscopically, the tumor was granular and fragile, covered by incomplete mucosa, with a white to tan gross appearance (figure 1D). Microscopically, spindle cell proliferation and inflammatory cell infiltration were observed in the tumor, while reactive hyperplasia in the lymph nodes was noted (figure 2A,B). Immunohistochemically, the spindle cells were positive for smooth muscle actin, myo-specific actin (figure 2C,D), and transducin-like enhancer of split 1 (weakly positive), and negative for anaplastic lymphoma kinase (ALK), epithelial membrane antigen, desmin, H-caldesmon, myogenin, P63, CD34, S-100, and Epstein-Barr virus-encoded RNA in situ hybridization. The proliferation marker protein Ki-67 (ki-67) index was 5%. A hypopharyngeal IMT was finally diagnosed. Three months after surgery, decannulation was achieved. She was able to communicate in a hoarse voice after decannulation. There was no evidence of recurrence during the 4-year follow-up period and the quality of the voice gradually improved.
{kind=link}
{kind=link}
Histological and immunochemical staining. (A) Spindle cells and lymphocytes infiltration under squamous cell hyperplasia of the overlying mucosa (H&E staining, original magnification ×50). (B) Spindle cells and lymphocytes infiltration (H&E staining, original magnification ×400). (C) The tumor cells were positive for MSA (immunohistochemical staining, original magnification ×400). (D) The tumor cells were positive for SMA (immunohistochemical staining, original magnification ×400). MSA, myo-specific actin; SMA, smooth muscle actin.
Acute UAO usually manifests as dyspnea and stridor and is more likely to occur in pediatric patients. In this condition, intrinsic and extrinsic etiologies should be differentiated so that immediate effective treatment can be given to the patient. Anaphylaxis, airway foreign body, acute epiglottitis, and laryngotracheitis should be considered initially.1 In addition, upper airway space-occupying benign lesions, such as laryngeal papilloma, hemangioma, lymphangioma, and retropharyngeal abscess, should also be considered. Although malignancy is uncommon, it can also be fatal if undiagnosed. A detailed medical history and careful physical examinations are important for diagnosis. Imaging and endoscopic examinations should be carried out as soon as possible if conditions permit. Early identification of airway stability or lability is vital in the management of children with acute UAO.10 Pediatric tracheotomy should be carried out as an elective procedure in extreme emergent situations, such as in patients with progressive aggravation of hypoxia after routine oxygen therapy, hormonotherapy, and intubation have been performed. In the present case, the tumor occluded the laryngeal entrance and made routine oxygen intake impossible.
IMT was previously named inflammatory pseudotumor, plasma cell granuloma, pseudosarcomatous inflammatory lesion, and so on. It is now recognized as a real tumor with uncertain behavior and etiology. Recurrence and metastasis of IMT have been reported in several isolated cases, and clonal cytogenetic aberrations have also been detected.4 9 IMT is very rare in the upper aerodigestive tract, and the larynx is the most common site.4 Hoarseness is the most common symptom in most reported laryngeal IMTs with glottic involvement, while acute UAO is extremely rare except in subglottic locations. In pharyngeal IMTs, dysphagia and globus sensation may be relevant mild symptoms. Unlike adults, IMT is very rare in children, especially in the head and neck region. Because pediatric IMTs usually mimic malignancy, such as sarcoma or lymphoma, surgery is the main therapeutic approach to cure the disease or to achieve a final diagnosis.11
The differential diagnosis of IMT should include spindle cell tumors with inflammation, such as IgG4-related diseases (IgG4-RD), inflammatory myomatous polyps (IFPs), inflammatory leiomyomas, etc. Approximately 16% of IgG4-RD cases may present as an inflammatory pseudotumor and these cases are usually accompanied by elevated levels of IgG4 in serum and tissues.7 Corticosteroid therapy is usually effective in these cases. IFP is characterized by eosinophil infiltration and immunohistochemistry shows CD34 positivity, which can differentiate it from IMT. Leiomyomas with lymphocytic infiltration are most easily confused with IMT. The spindle cells in leiomyoma are smooth muscle cells rather than myofibroblast cells. The degeneration of interstitial mucus is not obvious, and inflammatory cells are mainly small lymphocytes, whereas in IMT plasma cells and neutrophils are the main cells.
Hypopharyngeal IMT is extremely rare and only five case reports (four English articles and one Chinese article) were found through a PubMed search (table 1). The five cases were in one female and four male patients aged 49–74 years (mean 57.8 years). One malignant case was confirmed to harbor the 3a/b variants of the EML4-ALK fusion gene by genetic testing.9 The disease course is from 2 months to 2 years. The lesion usually occurred in the posterior wall of the pharynx. Globus sensation was the most common local symptom, followed by progressive dysphagia. Three patients presented with general symptoms, including weight loss and general malaise. Pharyngeal malignancy was considered in almost all patients prior to pathological results. Three of five patients underwent total resection transorally, and the patient with IgG4 IMT was treated with corticosteroids.8 The case of malignant transformation only received palliative surgical resection and subsequently succumbed to disease progression at 11 months postdiagnosis.8 From the reviewed literature, we concluded that hypopharyngeal IMTs occur mostly in adults and rarely affect respiratory function, and total resection is the preferred treatment for IMT.
Hypopharyngeal inflammatory myofibroblastic tumors in the literature
Although there is no consensus on the treatment of IMTs, complete excision is critical for cure and can result in a favorable prognosis in children. Anti-inflammatory treatment, chemotherapy, steroids, or immunomodulators as potential remedial and effective management strategies are recommended for adult patients who may not be able to undergo possible complete excision or in ALK-negative cases with a higher frequency of metastasis and invasiveness.12
In conclusion, in this child, the initial symptom of a large IMT was acute UAO. This report highlights the importance of differential diagnosis in a child with acute UAO. Following relief of acute UAO, wide excision of the tumor with safe margins should be carried out.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of West China Hospital, Sichuan University (ID: 20111108). Participants gave informed consent to participate in the study before taking part.
Footnotes
Correction notice This article has been corrected since it first published online.
Contributors LY contributed to investigation, visualization, original draft writing, review and editing. WL contributed to revising and final approval. Both authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.