Article Text

Abstract
Aim The purpose of the study is to compare the labial frenectomy between the laser surgery (erbium yttrium aluminum garnet and neodymium-doped yttrium aluminum garnet (Er:YAG and Nd:YAG)) and the scalpel method.
Methods The trial was a randomized controlled test. Thirty four patients aged from 5 to 10 years requiring the frenectomy were included in this study. Patients were randomly divided into two groups: group A: Er:YAG and Nd:YAG laser group and group B: scalpel group. In addition, this comparison considered the following factors: surgical time and Visual Analog Scale (VAS) pain score, which includes intraoperative pain, postoperative pain and complications, such as speaking and chewing, for 1 day and 7 days following labial frenectomy. After 3 months, we recorded the healing outcome by photos.
Results There was a statistically significant difference in mean surgical time between laser surgery (mean=224±59 s) and scalpel surgery (mean=740±168 s). According to VAS scores of the intraoperative period (3 hours after the operation and 1st postoperative day of pain), chewing and speaking were statistically higher in group B than those in group A; but in the 7th postoperative day of pain, there was no significant difference in speaking and chewing. After 1 month, all of the patient results were recorded, including the healing of wound and scar. Except for one patient in group B who had a scar, all patients achieved good results.
Conclusion Based on the results of this study, it can be concluded that Nd:YAG laser is an efficient and more comfortable alternative to the scalpel for a frenectomy in upper lip frenulum.
- pediatrics
- child health
- technology
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Previous studies have compared a single laser with the scalpel. With the development of the laser, we will take into consideration factors, such as a minimally invasive, painless, and effective procedure, postoperative comfort in the clinical work, and a classification of the labial frenulum.
What are the new findings?
Each laser has its own unique performance with specific advantages and disadvantages. This study reveals that we can get twice the result with half the effort by combining the characteristics of two lasers. The degree of cooperation of children is improved, and better outcomes in the postoperative experience are achieved.
How might it impact on clinical practice in the foreseeable future?
Owing to the limited survey samples, we need more samples to complete the subject comprehensively and objectively. There may be a new option for labial frenulum surgery. For some toddlers or patients with a thick frenulum, further study on the use of lasers is warranted.
Introduction
The frenulum is a band of mucosal folds connecting the mucosa of the alveolar process of the maxilla and the upper lip of the central incisor.1 As the alveolar bone grows vertically, the frenulum’s attachment moves toward the apex and shrinks.2 But the abnormalities of its size and location would cause the diastema of the front incisors, the limitation of the lip, speech and chewing, aesthetic problems and so on which used to solve with surgical excision.1 In 1974, Mirko et al analyzed 465 cases, based on the upper lip frenulum and maxillary incisor in periodontal tissue and the relationship between periodontal membrane, divided into four types: mucosal adherence, gum adhesion, gingival papilla adhesion and through the gingival papilla attachment type.3 Abnormal attachment of the upper labial frenulum is one of the main causes of excessive space between maxillary central incisor space. When the upper lip is pulled, it causes the gingiva papilla to whiten, and when the maxillary midline space is larger than 2 mm, it rarely closes naturally with growth and development.4 The site of attachment of the upper lip frenulum is closely related to facial aesthetics, patient age and maxillary central incisor space. The recovery of the upper labial frenulum is also related to the prevention of central incisor suture formation, prevention of orthodontic recurrence, aesthetic psychological factors, diastema closure, bone loss for muscle traction, limitations in lip mobility, brushing the maxillary anterior teeth with less traumatic pulling of the gingiva, and/or tethering of the upper lip by the frenum, leading to hypomobility of the philtrum of the upper lip and improved bilabial speech sounds.5 6
Histological studies have shown that the collagenous fibers in the upper labial frenulum divide the periodontal tract, which is strongly associated with the middle maxillary space.7 Frenectomy is described as a surgical excision including periodontal muscle fibers which are removed. In the past decades, the scalpel was the classic frenectomy with different methods, such as Miller’s technique, Z-plasty, and V-Y plasty.8–10 With the development of the laser, CO2, erbium (Er):yttrium aluminum garnet (YAG), and neodymium-doped YAG (Nd:YAG) were reported to use for frenectomy because of more patient acceptance, safer, less bleeding and more effectiveness.11 According to the characteristics of different wavelengths of laser, the ways of cutting soft tissue are different. Many researchers have reported the advantages of each individual kind of laser. Therefore, we did not find articles to use Er:YAG combined with Nd:YAG laser in frenectomy surgeries. The purpose of this study was to compare the scalpel technique with the Er:YAG combined with Nd:YAG laser technology to complete the frenectomy procedure, mainly including surgical time, electrocoagulation or suture, interoperative pain, 3-hour postoperative pain, uncomfortable speech and chewing on the 1st day and the 7th day after the operation. One month later, we observed the differences between the two groups by follow-up photographs.
Material and methods
The subjects were randomly assigned into two groups as a ratio of 1:1. It was accomplished at the Department of Pediatrics, Hefei Stomatological Hospital. The inclusion period started in November 2019 and ended in April 2021.
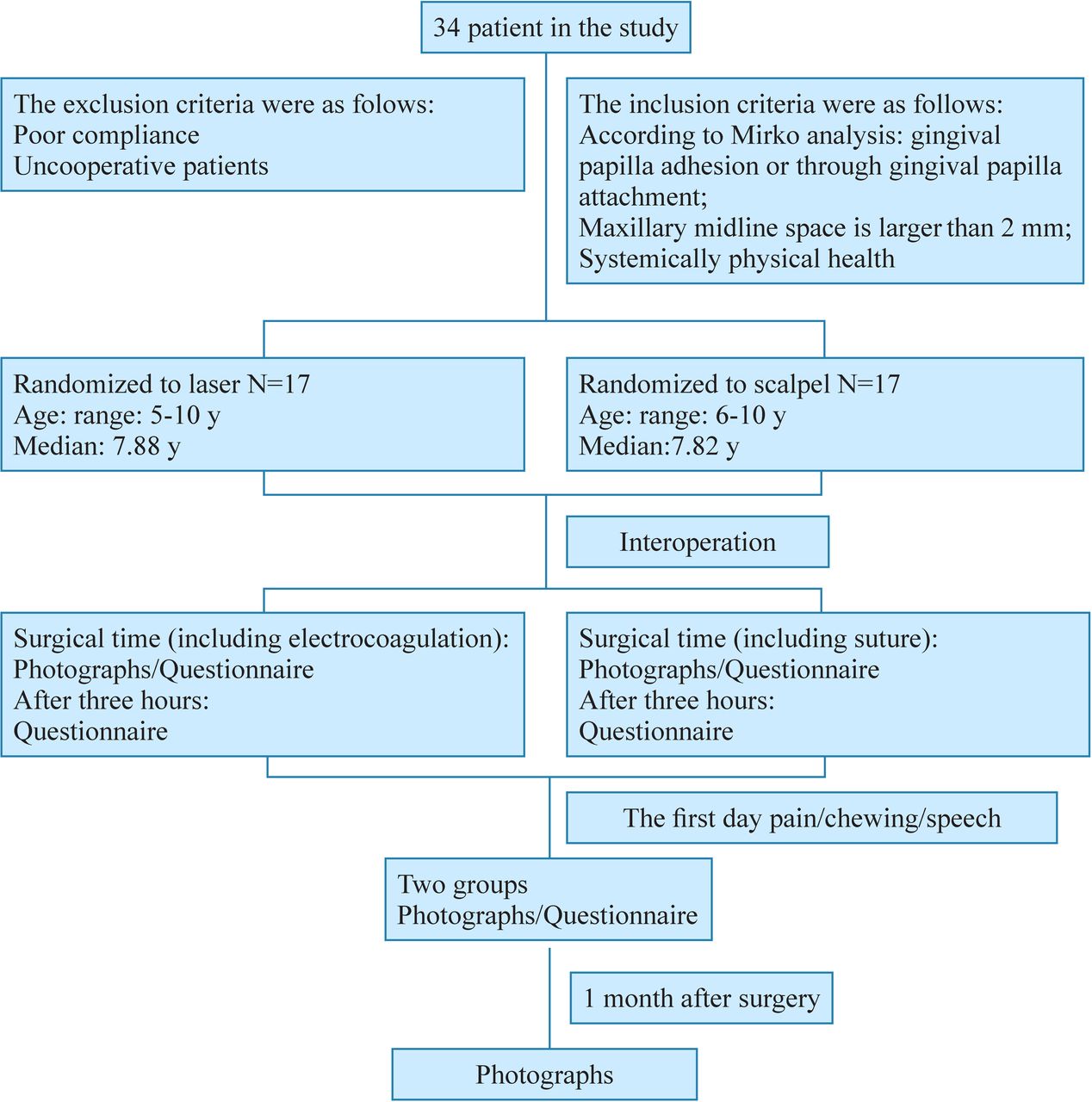
Totally, 34 children (5–10 years old) were invited to participate in this study. According to a simple randomized, double-blinded clinical trial, they were divided into laser group and scalpel group. The randomization method was carried out as indicated below: the designer in charge of randomization, without participating in the treatment, obtained the random number through the computer system, and finally formed the random assignment (table 1). All participants who were eligible to participate remained unaware of the method of the surgery. At the same time, the parents were provided with information sheets and signed informed consent. Patient recruitment and follow-up flow diagram is given in figure 1.
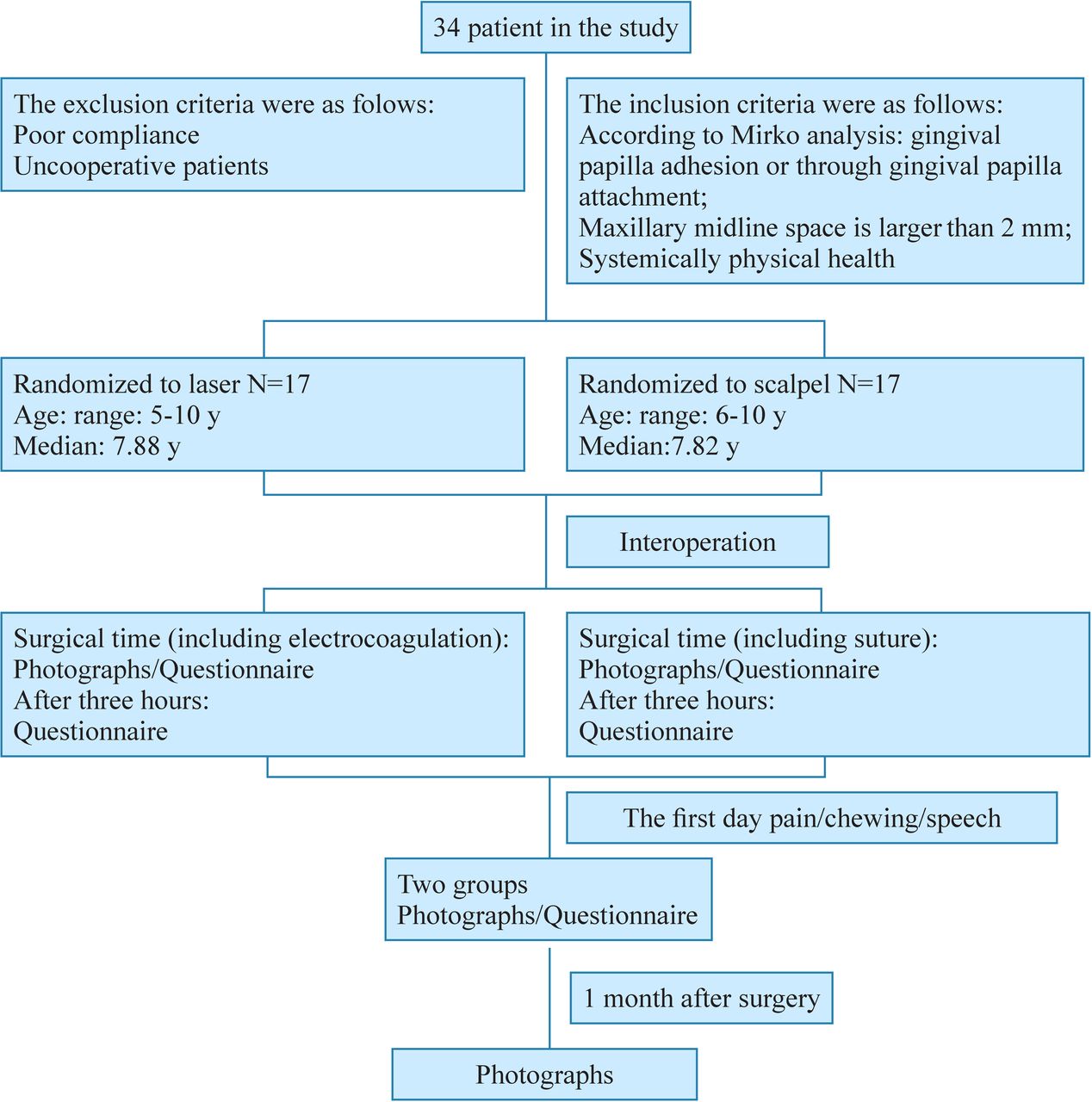
Patients’ recruitment and follow-up flow diagram.
The inclusion criteria were as follows:
According to Mirko analysis: gingival papilla adhesion or through gingival papilla attachment.
Maxillary midline space is larger than 2 mm.
Franke Behavior Rating Scale (FBRS) is rated 3 or 4 after local anesthesia.
Systemically physical health.
Good oral hygiene.
The exclusion criteria were as follows:
Poor compliance.
Being uncooperative with the dentist.
Speech problems.
Randomization
Patients were randomly divided into two groups, and the final sample consisted of 34 patients with a ratio of 1:1 (17 participants in each group).
There were 17 patients in group A (9 boys and 8 girls; with a median age: 7.88 years), 17 patients in group B (10 boys and 7 girls; with a median age: 7.82 years). Sex distribution characteristics for the study groups are listed in table 1.
Patient characteristics for the study groups (p<0.05)
Treatment procedure
All patients were treated with 4% articaine under Single Tooth Anesthesia (STA-5220 USA), painless local infiltration anesthesia. Group A used Er:YAG and Nd:YAG laser. First, Er:YAG laser, with the wavelength 2940 nm, (Lightwalker, Fotona, Slovenia) with handpiece H02-N and no working point hand tool. Cutting parameters were set as pulse width: short pulse (SP); energy: 60 MJ; frequency: 30 Hz; power: 1.80 W; water: 2; gas: 3, until extended to the vestibular sulcus. Subsequently, Nd:YAG laser, cylindrical, sapphire fiber tip, lightly contacted with bleeding surface electrocoagulation which parameters were set as pulse width: very long pulse (VLP); frequency: 20 Hz; power: 4.00 W. Simultaneously, the laser head was moved back and forth and 1 mm away from the tissue for therapy mode which parameters were set as pulse width: median short pulse (MSP); frequency: 15 Hz; power: 1.50 W. There was no suture. Group B used sterile scalpels, #11 (Lianhui, Shanghai), 4-0 absorbable suture after incision (HJ4901, Suzhou Medical), the stitches were removed after 1 week. All of the cases were recorded by photographs (figure 2).

{kind=link}
{kind=link}
Clinical images showing labial frenectomy with Er:YAG laser technology (A–E) and with the scalpel technique (F–J). A+F=before surgery, B+G=immediately after surgery, C+H=after 1 day, D+I=after 7 days, E+J=after 1 month. Er:YAG, erbium yttrium aluminum garnet.
Evaluation
Surgical time
The cases were all used with STA, just calculated surgery duration.12 The process of group A included laser surgery and electrocoagulation. Afterwards, the process of group B consisted of scalpel surgical time and suturing.
Scoring of pain
Visual Analog Scale (VAS) was labeled as VAS-10 cm to rate the experienced pain of each patient, to assign their verbal descriptors to typical numeric pain scale between the two anchors ‘no pain’ and ‘worst pain imaginable’.13 The line is marked with whole numbers from 0 to 10, the pain increases as the number increases. The patients were asked to mark their level of discomfort on the intraoperative period and 3 hours after the operation, 1st and 7th postoperative days. The patients were asked to record the degree of pain and the discomfort during eating and speech on the postoperative 1st and 7th days between 0 and 10 by VAS.
All assessments and data collections were performed by the same examiner who was unaware of the patients’ method.
Questionnaire
The patients were asked through questionnaires to rate their degree of pain during the operation, 3 hours after the operation, as well as pain and discomfort during chewing and speaking on the 1st day and 7th day. At the same time, all of these procedures were recorded by photos. After a month, we took photos again to record them. Questionnaires mainly consisted of birthday, name, symptoms, and FBRS. All of these questionnaires were recorded by the same examiner who could not take part in the process of the surgery.
Statistical analysis
Two groups’ sex distributions were compared using a Χ2 test. Age and surgical time were calculated with Wilcoxon rank-sum test. VAS was represented by median and analyzed by non-parametric test. Comparison between groups was analyzed by a rank-sum test and a U test. VAS changes in each group used a paired sample t-test. P<0.05 was considered statistically significant.
All statistical analyses were performed using SPSS software (V.22.0).
Results
Thirty-four patients completed the project. No statistically significant difference was found between the groups in terms of the sex distribution (p=0.730) or the average age (p=0.892). In this study, we just calculated the surgical time excluding the local anesthesia time. There was a statistically significant difference in mean surgical time between laser surgery (mean=224±59 s) and scalpel surgery (mean=740±168 s) (p<0.001) (table 1).
According to VAS scores of the intraoperative period, 3 hours after the operation and 1st postoperative day of pain, chewing and speaking scores were statistically higher in group B than those in group A. However, we got the same result in the 7th postoperative day in terms of pain, but no significant difference in speaking and chewing (table 2). At the same time, VAS scores of each group were statistically different between intraoperative and 3-hour postoperative period (table 3).
Comparison of VAS scores between two groups
Comparison of VAS scores’ intergroup of pain, respectively, intraoperative period and 3 hours after the operation
After 1 month, all of the patient results were recorded, including the healing of wound and scar. Except for one patient in group B who had a scar, all patients achieved good results.
Discussions
The goal of this study (to compare the advantages and disadvantages of laser and the scalpel surgical methods for frenectomy) was accomplished. Group A’s (laser group) surgical time was markedly shorter (excluding the application of local anesthesia). Because of the suture, group B’s (scalpel group) surgical time was substantially longer (the average time of group B’s procedure was 752.12 s, three times longer than the laser group). Similar results had already been obtained by Sarmadi et al,14 and meta-analysis by Protásio et al15 predicted we would get the same result. The laser frenectomy procedure was not only shorter by about 4 min, but it also resulted in other advantages (such as increased cooperation by patients, less interoperative pain, less postoperative discomfort in speaking and chewing). In terms of the scalpel surgery, the sutures were scissored on the 7th postoperative day.
In contrast with all other studies, this study combined Er:YAG and Nd:YAG lasers because of their separate traits. Er:YAG is highly efficient in the incision of soft tissue. It has a wavelength of 2940 nm, permitting shallow penetration and a high water absorption rate. This kind of laser can be strongly absorbed by the water molecules in the irradiated area, producing the photoelectric solution effect to make the water temperature rise sharply. The steam pressure is released from the tissue molecules to produce a small explosion which negates the result of the rising temperature. In short, the heat will not cause the soft tissue to burn and affect tissue healing, primarily because the water will counteract the effect of the heat. But we also observed that the wound did not stop bleeding quickly. In contrast, Nd:YAG laser has a wavelength of 1064 nm, so that soft tissue dissection is inefficient but rarely leads to bleeding. The high tissue penetration and hemoglobin absorption reduce bacterial populations by heating, resulting in local disinfection, which aids in wound healing and reduces the use of antibiotics. We used the mode of VLP, power 4 W to electrocoagulation and use the mode of low-level laser therapy (LLLT), MSP, power 1.5 W, to prevent oral aphthous ulcers, and analgesic and wound healing effects. Low-energy laser can effectively relieve the pain of ulcers and accelerate wound healing. All of these methods could cut the frenulum precisely and accelerate the healing of the wound.16 After local anesthesia, we made certain children’s FBRS could get to three or four level despite the different surgical methods. In this way, we could assure a smooth operation. In terms of conventional frenectomy, scalpel was the first choice and was easy to operate. However, open wounds lead to bleeding and hematomas that interfere with healing, which can lead to speech and chewing discomfort. At the end of the scalpel surgeries, we used suture to hemostasis. Most of these cases required three to five sutures, which cost more time to complete the surgery. However, the sutures would be hard to clean up, which caused more plaque to build up. These led to more discomfort speaking and chewing in the 1st and 7th postoperative days. On the other hand, one benefit of using laser was a reduction of postoperative inflammation because sutures were not required.17 Although many kinds of lasers have been individually employed in frenectomy surgery, we combined the advantages of the Nd:YAG and Er:YAG lasers. Er:YAG has the ability to disinfect the surgical site while cutting it accurately, while Nd:YAG can promote tissue healing and blood coagulation, sterilization and disinfection. Finally, the mode of LLLT can effectively relieve ulcer pain and speed up wound healing. The combined advantages of these lasers reduce intraoperative bleeding and accelerate the rate of postoperative wound recovery. Our results clearly showed VAS in the laser group resulted in a statistically significant difference after 3 hours, which was corroborated by other studies.18–20 VAS scores (pain, speaking, and chewing) of the laser treatment on the day of the operation and on the postoperative 1st day were statistically lower and were consistent with the reduction in pain perception during the procedure and the 7-day postoperative period21 compared with those of the scalpel surgery.
At the same time, the depth of incision during the operation for the scalpel group is difficult to calculate precisely. The wound at the suture site may lead to the accumulation of plaque, and the postoperative swelling may aggravate the lip movement limitation and the possibility of aggravating scar formation. Erbium laser does not need suture and has the function of hemostasis and sterilization. It can reduce the postoperative swelling, shorten the operation time, and avoid the trouble of suture removal and the fear and discomfort of suture removal in patients’ second visits.
During the whole treatment, each group had prominent progress in pain between intraoperation and 3 hours after labial frenectomy surgery by using VAS. After the disappearance of anesthesia, postoperative swelling and pain relative to intraoperative discomfort improved in both groups.
Other relevant studies showed that CO2 laser provided for bloodless fields and shorter surgical times but slower wound healing compared with the Er and Cr:YSGG (Chromium∶ Yttrium-Scandium-Gallium-Garnet).22 At the same time, a more uncomfortable sensation of both operative time and pain perception is exhibited with the CO2 laser.23 We need more data to describe the advantages and disadvantages of different lasers in subsequent studies.
However, some other studies manifested no number of analgesics used19 and suggested that wound healing took place more quickly with less scar tissue in laser technique than scalpel technique.24 In the present study, we used the same injection with the same model and same dosage. In future studies, we will add up another group to test the balance of the medical comfort level. Compared with the occurrence of the scar issue, damage caused by lasers to the soft tissue is minimal. At high temperature, blood vessels shrinking gave rise to photothermal coagulation.
Limitations
The small number of participants is an inherent limitation; however, the resulting differences between the two groups can be ascribed to the different methods of treatment, which fulfill the purpose of the current study, with additional investigations needed to be conducted in the future.
In conclusion, the abnormality of the labial frenulum is closely related to the space between maxillary central incisors. Taking into account the time of treatment for children, intraoperative pain, postoperative pain, speech, chewing and other factors, the effect of the combined treatment of bait and neodymium laser is far better than the scalpel treatment. Frenectomy performed using the dual-wavelength laser in pediatric patients is a useful, effective, comfortable and safe treatment method, but it also needs to be based on the clinical symptoms. Choice of the method depends on effectiveness, acceptability and security. However, it is very important to estimate the relative factors, such as equipment cost, to determine which is the optimal choice.
Above all, two-waved laser may be a new choice in frenectomy surgery as it leads to a marked improvement between intraoperative and postoperative pain.
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of Hefei Stomatological Hospital (project no. YW2019015). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
I would like to express my gratitude to all those who helped me during the writing of this thesis. I gratefully acknowledge the help of my coworker, Mr Zhang Liang, who has offered me valuable suggestions in the academic studies. In the preparation of the thesis, he has spent much time reading through each draft and provided me with inspiring advice. Without his patient instruction, insightful criticism and expert guidance, the completion of this thesis would not have been possible. I also owe a special debt of gratitude to all the professors in Hefei Stomatological Hospital, whose devoted clinical teaching and studying have benefited me a lot and academically prepared me for the thesis. I would finally like to express my gratitude to my beloved coworkers of my department who have always been helping me out of difficulties and supporting without a word of complaint.
References
Footnotes
Contributors LX conceived conceptualization, completed investigation, led the writing – review & editing. PW contributed to data curation. YD took visualization. LZ contributed to formal analysis. All authors read and approved the final manuscript. LX is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.