Article Text

Statistics from Altmetric.com
Omphaloceles occur in about 1 in 5000 births and are the second most common congenital abdominal wall defects.1 Repair remains a surgeon’s preference with early closure only attempted for small-to-medium omphaloceles, while delayed closure is used for giant omphaloceles.2–4 In recent years, novel techniques that aim at reducing the disproportion between the abdominal cavity and the volume of the extra-abdominal viscera have been described to manage giant omphaloceles.4–17
Although less commonly associated with genetic abnormalities, giant omphaloceles are associated with adverse neurodevelopmental outcome at 2 years.18 In addition to gestational age, birth weight, associated malformation, resuscitation and hypoxia, other factors including prolonged stay in the neonatal intensive care unit (NICU), time on ventilation, infections, and delayed establishment of enteral nutrition are likely contributory factors.19
This is a case study of two infants with giant omphaloceles treated in our institution with a novel neoprene binder preoperatively. The binder allows for gradual reduction of the viscera below the level of the skin followed by early fascia closure. Families were contacted for a follow-up survey about parental experience and satisfaction in March–July 2020. A summary of the demographic and outcomes is reported in table 1.
Summary of patient’s demographic and outcomes
Both infants had giant omphaloceles2 3 larger than 5 cm with most of the liver and bowel in the sac. Neither had other major abnormalities nor genetic disorders. After delivery, infants were wrapped in a plastic bag to protect the omphalocele sac and were transferred to NICU for initial care. Infants did not require sedation or intubation, and enteral feeds were started on day 1 of life, with 5 and 11 days, respectively, of concomitant parenteral nutrition until full enteral feeds were established. Immediately postnatally, the intact sac was cleaned and dressed with Restore silver dressing and was wrapped with kling gauze. The neoprene silo binders were custom built by our NICU occupational therapists (guide in online supplemental appendix 1) and were customized based on omphalocele, abdominal opening and baby sizes (figure 1, online supplemental table 1, online supplemental figures 1–6). Compression began on the first day of life. All the changes to compression were done with the infant awake—no sedation, paralysis or analgesic other than occasional sugar water was used (online supplemental figure 1). Parents were able to hold their babies from day 2 of life.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
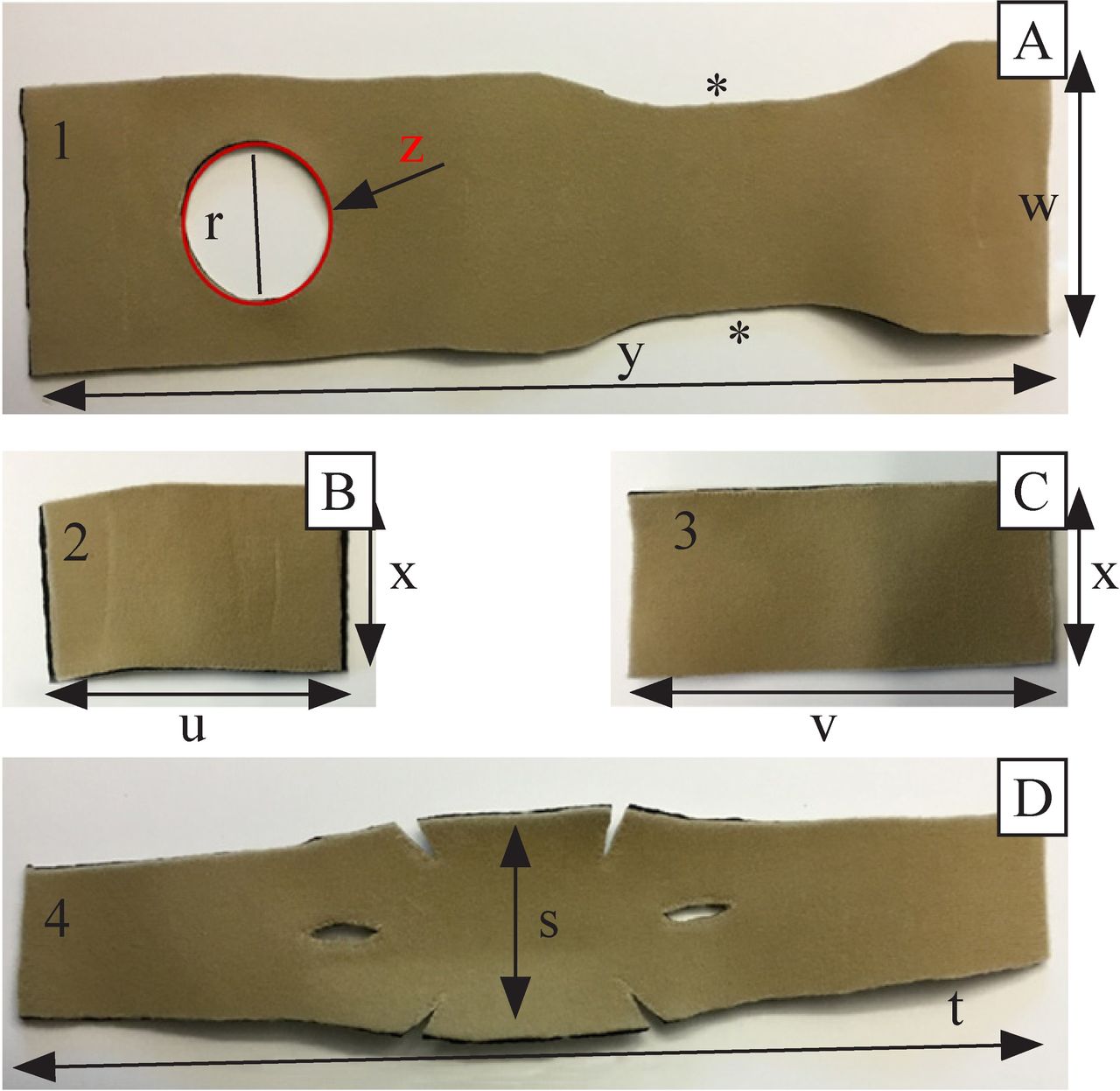
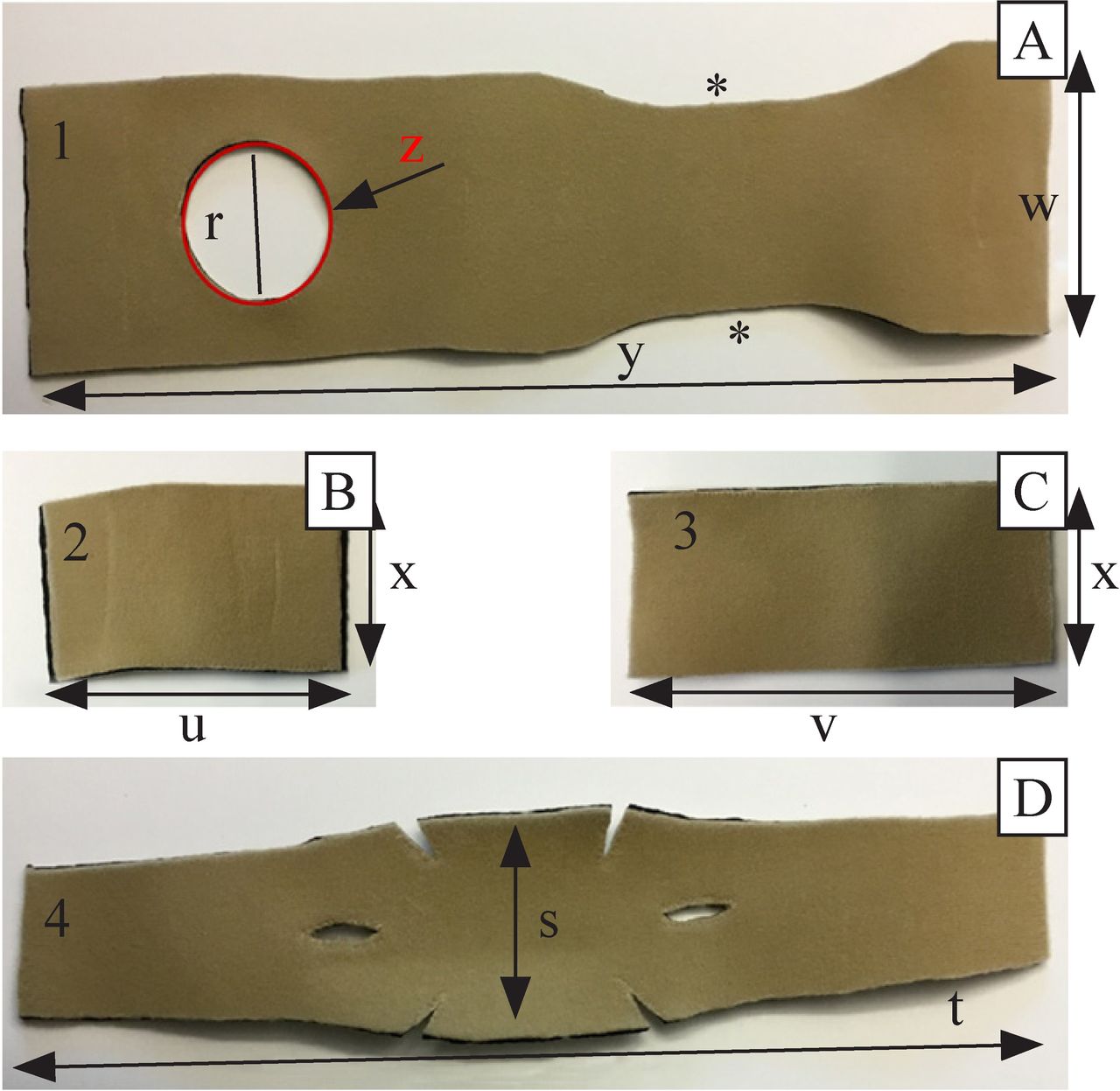
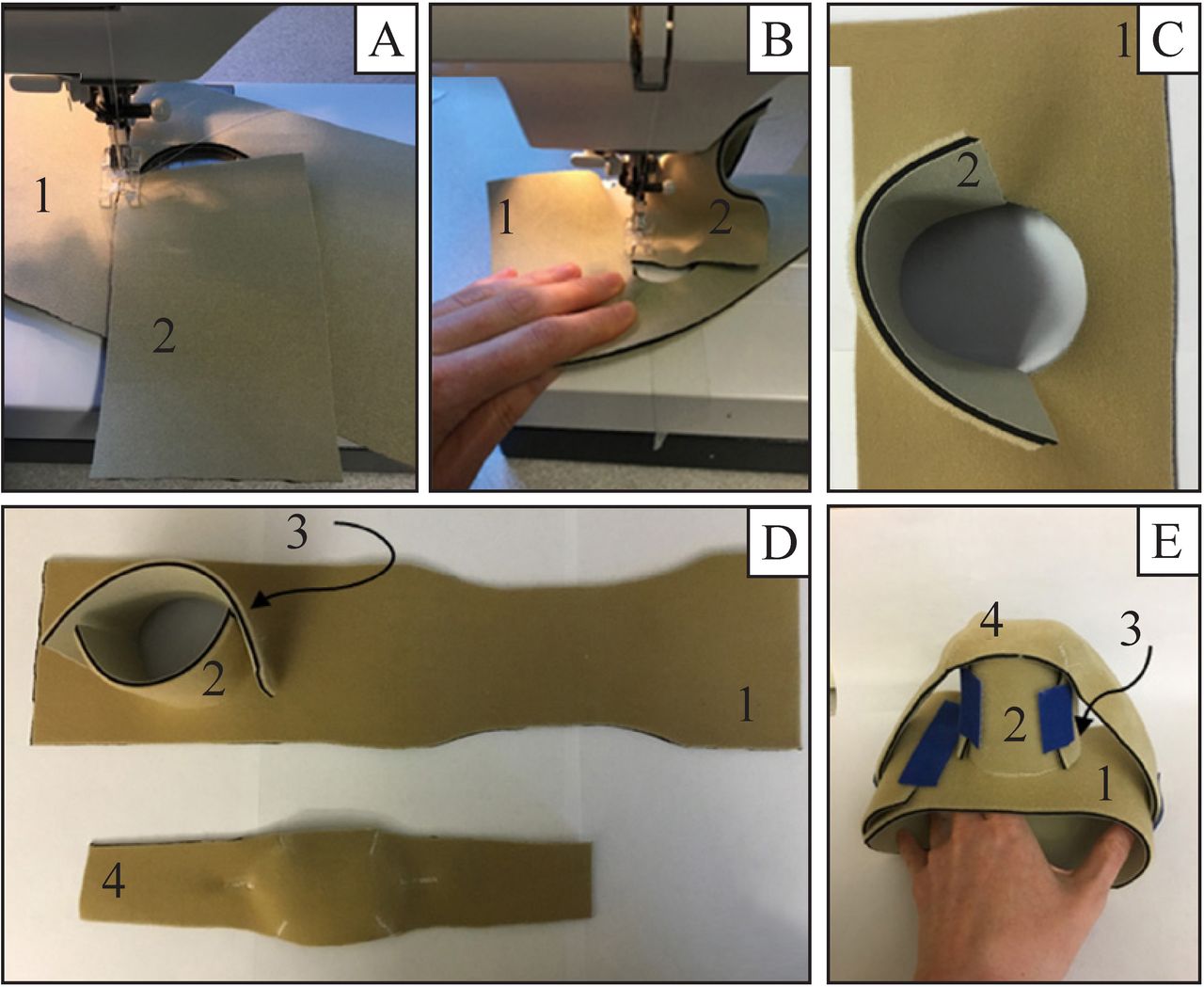
Components of the omphalocele binder. (A) Torso wrap with hole cut to fit over omphalocele. (B,C) These two parts will make the silo to support the omphalocele. (D) The compression strap that will fit over the top of the silo. Please refer to guide in online supplemental appendix 1 for all the details and how to measure infants to make a binder to fit each infant. Asterisks indicate the area narrowed to accommodate the shoulder blades. r, diameter of whole in torso wrap; s, width of compression band (piece 4)=20% wider than the diameter of the hole in the torso wrap r; t, length of the compression band (piece 4)=4.5 times the height of the omphalocele (x); u, length of piece 2 equivalent to half the circumference of the neck of the omphalocele; v, length of piece 3 which is 20%–30% longer than piece 2; w, torso length; x, the height of the omphalocele when the peritoneal sac is gently contained to extend upright within the circumference of the abdominal wall defect from base to top; y, the circumference of the infant’s torso plus 10%–15% for overlap and growth; z, the circumference of the abdominal wall defect.
The binder includes three components (figure 1 and online supplemental figures 1–3). The first component (piece 1) is a full torso wrap with Velcro closure and a hole cut to the circumference of the omphalocele. The second component is a neoprene silo attached to the torso wrap (pieces 2+3). The height of this silo starts 1–2 cm below the total height of the dressed and contained omphalocele. During application, care is made to prevent a ‘mushrooming’ effect of the omphalocele over the top of the silo to prevent the defect from getting wider. The third component (piece 4) is a compression strap that is placed over top of the silo with wide straps extending down to the torso wrap (figures 2 and 3A,B). Suspended external devices were not necessary because the neoprene offers enough rigidity to hold the silo upright. Minor readjustments—tightening of the compression and silo circumference straps, as well as adding gauze inside the silo to aid in downward compression (figure 3C)—were made once or twice per day. Restore silver dressing was used daily on non-epithelialized areas until skin was full epithelialized and then was discontinued. Infant response was assessed clinically without invasive monitoring. When the omphalocele was close to the level of the abdominal wall, a foam disk ‘plunger’ (figure 3D) was added inside the silo under the compression strap, this allowed compression while at the same time preventing ‘mushrooming’. This ‘plunger’ provided sufficient compression to invert the omphalocele in preparation for surgery (figure 3D). As the omphalocele decreased in size and the infant became more active, straps over the shoulders and the diaper were used to keep compression centered over the abdominal opening (figure 3B and online supplemental figure 6). Major readjustments were made every 2–4 days by cutting down the silos’ height and by adjusting the torso wrap and the compression strap for the changing shape of the omphalocele. A key feature of our technique is that it allows the liver and hepatic vessels to move back into the abdominal cavity gradually, as the abdominal space naturally increases, reducing the risk of hepatic vessels kinking and reducing the potential damage to the liver. In addition, our infants remained stable from a cardiorespiratory point of view, did not develop pulmonary hypertension, and did not require any respiratory support. Figure 4 shows a progression of the omphalocele reduction in the abdominal cavity.

Assembly of the omphalocele binder. (A,B) Depict use of a standard sewing machine to sew flat edges of the silo piece (2) to the hole in the torso wrap (1) using zigzag stitch, piece 3 is sewn in a similar manner; (C) depicts the beveled edge cut into the inner component of the silo to reduce pressure ridges; (D) depicts the three-dimensional shapes created by these flat zigzag stitched seams for both the silo and the compression band. Note that the torso wrap has been cut to have reduced width around the shoulder blade. (E) Shows the assembled binder with Velcro closures that can be used to increase or decrease compression of the omphalocele to support gradual reduction into the abdominal cavity.
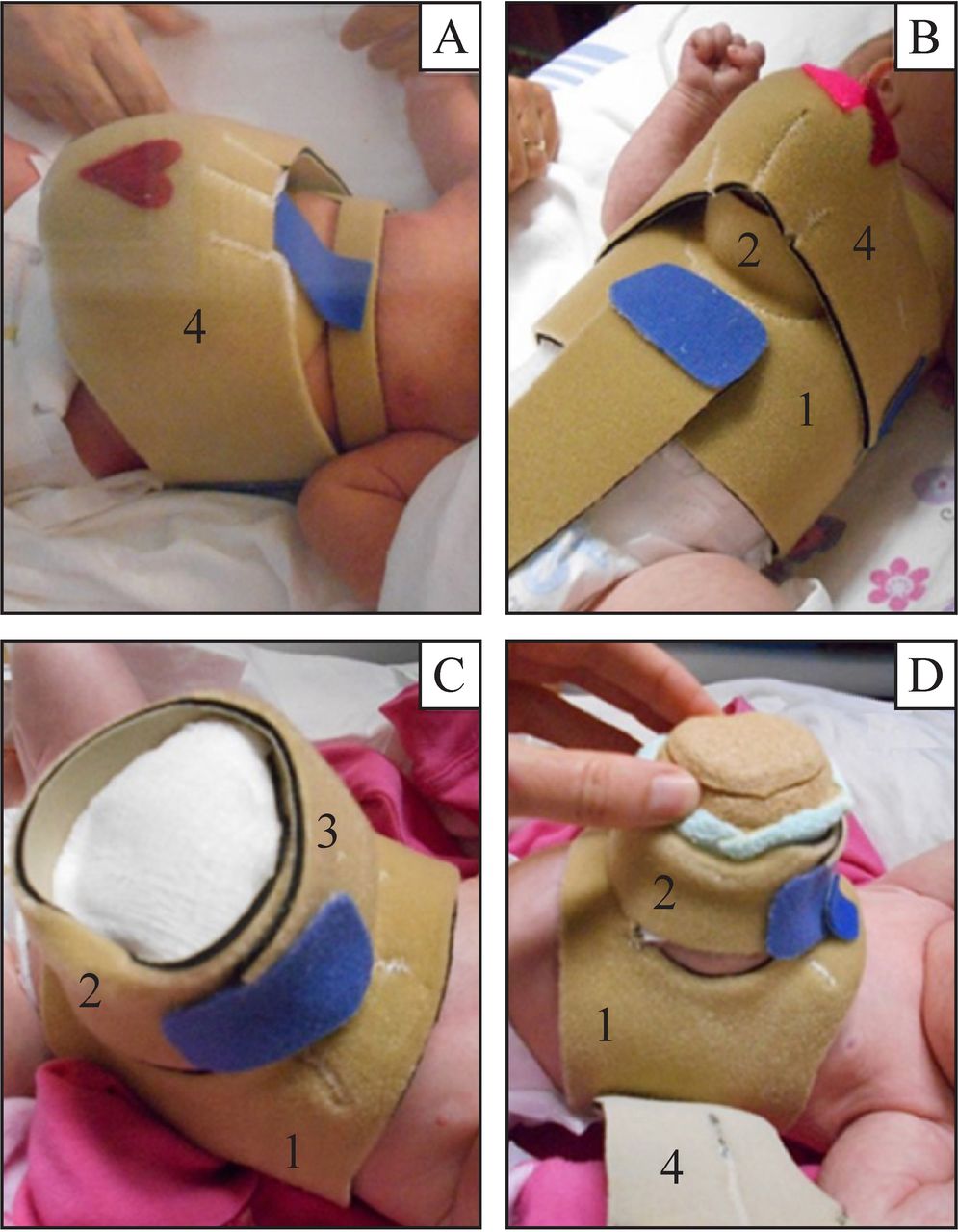
Neoprene omphalocele binder in use. (A) Early days of wearing the binder. (B) Strap added over diaper (and shoulders) to hold the torso wrap in place and maintain omphalocele over top of the abdominal opening. (C) The silo has been cut down significantly from the initial version and gauze has aided in the compression of the omphalocele within the silo. (D) A foam plunger used inside the silo increases the downward compression of the omphalocele contents to take advantage of the increased intra-abdominal space. 1, torso wrap; 2 and 3, silo components; 4, compression strap.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
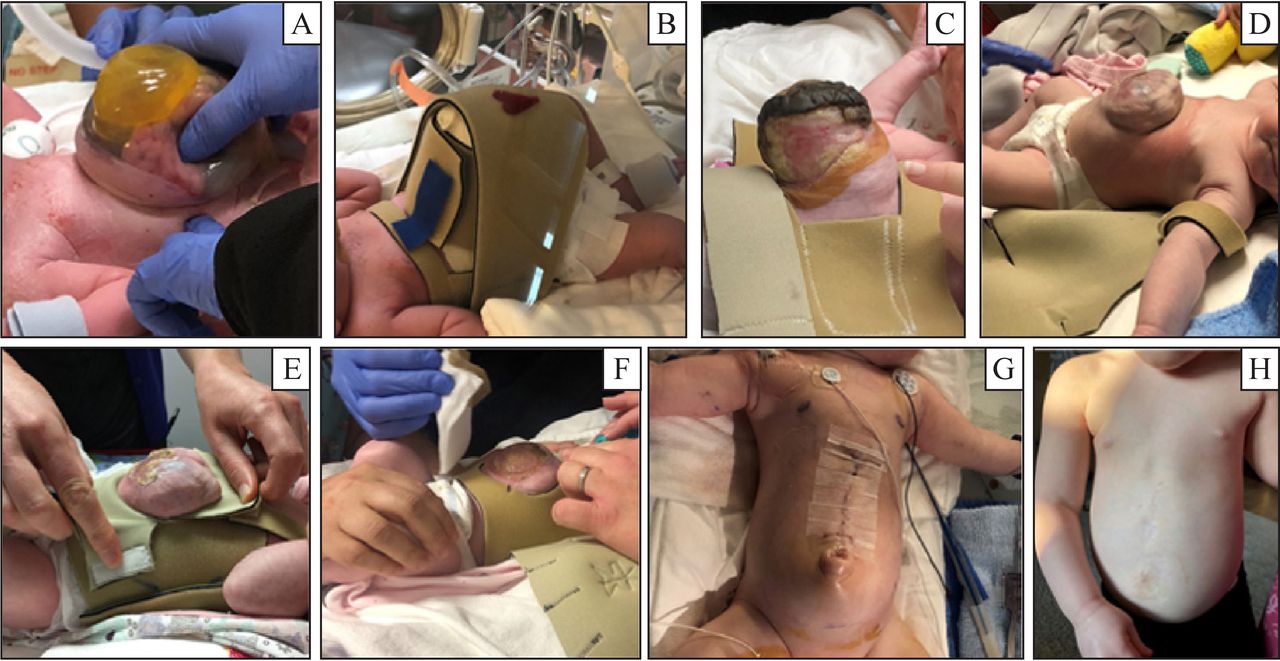
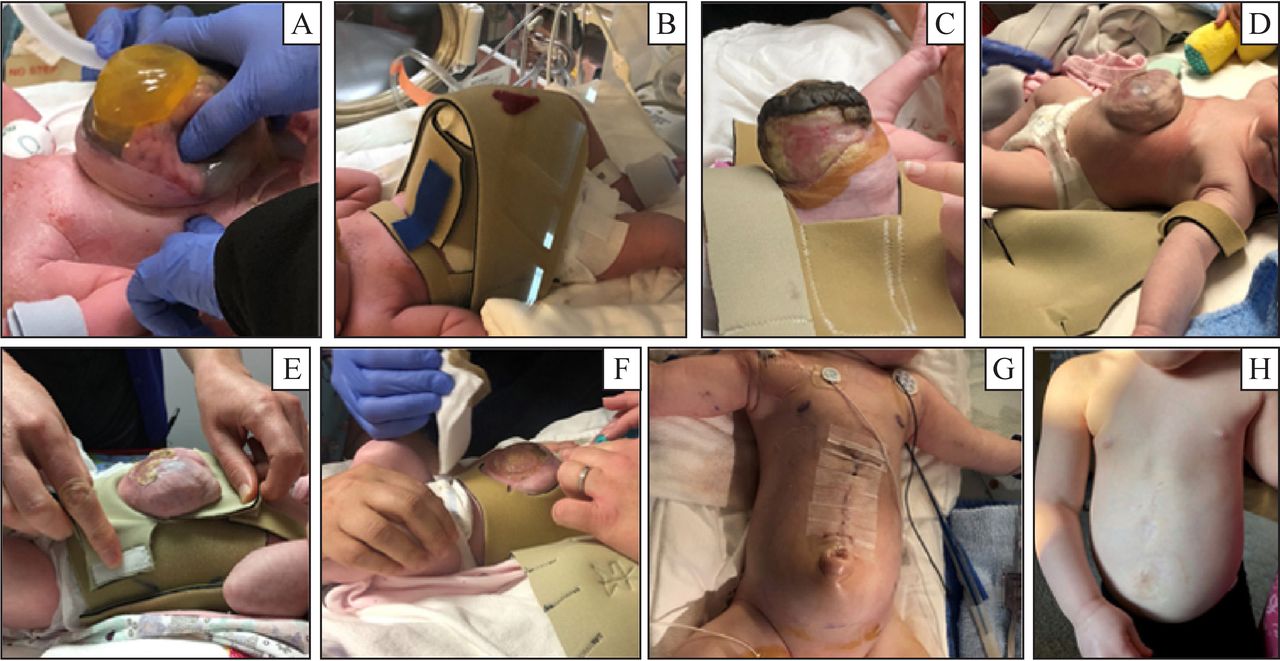
Progression of omphalocele reduction. (A) Immediately postnatally; (B) Initial binder; (C–F) Progressive reduction of omphaloceles; (G) Immediately postoperatively; (H) Child at age 4.
When the abdominal content was completely reduced below the fascia, the babies were brought to the operating room for primary surgical repair. At the time of surgery, both babies had fully reducible omphaloceles with enough growth of fascia and skin to allow primary closure without the need of a patch. One child had enough excess skin available to create a pseudo umbilicus (figure 4). Both patients had closure of the muscle layers at the time of surgery. Airway pressures, urine output and lower limb perfusion were monitored throughout the surgical procedure for respiratory compromise and abdominal compartment symptom.
Babies were extubated in the operating room and were brought back to NICU for postoperative care. This included wound and pain management and resumption of enteral feeds when bowel sounds were present. During the postoperative period, infants were awake, they did not require muscle relaxant or any invasive monitoring. Time to surgery was 47 days (baby 1) and 102 days (baby 2), and both infants were discharged 12 days postoperatively.
Neither patients had further surgical needs, hospital readmission or complications from surgery in the first 2 and 4 years of life, respectively. Overall complications included skin breakdown, suture reaction, and small abscesses post-surgery that did not require antibiotics.
A follow-up survey (online supplemental appendix 2) was sent to parents to assess parental satisfaction and their expectations preoperatively and postoperatively. Caregivers had incredibly positive views of the binder, the surgery, and the outcome (table 2). Neither babies had any developmental issues at age 2 and 4 years, respectively.
Supplemental material
Summary of results from parent’s survey
Techniques that use compression to reduce omphaloceles within the abdominal cavity prior to surgery aim at increasing available skin and fascia to obtain primary closure, ideally without the use of a patch.4–16 In addition to those aims, our goals also included avoiding repeat surgeries, reducing developing brain’s exposure to sedative and analgesic medications, early enteral feeds, and allowing for normal infant neurodevelopment. Our technique is easy to reproduce and customize with low-cost neoprene and a sewing machine. The binder is easily applied, adjusted and removed, reducing the risk of increased intrathoracic pressure, pulmonary hypertension, compression of vena cava, limb ischemia, respiratory distress, and skin break down. Children were awake, not paralyzed, and were able to do early tummy time. Early enteral feeds were achieved, which removed the need for long-term intravenous access. No pain was associated with the application of the binder, and there were minimal nursing concerns. Our survey showed that both families had negative expectation of outcome when the diagnosis of omphalocele was made prenatally, but are currently doing well, with minimal impact to the child and are developmentally on par with children of similar age.
One consideration with our technique is the need for hospitalization until time of surgery. Given that the omphalocele is not reduced in the abdominal cavity immediately, we felt it was safer for the children to remain in hospital for monitoring. Infants had early transfers to our level II NICU and only require 2–3 days of admission in level III NICU—immediately postnatally and immediately post-surgically. Infants have not required any other time in hospital since the time of discharge. In addition, families have not required other interventions (occupational therapy, physiotherapy, education support, etc) which, in the lifetime of the child, would reduce the burden to the healthcare system, the insurance companies or the family in a privately paying system.
It is evident that many surgical groups around the world have noted the value of reducing the size of omphalocele prior to surgery, and others have used a neoprene binder in gynecological surgeries with positive outcomes.20 We believe that broad adoption of a neoprene binder can increase the success of the repair and can improve developmental outcome of children with giant omphaloceles.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. All relevant data are available in the manuscript. A detailed guide on how to build the neoprene silos has been added as supplemental material in the hope of disseminating the information widely and allowing other surgical team to easily reproduce it.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Health Research Ethics Board (HREB) (study # H2019-076) for the retrospective study and the qualitative study of parent’s satisfaction level.
Acknowledgments
Thank you to the families who participated in our study. We would also like to thank Dr Scott Cameron for critical appraisal of our manuscripts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BL-G contributed to conceptualization, formal analysis, visualization, investigation, writing original draft and guarantor. LC contributed to visualization and writing original draft. JK contributed to conceptualization and writing review and editing. NY contributed to conceptualization and writing review and editing. SC contributed to writing review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.