Article Text

Abstract
Background Monteggia equivalent lesion represents a group of injury or combined injury patterns that resemble the Monteggia lesion in its presentations and mechanisms. Unlike Monteggia lesions, the equivalent ones, which share vague definitions and mostly occur as sporadic single case reports in the literature, have not been thoroughly reviewed since Bado first proposed the term, especially in the pediatric population. The objective of this review was to elucidate the definition by elaborating on its clinical styles and thus analyzing the mechanism, diagnosis, and management through related literature.
Data sources Based on the terms of ‘Monteggia equivalent’, ‘radial neck fracture’ and ‘pediatric’, all of the related literature was searched on the PubMed and Google Scholar search engine.
Results The advance of the definitions for pediatric Monteggia equivalent lesion (PMEL) was reviewed. The functional roles of the ulnar and the related mechanism theories in this injury were analyzed. The status of the radiocapitellar joint in this injury was emphasized. According to the previous statements, a new classification model was proposed and proper diagnosis and treatment approaches were suggested.
Conclusions PMEL should be defined as an ulnar fracture at any level combined with a proximal radial fracture. According to the status of the radiocapitellar joint, it could be divided into three groups. The occult ulnar bowing and delayed radial head dislocation should be a serious concern of orthopedists. Surgical need is usually warranted. Maintaining the ulnar length and securing the radiocapitellar joint are highly recommended.
- orthopedics
- pediatrics
Data availability statement
Data are available in a public, open access repository. As a review article, the data is acquired from the previously published works.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Monteggia fracture, named after Giovanni Monteggia in the 19th century and well described and classified by Dr Bado decades ago, involves ulnar fracture and concomitant dislocation of the radial head. The term ‘lesion’ has gradually superseded those such as ‘fracture’, ‘fracture–dislocation’, or ‘injury’ in the literature, stressing the importance of noticing the radiocapitellar joint and reflecting an increased awareness of the complexity regarding its manifestation and mechanism among orthopedists.
Apart from the established four types proposed by Bado, the groups of ‘Monteggia equivalent lesion/variant’ have been considerably expanded during decades of sporadic case reports. The boundary of that definition has largely been blurred. Also, especially in pediatric patients when immature radiocapitellar epiphysis interferes with judgment and flexible joint allows more frequent subluxation, quite a number of these types tend to be misdiagnosed or neglected owing to the occult presentation of radiocapitellar joint or plastic bowing ulna on radiographs. Yet, throughout these decades, literature has been disproportionally scarce on reviewing this subset of the entity.
The aim of this narrative review was to enumerate the extended cases for this lesion and to achieve a reasonable academic consensus on the definition. Pediatric orthopedists’ additional awareness of this variant is expected to develop. We hope that greater understanding and management of the Monteggia equivalent lesion in children are facilitated by this review.
Definition
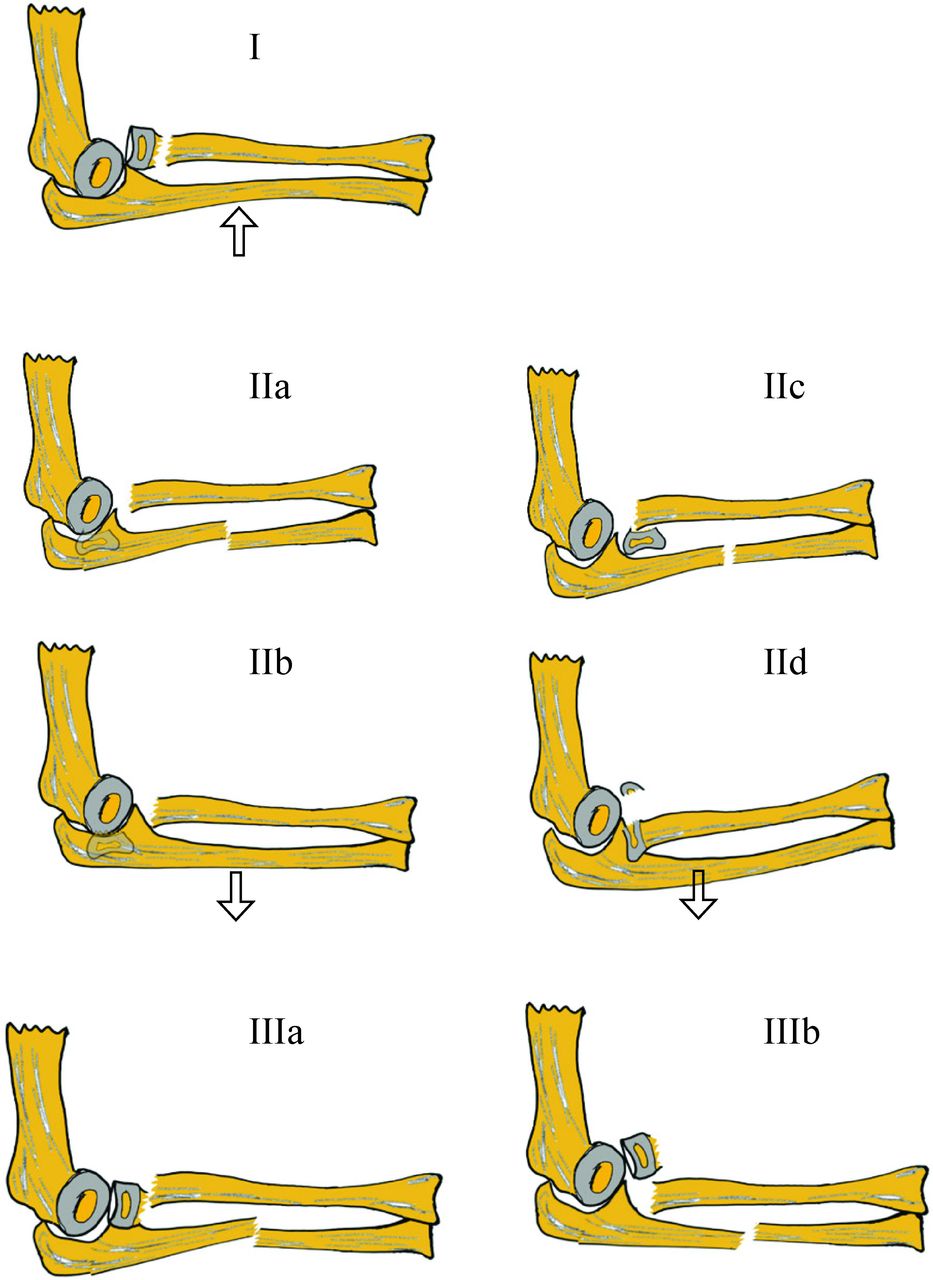
The term ‘Monteggia equivalent lesion’ was first proposed by Jose Luis Bado in his seminal article published in 1967.1 In addition to the established four types, he classified a group of lesions that shared a similar mechanism yet presented heterogeneous manifestations with those of ‘Monteggia lesion’. Five groups of type I equivalents were described: (Ia) anterior dislocation of the radial head (without obvious ulnar fracture, probably could not be detected due to then examination restriction); this group also includes the ‘pulled elbow syndrome’ in the child; (Ib) fracture of the ulnar diaphysis with fracture of the neck of the radius; (Ic) fracture of the neck of the radius; (Id) fracture of the ulnar diaphysis with fracture of the proximal third of the radius; and (Ie) fracture of the ulnar diaphysis with anterior dislocation of the radial head and fracture of the olecranon (figure 1). He categorized some kinds of epiphysial or radial neck fracture into type II equivalent. As shown in figure 1, type Ib–Id and type II equivalents did not specifically involve the status of the radiocapitellar joint, which was contrary to those type I–IV lesions that each combined with a dislocated radial head. Besides, he did not mention any of the type III and IV equivalents (figure 1).

Evolution for the definition of pediatric Monteggia equivalent lesion. Bado’s classification: five types were mentioned. Note the anterior dislocation of the radiocapitellar joint in types Ia and Ie. Lett’s type A–C depicted anterior bowing of ulna. Wiley’s I–III described anterior, posterior and lateral dislocation of the radiocapitellar joint, each combined with an olecranon fracture. More universal definition from Olney and Čepelík. Question marks indicate the undescribed status of radiocapitellar joint in subtypes Ib–Id. Arrows show the associated anterior dislocation of the radiocapitellar joint. Hollow arrows show the proximal radial fracture combined with proximal, middle or distal third fractures of the ulna.
Subsequent studies had been more willing to fill that categorical vacancy. Following the logic of Bado classification for Monteggia equivalent lesion, Ravessoud2 put a pediatric case of lateral condylar fracture and ipsilateral ulnar shaft fracture into type III equivalent, while another author categorized an adolescent case of radiocapitellar dislocation and concomitant fracture of the supracondylar humerus and distal radius as type IV equivalent.3
The concept of ‘equivalent’ for the pediatric population continued to evolve as further elucidation came from two study groups separately in the same year, 1985. Letts and his colleagues4 stressed the importance of noticing the anterior bend or greenstick of immature ulnar and subsequently dislocated or subluxation of the radiocapitellar joint in pediatric Monteggia lesion. They took these occasions into the expanded equivalent lesions. Wiley and Galey5 placed specific concern on the olecranon and proximal ulnar fracture-related radiocapitellar joint issues. They suggested including those three scenarios into type I–III pediatric Monteggia equivalent lesions (PMELs), respectively. That proposition conflicted with the former opinion, which specifically excluded the olecranon-involved type out of the category of Monteggia lesion.6
Olney and Menelaus’s7 102 case studies on PMEL in 1989 offered a periodical review for Monteggia equivalent lesion in children. Out of 102 cases in that study, 17 were deemed as the equivalent. Aside from two cases of radiocapitellar dislocation with bowing ulna and one with concomitant olecranon and ulnar shaft fracture, 14 of them, with concomitant fracture of the ulnar shaft and radial head/neck, were ranked as the third most common in their series, second only to true Monteggia lesion of Bado types I and III.
The discussion has never stopped over ‘the equivalent’ as to its presentation, injury combination, mechanism, diagnosis, and management in the past several decades when a few sporadic case reports demonstrated some of the unclassifiable ‘equivalent’.8–20
A most recent contribution towards the definition has been made by Čepelík et al21 and his group in their study of 111 cases. They defined it as an ulnar fracture at any level combined with ‘displaced’ (with undisplaced or minimal displaced ones were not included) proximal radial fracture, which embraced Olney criteria and was consistent with Bado Ia–Ic. Those with the radiocapitellar dislocation or subluxation induced by ulnar bowing or incomplete fracture (Lett I and II) and by olecranon fracture (Wiley I–III) were included into ‘true’ Bado type I–III counterparts, respectively, and thus were excluded from the equivalent lesion. This is a big advance for the currently highly heterogeneous definition of PMEL. Yet, though this definition, like the Olney one, brought forward the association of proximal radial fracture in PMEL, they both failed to further specify it. As previous case studies have shown, the proximal radial fracture, involving the region of the radial head, neck, and especially the radiocapitellar joint presented extremely complicated attributes, thus justified a more elaborated classification on it for the PMEL (figure 1).
Thus, based on Olney’s and Čepelík’s definitions, and taking various elaborations of the lesion type in the proximal radius region into account, we could try to sort out a currently reasonable subcategorization strategy for PMEL mostly according to the status of radiocapitellar joint (figure 2).
Proposed classification based on Olney and Čepelík. Group I: anterior ulnar plastic deformity combined with radial neck fracture and anterior radiocapitellar joint dislocation. Arrow shows the anterior bowing. Group II: ulnar fracture associated with posterior radial neck fracture and posterior radiocapitellar joint dislocation. Four subtypes were observed in the literature cases. Group III: ulnar shaft fracture associated with a radial neck fracture, the most frequently seen subtype. Arrows indicate posterior bowing.
Presentation
Historical case reports on PMELs are listed in the four tables as follows. All but two of these specific cases fit Čepelík’s definition of ‘displaced proximal radial fracture and concomitant ulnar fracture at any level’. The 14 cases were roughly divided into four groups according to the migration direction of the radial head or the main part of the radial head relative to the capitellum. Only two cases8 9 in the literature were sorted into group I and identified as with anterior dislocation of the radiocapitellar joint. Both were late present or neglected cases with occult ulnar fracture (table 1). Four with posterior dislocation of the radial head were sorted into group II, among which two with undiscovered posterior bowing of ulna underwent an unpleasant prolonged treating process and one with radial head fracture (Salter-Harris IV) was the only one in this series (table 2). Intact radiocapitellar joint occurred in six cases, which constituted group III and was also the only described type in Olney’s or Čepelík’s series (table 3). The other two cases, with either a fracture of humerus or distal third radius, were not combined with a radial neck or head fracture and thus did not affiliate to Čepelík’s definition. They were suggested to be classified as true Monteggia fractures in this review (table 4).
Analysis of reports on pediatric Monteggia equivalent lesion (group I)
Analysis of reports on pediatric Monteggia equivalent lesion (group II)
Analysis of reports on pediatric Monteggia equivalent lesion (group III)
Analysis of reports on pediatric Monteggia equivalent lesion (group 4)
Proximal radius and radiocapitellar joint
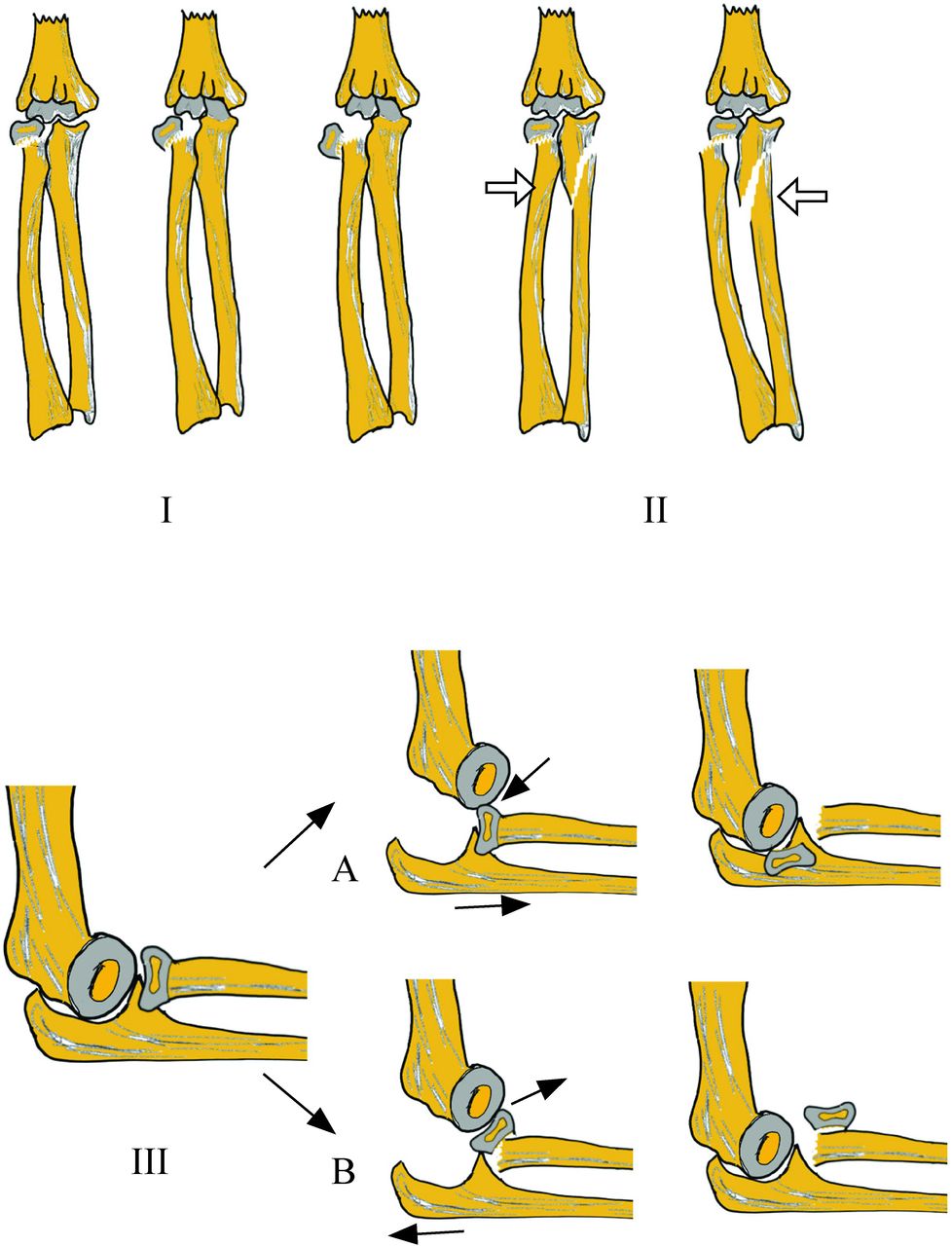
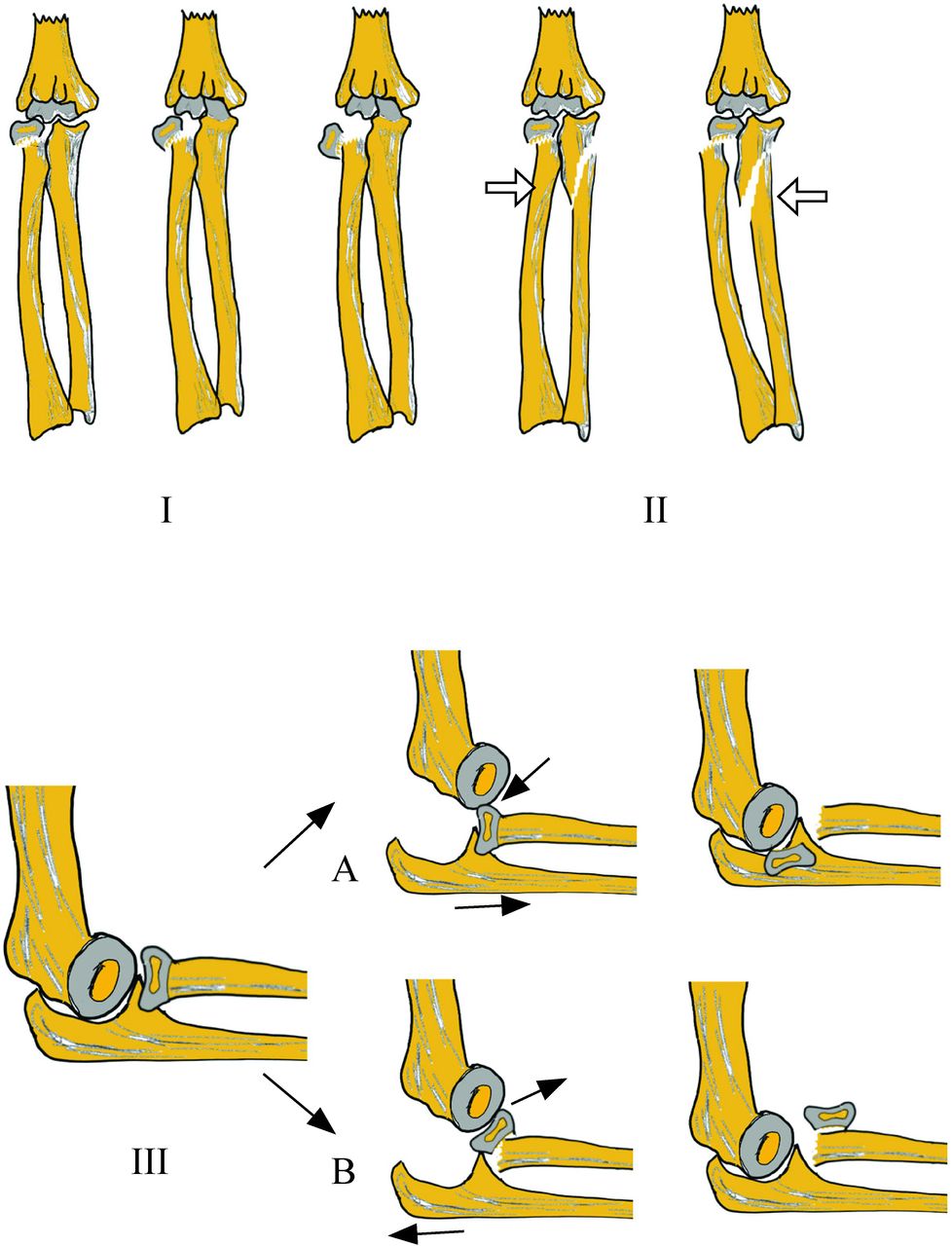
The involvement of the proximal radius in the PMEL brought up its entanglement with the definition of the isolated pediatric radial neck and head fracture. The rarely used Chamber22 classification for pediatric radial neck fracture (PRNF) ascribed its group II injuries, that is, those with primary displacement of radial neck (and largely intact radial head and radiocapitellar joint), to Monteggia equivalent lesions, the group III in our review (figure 2). And the Chamber group I was compatible with currently prevailing classifications of Judet23 and O’Brien,24 which were mostly based on Jeffery’s25 in 1950, grading the severity according to the lateral angulation and displacement of the radial head (figure 3). This pattern of radial neck fracture might lead to gradual angulation deformity of the radial head and to subsequent incongruity of radiocapitellar joint and played a role in some of the delayed PMEL, like the two cases of group I in the first table (table 1). Additional patterns of PRNFs, described by Jeffery and subsequent authors,26–29 were also found in group II (table 2) of this review, where momentary partial elbow dislocation and relocation caused the displacement of the radial head. Combined with ulnar posteriorly bowing, it generated two late presented PMELs, prolonging the treating process (figure 3).
{kind=link}
{kind=link}
{kind=link}
Various categorizations for proximal radial fracture. I: prevailing classification of Jeffery, Judet or O’Brien on lateral displacement and angulation of the radial head. II: chamber group II, where the radial head stayed in situ; primary displacement is in the radial shaft, found in group III of this review. III: another pattern of the radial neck fracture, involved in the posterior elbow dislocation and reduction mechanism, found in group II of this review. Arrows and hollow arrows show the direction of the force.
The review suggests only a small fraction of radial fracture types that occur in the PMEL could apply the Judet and O’Brien classifications, whereas on most occasions, orthopedists have to resort to the less prevailing Chamber classification to describe those with radial neck and shaft displaced and radial head and radiocapitellar stayed in situ (table 3). Moreover, the classification system this review provided for PMEL has put more concern on radiocapitellar status and covers most PMEL types as recently reported (figure 2).
Ulnar
Both Olney’s and Čepelík’s definitions on PMEL have made it clear that it combined with an ulnar fracture at any level (proximal third, middle shaft, or distal third), of any form (displaced fracture, greenstick fracture, or occult bowing). They did not specify the aspects of the angulation or rotation direction of fracture. Though most of the historical cases were not able to verify the rotation direction or degree, they did note anterior or posterior angulation. In the 12 cases, we recorded nine anterior and three posterior angulations of the ulna. Among them, two anterior angulations8 9 and two posterior angulations11 12 were verified as occult or obscure fracture, the modalities of which were either anterior or posterior chronic bowing of the ulna, in light of the muscular and ligamental linkage, leading to the chronic dislocation of the radiocapitellar joint.
The precise mechanism for PMEL has not been described. The modern consensus is that the PMELs share the similar mechanism with the true Monteggia lesion. However, even for the true Monteggia lesion, a universal mechanism still does not exist. Well-accepted ones are direct trauma, hyperpronation, and hyperextension. The direct blow theory is the most traditional proposed mechanism for true Monteggia lesions. It was first described by Monteggia30 himself and was elaborated well by Speed and Boyd,31 and then was endorsed by Smith.32 It ascribed the dislocation of the radial head to the ‘continued deformation or direct pressure’ of the ulnar fracture, which was caused by direct force on the fracture site. Moreover, this force from continued deformation or direct pressure could also be on the pediatric proximal radial epiphysis transversely. The radial neck might break off before rupture of the annular ligament or lateral elbow capsule, in a skeletal immature system where ligament exceeds bony strength, generating group III of this literature series, the most common PMELs. The hyperpronation theory was suggested by Evans,33 who postulated the rotational force the proximal radius bears to be generated when the forearm is excessively pronated and the radius cross over mid-ulna. However, it was disputed by Tompkins,34 who raised the theory of combined dynamic and static force for the nature of the cadaveric study and the fact that the spiral fracture of ulna resulting from the rotational force was rarely seen clinically. In group I and group II PMELs, the classical mechanism for radial neck fracture might be combined with those proposed for Monteggia. However, more high-level studies are still needed to elucidate the precise mechanism for PMELs.
Other related parts
Previous studies2 3 20 have also recorded Monteggia lesion associated with lateral condyle, supracondylar and medial condyle fracture; the former two were noted as equivalent Bado type III and type IV. Aside from the lesions of the distal humerus, distal radial and ulnar fracture have also been found to be combined with a radial head dislocation19 However, as we put it, we would like to put these combinations to true Monteggia counterparts and stick with the primary definition for PMELs of the presentation of a proximal radial fracture, to elucidate the currently extremely entangled terms.
Diagnosis
Diagnosis for PMELs has always been tricky for the highly heterogeneous presentation, obscure mechanism, and difficulty of discerning the immature radiocapitellar joint and the occult ulnar fracture patterns. Yet, regarding the high risk of misdiagnosis for PMELs and atrocious prognosis for shortened ulna and deformed forearm, and chronically degenerated radiocapitellar joint when subluxation or dislocation of it is unrecognized and untreated, the orthopedists are urgently recommended to acquire proper diagnosis tips.
Physical examinations may reveal non-specific swelling and tenderness of the forearm and elbow, inability to rotate the forearm, flex, and extend the elbow. Considering children’s nature, orthopedists will currently have to rely heavily on imaging measures, traditionally the anteroposterior (AP) and lateral radiographs, to diagnose the PMELs. As the tabled case series shows, the AP and lateral X-rays might not always be accountable initially in discovering a radial neck or head fracture, for the vagary induced by unossified physis8 10 13 or the shading from adjacent bony structure. 11 13 16 Yet, it is still an effective first-line approach to discern most of the group III cases. For group I and II cases, where the radiocapitellar joint matters, the classical principle of the radiocapitellar line, named by Storen,35 intersects the capitellum in all views could help. However, a recent study has found approximately 16% of the normal elbow does not fit that law, especially in AP view of children under 5 years old.36 Thus, the lateral humeral line was introduced by Souder et al37 to complement evaluating radiocapitellar dislocation or incongruity. For all of the PMEL cases, the plastic deformity or gradual malunion of the ulna was an easily neglected condition, which could be responsible for delayed dislocation of the radiocapitellar joint. The line drawn tangential to the posterior border of the ulnar diaphysis has been introduced by Lincoln and Mubarak38 to determine the ‘ulnar bow sign’, and the maximum perpendicular distance of more than 3 mm of this line from the ulnar shaft would be deemed as a possible Monteggia equivalent.
Most of the time, plain radiographs would be sufficient for an acute PMEL. However, for an uncertain occasion or a prolonged history, a vast majority of the authors in this literature series applied advanced examinations, such as CT or magnetic resonance, to discover the occult ulnar fracture or unapparent radiocapitellar joint dislocation. Besides, under anesthesia, techniques, such as B-ultrasonic39 or arthrography,40 could also be employed to ensure that the radiocapitellar joint was congruent for groups I and II of the PMELs.41
Management
Management strategies for the PMELs should depend on the categories. For the most common group III cases, achievement and maintaining the fracture reduction are the priority. In Olney and Menelaus’s7 series, 10 out of 14 were surgically treated, and the operating focus was to prevent ‘common deformity of varus angulation’; and Čepelík et al21’s experience for their 38 cases of ‘displaced Monteggia equivalent’ was a total rate of 76% to internally fix, within which 23.5% were open reducted. The six literature cases we collected revealed four operation choices. As Čepelík et al21 explained, the instability provided by long spiral or oblique fracture of the ulna, the intra-articular fracture of the olecranon, and the hindering of the proximal radial fracture reduction by the incarcerated annular ligament might be the indication for surgery. Moreover, the pins or the elastic nailings are the most used fixations to stabilize the fracture. Plate and screws are sometimes used to control the ulnar varus better.
For group II of the PMEL, a relatively scarce case number makes the treatment choice hard to decide. However, the involved proximal radial fracture might apply the existing management protocol for posterior located Judet IVb or O’Brien III types. Closed reduction seems extremely difficult for this type and has a chance to reverse the radial head 180°, turning artificial surface against the fracture side.12 42 The alternative way is to use the percutaneous leverage technique to assist reduction.43 Rigid Kirschner wire or Metaizeau elastic nailing were the most frequently suggested of this technique. Open reduction for proximal radial fracture and ulnar fracture could be served as in group I, though concern over the issue of potential ulnar fracture still exists. Two literature reports11 12 resented this type with a posterior bowing of ulnar, which went through delayed radiocapitellar joint dislocation and underwent unscheduled operations.
Group I in our review was extremely rare. The two cases demonstrated similar presentations. Considering the late presenting nature and prolonged treatment process of both cases, the diagnosis outweighed the management. Initial anterior bowing of the ulna and subsequent potential for dislocation of the radial head are anticipated to be discovered as soon as possible.
Conclusion
PMEL makes up a considerable proportion of all pediatric Monteggia lesions. It is not properly recognized among the academic community and is frequently misdiagnosed and maltreated. The definition should be unified as an ulnar fracture at any level combined with a proximal radial fracture. We propose to divide it into three groups according to the status of the radiocapitellar joint. The occult ulnar plastic deformity and delayed radial head dislocation should be serious concerns of orthopedists. Surgical need is usually warranted. Maintaining the ulnar length and securing the radiocapitellar joint are highly recommended.
Data availability statement
Data are available in a public, open access repository. As a review article, the data is acquired from the previously published works.
Ethics statements
Ethics approval
Not required.
References
Footnotes
Contributors All of the authors have read and approved the manuscript. Specific authors’ contributions are as follows: LX contributed to conceptualization, data curation, formal analysis, funding acquisition, Investigation, methodology, supervision, validation, visualization, writing - original draft and writing - review & editing; WY contributed to conceptualization and supervision; HL cotributed to data curation, formal analysis and funding acquisition; JX contirbuted to validation and visualization; WZ contributed to data curation Investigation; ZZ contributed to data curation and formal analysis; YY contributed to data curation and methodology.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.