Article Text

Abstract
Objective Rocuronium-associated intravenous injection pain occurs frequently in children during induction of anesthesia. The aim of this study was to systematically evaluate the benefits of nalbuphine in patients with rocuronium-associated injection pain.
Methods Ninety children undergoing tonsillectomy and adenoidectomy in our hospital between October 2019 and September 2020 were randomly divided into the following groups, with 30 patients per group: control group (group C), lidocaine group (group L), and nalbuphine group (group N). Routine 0.1 mg/kg midazolam and 2 mg/kg propofol were injected intravenously. After sedation, children in group C, group L, and group N were administered an intravenous injection of saline, lidocaine (10 mg/mL), or nalbuphine hydrochloride (2 mg/mL), respectively, at a dosage of 0.1 mL/kg. Intravenous injection of rocuronium stock solution (0.6 mg/kg) was administered 2 minutes later. Pain was evaluated using Ambeshs 4-pointscale. The incidence of rocuronium injection pain was compared among the three groups, and postoperative adverse reactions, such as drowsiness, bradycardia, hypotension, and respiratory depression, were evaluated.
Results The incidence of injection pain among children in group N was significantly lower than that in group C and group L (p<0.05). The incidence of drowsiness in group N was significantly higher than that in the other groups (p<0.05). The incidences of hypotension, bradycardia, and respiratory depression were not significantly different among the three groups (p>0.05).
Conclusions Intravenous nalbuphine during induction of anesthesia effectively prevented rocuronium-associated injection pain in children. Drowsiness is a complication.
- anesthetics
- pain
- pediatrics
Data availability statement
Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Rocuronium-associated intravenous injection pain occurs frequently in children during induction of anesthesia.
Pain can immediately cause withdrawal movements, which can lead to increased incidence of pulmonary aspiration in unconscious patients, detachment or displacement of venous catheters, or other emergencies.
Lidocaine is considered one of the most effective drugs for preventing rocuronium injection pain; however, the use of lidocaine alone cannot completely prevent injection pain.
Nalbuphine is mainly used to relieve severe pain and pediatric perioperative pain.
What are the new findings?
This study showed that injecting nalbuphine before rocuronium effectively reduced the incidence of rocuronium injection pain.
Compared with lidocaine, nalbuphine was more effective in reducing rocuronium-associated injection pain.
Due to its sedative effect, nalbuphine might be more suitable for children than lidocaine.
How might it impact on clinical practice in the foreseeable future?
Nalbuphine might be a reasonable drug to reduce rocuronium injection pain.
Introduction
Rocuronium is a non-depolarizing muscle relaxant with an intermediate effect. Compared with other non-depolarizing muscle relaxants such as vecuronium bromide and atracurium, rocuronium has a rapid onset effect.1 Due to this property, rocuronium is used for tracheal intubation during induction of routine anesthesia and maintenance of intraoperative skeletal muscle relaxation. Local pain caused by rocuronium injection is a challenge for anesthesiologists because the incidence of such pain occurs in 50%–80% of adults and in 83%–94% of children.2–4 Rocuronium-associated injection pain occurs in conscious patients. Even after induction of anesthesia, it can produce burning pain. The pain can immediately cause withdrawal movements of the arm and hand and may soon extend to the whole body.5 This type of body movement reactions can lead to increased incidence of pulmonary aspiration in unconscious patients, detachment or displacement of venous catheters, or other emergencies. Therefore, reducing pain caused by rocuronium injection has important consequences in clinical application.
Lidocaine is considered one of the most effective drugs for preventing rocuronium injection pain.6 In addition to drug prophylaxis, studies have shown that the dilution of rocuronium to a lower concentration can also reduce the incidence of injection pain.5 However, the use of lidocaine alone or of low concentrations of rocuronium alone cannot completely prevent injection pain. Many randomized controlled trials in adults have shown that a variety of opioids, such as fentanyl and sufentanil, can effectively reduce the incidence and severity of pain or muscular fasciculations caused by injection of rocuronium.7–9 However, the use of fentanyl and sufentanil in children is associated with risk of chest wall stiffness and reductions in oxygen saturation.
Nalbuphine is a synthetic opioid agonist–antagonist and its structure is similar to those of naloxone and hydromorphone.10 Nalbuphine can produce mild to moderate analgesia through μ opioid receptor and kappa opioid receptor activation.11 Numerous studies have reported its advantages in pain management.12
The aim of our study was to systematically evaluate the benefits of nalbuphine in patients with rocuronium-associated injection pain.
Methods
General information
The parents of patients participating in this study provided written informed consent.
The study comprised a total of 90 patients, aged 4–8 years, who were in American Society of Anesthesiologist (ASA) I risk group, and had undergone tonsillectomy and adenoidectomy at the Children’s Hospital, Zhejiang University School of Medicine between October 2019 and September 2020. Patients who had a recent history of hepatic or renal insufficiency, severe allergic or hypersensitivity reaction to the study drugs, cardiovascular or neurological disease, and those taking opioids were excluded.
Using a computer-based random number method, children were randomly divided into three groups, with 30 patients each group: control group (group C), lidocaine group (group L), and nalbuphine group (group N).
Anesthesia methods
Children underwent intravenous catheterization with a 24 G retention needle before entering the operating room. Once inside the operating room, each patient underwent electrocardiogram (ECG), non-invasive blood pressure (NIBP) measurement, and percutaneous oxygen saturation (SpO2) monitoring, and received oxygen through a mask. The patients in all three groups were treated with 0.1 mg/kg midazolam and 2 mg/kg propofol. After sedation, the children received intravenous administration of saline, nalbuphine (10 mg/mL), or lidocaine (2 mg/mL) at a dose of 0.1 mL/kg. All three groups were administered 0.6 mg/kg rocuronium 2 minutes later, and 2 µg/kg remifentanil was given after muscle relaxation. Intraoperative remifentanil (0.5 µg/kg/min) and propofol (100 µg/kg/min) administration was maintained until the surgery was terminated.
Observation indicators
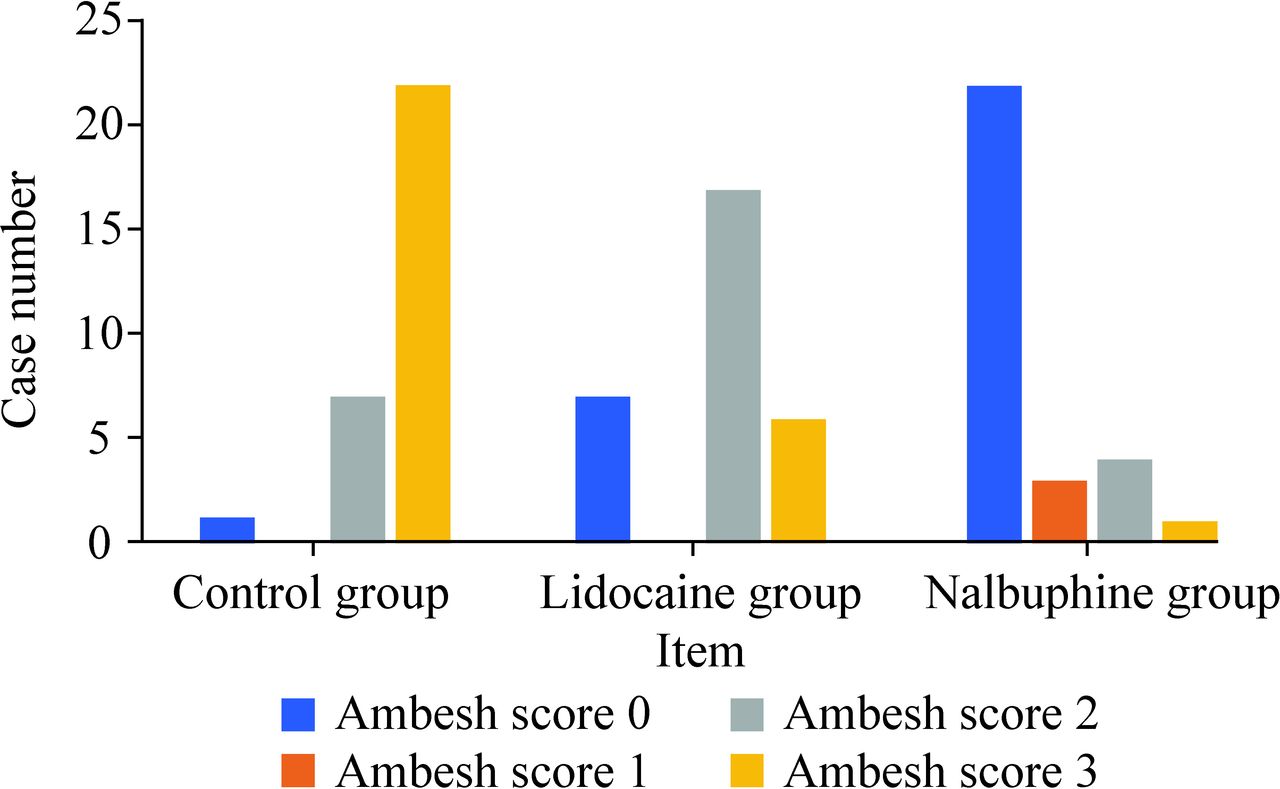
All data were recorded by the same anesthesiologist, who recorded (1) NIBP, heart rate (HR), and SpO2 after entering the room (T1) and at the time of rocuronium injection (T2); and (2) pain scores, which were evaluated using Ambesh’s 4-point scale during injection of rocuronium. Pain was graded based on the following scale: 0, no pain response; 1, mild pain (pain, but no body reaction); 2, moderate pain (pain with obvious limb retraction or movement); and 3, severe pain (painful expression, accompanied by contraction, frowning, and tearing).
Drowsiness means that the patient can be awakened and can answer questions correctly, but without the stimulation, the patient falls asleep soon. Bradycardia was defined as reduction in HR of <60 beats per minute (BPM); 0.1 mg/kg atropine was given when HR decreased to <60 BPM.13 Hypotension was defined as systolic blood pressure (SBP) <80 mmHg or SBP decline of >30% compared with baseline. Respiratory depression was considered if SpO2 was <90%, respiratory rate was <6 breaths per minute, or if airway obstruction with cessation of gas exchange was observed at any time. Jaw thrust and chin lift maneuvers were performed in the event of respiratory depression.
Statistical analysis
The collected data were analyzed using SPSS V.22.0 statistical software. Measurement data are expressed as mean±standard deviation (SD). We used analyses of variance to compare data among the three groups. χ2 test was used to analyze the incidence of pain induced by rocuronium, ASA class, and gender. P<0.05 was defined as statistically significant.
Results
Demographic data
There were no significant differences in age, sex, weight, and ASA classification among the three groups (p>0.05; table 1).
Demographic data of patients and propofol dose in three groups
Vital signs
As shown in table 2, the values of HR, mean arterial pressure (MAP), and SpO2 at T1 were comparable among the groups (p>0.05). In group N, HR and MAP decreased significantly after anesthetic induction at T2. MAP also decreased significantly in group L.
Vital signs in each group
Comparison of injection pain among the groups
The incidence of injection pain (Ambesh score ≥1) was 96.7% in group C, 76.7% in group L, and 26.7% in group N. There was no significant difference between group C and group L (p>0.05). The incidence of injection pain in group N was significantly different (p<0.05) from that in the other two groups (figure 1 and table 3).
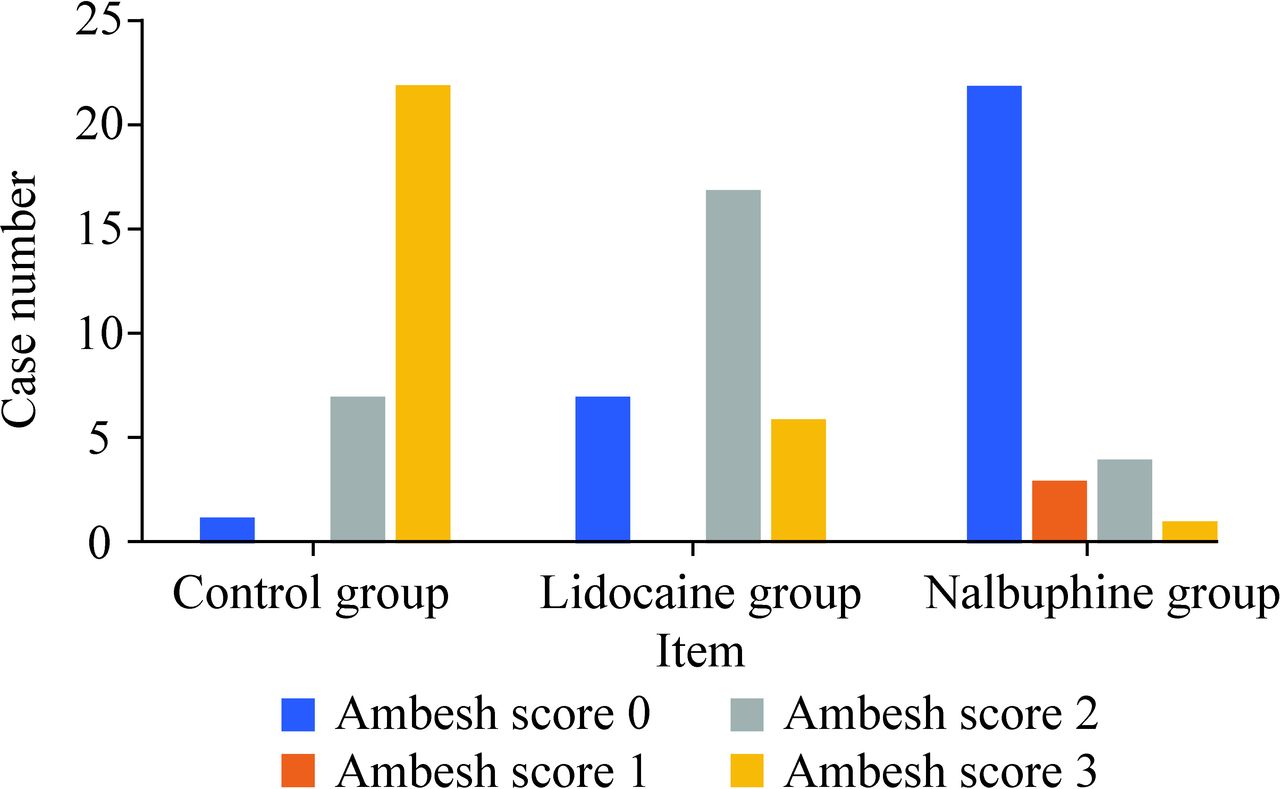
Incidence of Ambesh score 0 in the nalbuphine group was significantly higher than that in the control group and lidocaine group (p=0.001).
Incidence of injection pain
Comparison of other adverse reactions among the groups
Comparison of children in the three groups indicated that the incidence of drowsiness in group N (30%) was significantly higher than that in the other two groups (p<0.05), whereas bradycardia, hypotension, and respiratory depression were not significantly different (figure 2 and table 4).

{kind=link}
{kind=link}
Compared with the control group and the lidocaine group, the incidence of drowsiness in the nalbuphine group increased significantly (p=0.000). RD, respiratory depression.
Comparison of adverse reactions
Discussion
This study showed that injecting nalbuphine before rocuronium could effectively reduce the incidence of rocuronium injection pain. The mechanism of rocuronium-related injection pain remains unknown. It was reported that polymodal nociceptors invested peripheral veins, after being stimulated by unphysiological osmolarity or pH of the drug solution, endogenous pain mediators such as prostaglandins were released.14 The pH of rocuronium is 4.0; neutralized dilution could increase the pH and reduce injection pain.15 16 The dolorific effect of rocuronium might be due to the calcitonin prostaglandin E2 and gene-related peptide, which leads to direct activation of C receptor nerve endings.17
Nalbuphine is an opioid receptor agonist (antagonist analgesic) which mainly acts on the kappa receptor in the spinal cord, and can relieve severe pain (such as burns, biliary colic, cancer, or surgery pain) by activating the kappa receptor at the spinal cord level and the kappa 3 receptor at the upper spinal cord.18 Nalbuphine is also used as an analgesic for angina pectoris, myocardial infarction, postoperative pain, etc. Compared with dezocine and morphine, nalbuphine can relieve adverse reactions such as respiratory depression, nausea, itching, and vomiting, without increasing blood pressure. It also works quickly and lasts long and therefore can be used for pediatric postoperative analgesia.19
According to the Chinese Society of Anesthesiology, in principle, systemic opioids should be less used for patients who need surgery20 because they often cause excessive sedation and respiratory inhibition, even nausea, vomiting, pruritus, and urinary retention.21 A meta-analysis of randomized controlled trials showed that compared with morphine, nalbuphine had similar analgesic effects22 but lack opioid-related adverse effects, such as itching.23 Nalbuphine provided good analgesia of adequate duration and proved to be an acceptable alternative to lidocaine.24 The pros and cons of the results indicate that nalbuphine might be more suitable for pretreatment due to reduced pain during intravenous injection.
The results showed that MAP and HR decreased significantly after induction of anesthesia at T2 in group N. The incidence of postoperative drowsiness was higher in group N than that in other groups, whereas the incidence of other adverse reactions was similar. Drowsiness is one of the common complications of analgesics. The incidence of drowsiness in adults after nalbuphine administration was 32% according to a study by Kubica-Cielińska and Zielińska.10 In one study, a newborn was mistakenly given a dose 10 times higher than the dose required for nalbuphine, which resulted in prolonged sedation without respiratory failure.25 Some studies had shown that nalbuphine injection before anesthesia could reduce stress reaction due to decreased fluctuations in HR and blood pressure during intubation, which might be due to pain relief.23 In this case, the occurrence of drowsiness may also have been due to the analgesic effect of nalbuphine. Intravenous lidocaine blocks Na+ channels in the heart, which inhibites sympathetic transmission and depresses the hemodynamic response,26 and so the MAP decreases significantly in group L.
In conclusion, this study suggested that nalbuphine might be a reasonable drug to reduce rocuronium injection pain in pediatrics. Drowsiness is a complication.
Data availability statement
Not applicable.
Ethics statements
Ethics approval
This study was approved by the Ethics Board of the Children’s Hospital, Zhejiang University School of Medicine on September 30, 2019 (approval number: 2019-IRB-093).
References
Footnotes
Contributors WFH and YH contributed to writing-original draft. DW and HL contributed to data curation. JW contributed to formal analysis. JH contributed to writing-review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.