Article Text

Abstract
Background Necrotizing enterocolitis (NEC) is associated with high mortality and morbidity in neonates. For infants with NEC, intestinal perforation is the most serious complication, and confirming perforation and performing radical surgical treatment as early as possible may reduce mortality and sequelae. The aim of this study was to identify the specific imaging characteristics of intestinal perforation after NEC on supine abdominal X-ray for the early diagnosis of intestinal perforation.
Methods A retrospective study was conducted at the Children’s Hospital of Chongqing Medical University. Infants admitted to the hospital from 2013 to 2020 with NEC (Bell’s stage ≥Ⅱ) were divided into perforation and non-perforation groups. All infants were examined by abdominal X-ray in the erect and supine positions. The sensitivity and specificity of specific X-ray signs were analyzed.
Results A total of 598 infants were included, 113 of whom suffered from perforation. On the supine abdominal films, lucency over the liver shadow, the liver falciform ligament sign, the football sign, the Rigler sign, the triangle sign and more than any one of the above signs had sensitivities of 64.60%, 45.13%, 37.17%, 30.97%, 15.93% and 86.73%, respectively. None of these signs were found on erect or supine abdominal films in the non-perforation group. The total of accuracy of prediction was 46.76%, and the specificity of all the signs was 100%.
Conclusion Specific signs on supine abdominal X-ray could be used to confirm perforation in neonates with NEC with 86.73% sensitivity and 100% specificity.
- child health
- gastroenterology
- neonatology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject
Abdominal radiograph assessment remains an important means of confirming intestinal perforation.
Subdiaphragmatic air is the most obvious imaging feature on erect abdominal X-ray.
Identification of perforation by supine X-ray can be conducted according to some imaging including lucency over the liver shadow, liver falciform ligament signs, football sign, Riglar sign and triangle sign.
What are the new findings
The sign with the highest sensitivity was lucency over the liver shadow.
The triangle sign had the lowest sensitivity.
The total of accuracy of prediction was 46.76%, and the specificity of all the signs was 100%.
How might it impact on clinical practice in the foreseeable future
We can use the sign of lucency over the liver shadow, liver falciform ligament signs, Riglar signs, football signs and triangle signs in supine abdominal film to confirm the perforation of necrotizing enterocolitis with 86.73% sensitivity and 100% specificity.
Introduction
Necrotizing enterocolitis (NEC), a devastating intestinal disease, is associated with high morbidity and mortality in the neonatal population, especially in preterm infants.1–3 Although medical technology has rapidly developed over time, the mortality in infants with NEC who need surgery remains as high as 35%–50%4 5 and has not shown a significant decreasing trend.6–8 In addition, surviving NEC infants develop severe morbidities, such as short bowel syndrome parenteral nutrition-associated cholestasis, poor physical growth and delayed neurodevelopment.1 9 Moreover, infants with advanced NEC who need surgical intervention have an increased risk of neurological impairment.10 For infants with advanced NEC, intestinal perforation is the most serious complication; therefore, confirming perforation and performing radical surgical treatment as early as possible may reduce mortality and sequelae.
In clinical practice, abdominal radiograph assessment remains an important means of confirming intestinal perforation, and subdiaphragmatic air is the most obvious imaging feature on erect abdominal X-ray. However, an erect position is often impracticable for sick neonates that are admitted to the neonatal intensive care unit (NICU) and cannot be transported to the Department of Radiology.11 Cross-table or lateral decubitus images do not require moving the infant and are good options for sick patients. However, identifying free air in infants is difficult on abdominal X-rays taken in the supine position, which might lead to a missed or delayed diagnosis of intestinal perforation.12
Awolaran12 reviewed some case reports of features of gastrointestinal perforation on X-ray, such as the triangle, football and Rigler signs. However, to the best of our knowledge, there have been no reports on the sensitivity and specificity of these signs for the diagnosis of intestinal perforation in infants with NEC. The purpose of this study was to explore the confirmation of gastrointestinal tract perforation based on supine abdominal X-rays in infants with NEC.
Methods
Patients
This retrospective study was conducted at the Neonatal Diagnosis and Treatment Center of the Children’s Hospital of Chongqing Medical University (CHCMU). Infants were diagnosed with NEC according to Bell’s criteria and the modified criteria of Walsh et al.13 14 NEC was defined by the presence of one or more of the following three clinical signs: (A) abdominal distension, (B) bilious gastric aspirate or emesis, (C) occult or gross blood in the stool (no fissure) and one or more of the following three radiographic or sonographic findings: (A) portal vein gas, (B) pneumatosis intestinalis and (C) pneumoperitoneum.
Inclusion and exclusion criteria
The inclusion criteria were all infants who were admitted to the hospital due to NEC from January 2013 to May 2020. Exclusion criteria included infants with spontaneous intestinal perforation, gastrointestinal malformations and infants with incomplete medical information or who did not undergo surgical intervention after the diagnosis of perforation. Infants only with supine position X-ray detection who were receiving mechanical ventilation support with intubation were excluded. Two senior radiologists, blindly reviewed all radiographic images, and a third radiologist was consulted if necessary.
All infants were divided into a perforation group and a non-perforation group. Air under the diaphragm was found on X-rays taken in the erect position in the radiology department in all patients in the perforation group, and massive intestinal necrosis and perforation were confirmed during surgery. Infants without perforation were judged according to the following two features: (1) these infants only received medical therapy and were discharged successfully from the hospital, and none of them died during hospitalization; and (2) all of these infants were examined using X-ray (erect position and supine position), and none of the patients had free air under the diaphragm on X-rays taken in the erect position. Only infants who meet the two criteria were divided into the non-perforated group.
Data collection
The demographic data of the neonates, including gender, gestational age, birth weight, age at admission, surgical intervention and outcomes, were collected. Abdominal radiographic X-ray data were collected, including air under the diaphragm, lucency over the liver shadow,15 the Rigler sign,16 the falciform ligament sign,17 the football sign18and the triangle sign.19
Statistical analysis
Statistical analyses were performed with SPSS V.23.0 (SPSS Inc, Chicago, Illinois, USA). Continuous variables were tested for normality with the Kolmogorov-Smirnov test. Normally distributed data were described as the mean±standard deviation (SD) and were analyzed with Student’s t-test. Skewed data were described as the median and interquartile range (IQR) and were analyzed with the Mann-Whitney U test. Categorical variables were analyzed with the χ2 test or Fisher’s exact test. Statistical significance was established at p<0.05.
Results
Baseline information
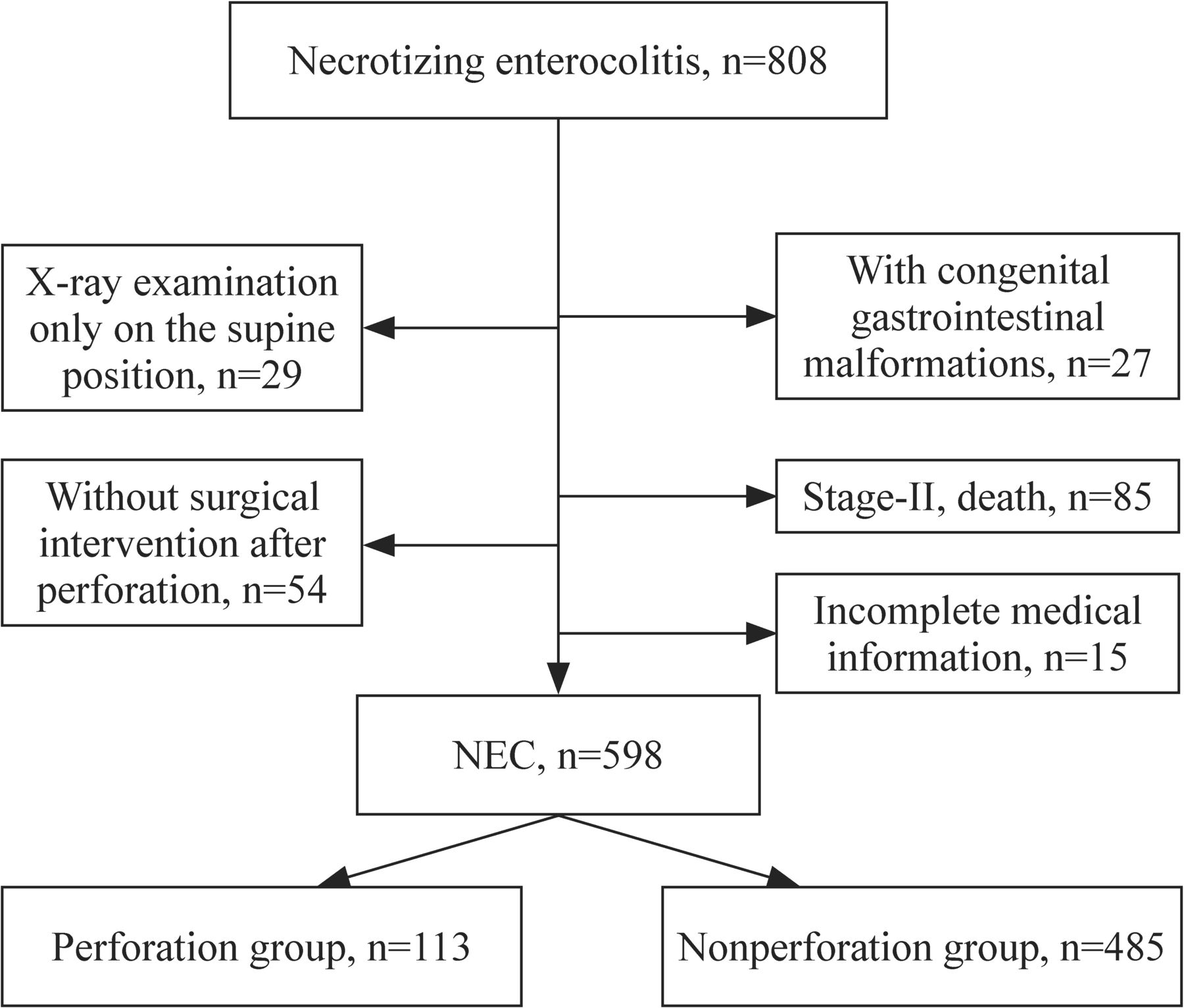
CHCMU is a level III teaching hospital in southwest China, and there are 80 beds in the NICU. A total of 67 753 newborns were admitted to the diagnosis and treatment center of CHCMU during the study period. Among them, 14 306 (21.11%) were premature infants, and 53 447 (78.89%) were full-term or post-full-term infants. During the study period, 808 infants with NEC were admitted to our hospital, and 210 of them were excluded from further study for different reasons (figure 1).

Flow chart of inclusion and exclusion. NEC, necrotizing enterocolitis.
Among these reasons, 54 infants with stage III NEC were excluded because their parents refused surgical intervention after air under the diaphragm was found. Another 85 infants with stage II NEC died and were excluded because we did not determine whether intestinal perforation occurred just before death due to lack of abdominal X-ray examinations. The remaining 598 infants were included in the study. Among them, 113 infants suffered from intestinal perforation, and the other 485 infants had no perforation. The baseline demographic features are shown in table 1. Relatively younger gestational age and a male predominance were found in infants with intestinal perforation. All 113 infants with perforation were treated with surgical intervention, and 26 (23.01%) died due to respiratory failure (n=12) or septic shock (n=14).
Baseline information of infants in the present study
Abdominal X-ray features
Among 113 NEC infants with perforation, air under the diaphragm was identified on abdominal X-rays taken in the erect position (figure 2A). On supine abdominal films, lucency over the liver shadow was observed in 73 (64.60%) infants (figure 2B), and the liver falciform ligament sign was observed in 51 (45.13%) infants (figure 2C). The football sign was found in 42 (37.17%) infants (figure 2D). Thirty-five (30.97%) infants developed the Rigler sign (figure 2E). The triangle sign was found in 18 (15.93%) infants (figure 2F). In addition, 98 (86.73%) infants developed more than one sign. None of these signs was observed on erect or supine abdominal films in the non-perforation group, and significant differences are shown in table 2.
Comparison of specific X-ray imaging signs between the perforation and non-perforation groups, n (%)

{kind=link}
{kind=link}
The specific imaging features on supine abdominal X-ray examination among NEC infants with perforation. (A) Free air under the left hemidiaphragm on erect abdominal X-ray examination; (B) lucency over the liver shadow on supine abdominal X-ray examination; (C) liver falciform ligament sign on supine abdominal X-ray evaluation; (D) football sign on supine abdominal X-ray examination; (E) Rigler sign on supine abdominal X-ray examination; (F) triangle sign on supine abdominal X-ray examination. NEC, necrotizing enterocolitis.
Table 3 shows the sensitivity and specificity of these signs for the diagnosis of perforation. The sign with the highest sensitivity was lucency over the liver shadow, and the triangle sign had the lowest sensitivity; the total sensitivity of these signs was 86.73%. The total of accuracy of prediction was 97.49%, and the specificity of all the signs was 100%.
Performance of specific X-ray imaging signs for the diagnosis of intestinal perforation
Discussion
A total of 598 infants with NEC admitted to our hospital were included in the investigation of the specific imaging features on abdominal X-ray that could be used to confirm intestinal perforation. Most infants had relatively older gestational ages, which was different from other studies.20 21 Previous studies have found that NEC mainly occurs in premature infants.20 21 In infants with a younger gestational age, the incidence rate is higher.22 Formula feeding is an important risk factor. We previously reported the features of NEC in our hospital, and most patients had a relatively older gestational age.23–26 CHCMU lacks an obstetrics department, and most of the patients admitted to our children’s hospital were transferred from other hospitals. The low breastfeeding rate during hospitalization is one of the important factors contributing to the development of NEC.
The surgical and pathological reports for the infants in the perforation group were reviewed, and NEC was confirmed. Intestinal perforation in infants with NEC can be fatal.1 2 In our study, nearly 30% of infants died because of their critical medical condition after perforation. Therefore, early diagnosis and timely surgical treatment might improve the rate of survival. The diagnosis of neonatal intestinal perforation mainly depends on abdominal radiographs. A standard two-view abdominal pelvic radiographic series composed of supine anteroposterior and upright/decubitus/cross-table lateral views is useful for the assessment of the bowel gas pattern and allows for the detection of even small volumes of free intraperitoneal gas.20 Classic subdiaphragmatic air may be the most obvious radiographic sign. However, this examination usually requires neonates to be transported to the Department of Radiology. Infants with NEC are often in critical condition and cannot be moved due to the need for monitoring, intubation and other procedures. Thus, it is challenging for clinicians to confirm perforation when abdominal X-rays are taken in only the supine position in sick infants.
In the present study, we found that the most sensitive sign was lucency over the liver shadow, which occurred in 73 (64.60%) infants with perforation. Lucency over the liver shadow indicates that there is free intraperitoneal air, and an area of hyperlucency in the right upper quadrant obliterating the normal opacity of the liver can be observed.15 The second most sensitive sign was the falciform ligament sign, which could be seen in 51 (45.13%) infants with perforation. The falciform ligament sign can be seen as a longitudinal linear density in the right upper abdomen parallel to the right border of the spine in the supine position, indicating that free air exists in the abdominal cavity.16 The football sign is an oval hyperlucency on a supine radiograph in the shape of an American football, which is seen when there is a large amount of free air.17 We observed this sign in 42 (37.17%) infants with perforation. The Rigler sign occurred in 35 (30.97%) infants with perforation. The Rigler sign can be seen in the supine position when there is air inside and outside of a single loop of the bowel, making the edges of the bowel look much thinner than normal.18 The triangle sign occurred in 18 (15.93%) infants with perforation. The triangle sign occurs when the free air pushes two walls of the bowel apart and creates sharp angles or a triangle; the triangle is bounded by two or three bowel loops, and the lateral peritoneum can be seen on the supine abdominal film.19
Among the 113 infants with perforation, 98 patients had more than one of the above-mentioned signs on abdominal X-ray taken in the supine position, and the diagnostic sensitivity of these signs was 86.73%. None of the above-mentioned specific signs could be found in the other 15 infants, and we only found linear or small crescent-shaped gas shadows on abdominal films taken in the erect position, which suggested that there was only a small amount of free air in the abdominal cavity. The sensitivity of a single sign was not as high, and the total of accuracy of prediction was only 46.76%. For infants with NEC, perforation of the gastrointestinal tract is an absolute indicator for surgery, but not all NEC patients who require surgery actually have signs of perforation on X-ray. Therefore, the judgment of whether infants with NEC need surgery is based on clinical considerations, not just X-ray performance. It is also necessary to examine the early risk factors and X-ray signs of intestinal perforation to provide clinicians with more valuable diagnostic and treatment information.
The specificity of the signs investigated in the present study was as high as 100%, and none of these signs were observed in NEC infants without perforation in the present study. All infants in this retrospective study underwent abdominal X-ray on the erect position and supine position in the radiology department. However, it is sometimes impossible to transfer sick infants, especially those on ventilation after intubation, to the radiology department. Therefore, our findings suggest that intestinal perforation can be confirmed with supine abdominal X-ray, and emergency surgical intervention is recommended if any of these radiographic signs are observed.
The limitations of our study include the errors and bias inherent in a retrospective study. In addition, horizontal lateral position radiography was not performed, which may increase the probability of finding specific signs of intestinal perforation.3
In conclusion, supine abdominal X-ray is important for the timely diagnosis of gastrointestinal tract perforation in infants with NEC. The liver falciform ligament sign, Rigler sign, football sign, triangle sign and lucency over the liver shadow can all be used to confirm perforation in patients with NEC with 86.73% sensitivity and 100% specificity.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Data are available on reasonable request.
Ethics statements
Ethics approval
This study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Children’s Hospital of Chongqing Medical University (Number: 2019–299). The clinical and demographic information of each patient was recorded anonymously, and the Ethics Committee waived the requirement for informed consent because of the anonymized nature of the data and scientific purpose of the present study.
References
Footnotes
Contributors ZH contributed to writing – original draft preparation and writing—review and editing. GL contributed to conceptualization. LKR and HXY involved in data curation. LLQ and LW involved in writing – review and editing. All authors contributed to the article and approved the submitted version.
Funding This study was funded by the Chongqing Municipal Administration of Human Resources and Social Security (Cx2017107) and the Natural Science Foundation Project of Chongqing Science and Technology Commission (cstc2018jscx-msyb-X0027).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.