Article Text

Abstract
Background Although hydrostatic reduction of intussusception with ultrasound (US) or fluoroscopy guidance is well known, it is not yet well established in many low-income and middle-income countries. The aim of the study is to report our results of hydrostatic reduction with intermittent radiography, which has the potential to be practiced in resource-limited settings.
Methods We retrospectively analyzed our patients with intussusception from 2009 to 2019 (11 years). Hydrostatic reduction was performed using water-soluble contrast medium (iopamidol), and reduction was followed with intermittent X-rays taken after every 50 mL of diluted contrast injection. The procedure was not continuously monitored by US or fluoroscopy. Differences in outcome based on age and gender, and yearly trends of admission for intussusception, types of treatment and mortality were analyzed.
Results Among 672 patients, the ratio of boys to girls was 2.46:1.0, and their ages ranged from 1 month to 15 years (median 8 months). Hydrostatic reduction was performed successfully in 351 (52.23%) patients; 308 (45.83%) patients underwent surgery; and 13 (1.93%) patients died before any intervention. There were significant differences in age between patients with successful hydrostatic reduction (median 7 months) and patients needing surgery (median 9 months) (p<0.001). The number of successful hydrostatic reductions increased during the 11 years of the study (R2=0.88). One patient (0.15%) died after hydrostatic reduction, and 10 (1.49%) died after surgery.
Conclusion Hydrostatic reduction with intermittent radiography was performed successfully in more than half of the patients with acceptable complication rates.
- child health
- health services
- hospitals
- pediatric
- pediatrics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Non-operative treatment of intussusception with hydrostatic or pneumatic reduction under ultrasound (US) or fluoroscopic guidance is well accepted.
Many canters in the low-income and middle-income countries (LMICs) could not establish non-operative treatment due to lack of US or fluoroscopy or lack of interest from radiologists.
What are the new findings?
Hydrostatic reduction with intermittent radiography can be performed with similar success and with acceptable complication rates.
It obviates the continuous presence of a sonologist or higher radiation exposure from fluoroscopy.
How might it impact on clinical practice in the foreseeable future?
Centers in LMICs that have X-ray facility can perform non-operative treatment of intussusception and may avoid unnecessary surgery and anesthesia in patients who present early.
Introduction
Intussusception is the most common cause of acute intestinal obstruction in infancy and early childhood with an incidence of one to four per 1000 live births.1 2 It is defined as the invagination of one segment of the bowel into an immediately adjacent segment of the bowel, and the peak age of incidence is between 6 and 9 months.3 4 Non-operative treatments of intussusception are well established and include reduction via hydrostatic or pneumatic pressure.4 5 For hydrostatic reduction, saline enema or Hartman solution is commonly used with ultrasound (US) guidance, and contrast enema is used with fluoroscopic guidance. For pneumatic reduction, room air, carbon dioxide or oxygen is used with either US or fluoroscopic guidance.4 However, operative intervention is indicated if the intussusception cannot be reduced by non-operative interventions if a malignant or other pathological lead point is suspected, or if the patient is unstable, or has evidence of peritonitis or gut perforation.2 6 Various studies have proven that non-operative reduction is safe, quick and effective; that perforation risk is low; and that reduction can be achieved about 70%–85% of the time.2 4
Unfortunately, many centers in our country and in low-income and middle-income countries (LMICs) cannot yet adopt non-operative reduction, and the majority of patients undergo surgical procedures that could have been avoided.7 8 A 20-year, population-based cohort study in Canada showed that 43% of children who presented to a community hospital underwent immediate surgical management for intussusception, compared with just 11% of children at tertiary centers.9 A hospital-based surveillance for intussusception at seven tertiary care hospitals in Bangladesh with pediatric surgical facilities reported that 95% of the patients of intussusception underwent surgery.10 Because non-operative treatment is usually performed by a radiologist in most centers, it can be assumed that reluctance or lack of experience in these procedures may be among the most important causes of failure to establish or sustain this technique in most LMICs.11 12 This procedure is also time-consuming, sometimes messy and involves some risks. The aim of the study was to report our results of hydrostatic reduction using intermittent radiography. The objectives were to describe epidemiological characteristics and to estimate the trend in disease load in the department, the trend of different treatment modalities and the in-hospital mortality rate from this disease. Objectives were intended to re-emphasize the role of hydrostatic reduction as a means of avoiding unnecessary surgery and anesthesia in children.
Methods
Study design and setting
This is a hospital-based, retrospective study carried out in the department of pediatric surgery, Chattogram Medical College Hospital (CMCH), which is the largest government referral center for pediatric surgical services for about one-fifth (about 28.4 million) of the population of the country (161.4 million). The study included all children with confirmed diagnosis of intussusception admitted in this department between January 2009 and December 2019 (11 years). Diagnosis was confirmed by suggestive history with evidence of intussusception in ultrasonogram or contrast enema or naked eye observations during surgery. The study excluded patients who were admitted with ultrasonography (USG) reports of intussusception performed in remote settings but on admission did not have suggestive clinical features or improved spontaneously without any intervention. Patients in whom intussusception was excluded by repeat USG or contrast enema were also excluded from the study. Intussusception mimics in the USG who were diagnosed otherwise during surgery were also excluded.5 Hydrostatic reduction was attempted in patients who had symptoms for less than 3 days, did not have any sign of peritonitis, gut perforation or sepsis, and did not present with severe dehydration or shock. Hydrostatic reduction was performed using water-soluble contrast medium (iopamidol).4 13 However, contrast was introduced gently with a 50 mL syringe through a Foley catheter rather than from a hanging saline bag as traditionally used. Fifty milliliter contrast was diluted with 200 mL normal saline and introduced per rectally though an 18 Fr Foley catheter after inflating the balloon in the rectum and strapping the buttocks with adhesive taps to prevent backflow of liquid. Reduction was followed with intermittent X-rays under supervision of a radiologist from a remote panel attached to the procedure room. Intermittent radiography was performed after every 50 mL of contrast insertion rather than using continuous fluoroscopic monitoring. If the intussusception mass did not reduce, the introduced contrast was sucked back into the syringe and reinserted with a very gentle push. Occasionally, depending on the redundancy of the sigmoid colon and the size of the colon, another 200 mL of contrast mixed normal saline was introduced. The resistance of the mass that would not allow a hydrostatic reduction was a subjective assessment of the radiology technician and was not measured. In cases of mild resistance, some back-and-forth movement of contrast through the syringe helped in the reduction of the mass. Whenever there was more resistance (subjective) to the flow of contrast material or backflow of liquid, the procedure was abandoned. On average, a total of four to six X-rays were performed for a single procedure, which had a lower total dose of radiation than continuous fluoroscopy. The procedures of hydrostatic reductions were performed at three private diagnostic centers near CMCH, and the surgeries were performed at CMCH. All three private centers had fluoroscopy facilities, but the radiologist and the radiology technicians became used to this method and preferred it to fluoroscopic reduction.
Data collection and analysis
Records of all admitted patients with intussusception were added to an Excel spreadsheet (V.2019) to document the date of admission, age, sex, diagnosis, type of treatment and mortality. Data were summarized to present the yearly percentage of patient bulk, age and sex distribution, mode of treatment and mortality. Differences in outcome based on age and gender, and yearly trends of admission for intussusception, types of treatment and mortality were analyzed using Mann-Whitney U test, Kruskal-Wallis test, χ2 test or Fisher’s exact test as appropriate. A p value of less than 0.01 was considered to be statistically significant. R2 values for trend lines were calculated using a linear regression model. Data were analyzed using both Microsoft Excel V.2019 and SPSS V.22 and cross checked.
Results
During the study period, a total of 28 289 patients were admitted in this department, and among them, 672 (2.38%) patients had confirmed diagnosis of intussusception. These included 478 male patients and 194 female patients (ratio 2.46:1.0). The male to female ratio of all admitted patients was 1.91:1.0. The age of the patients with intussusception ranged from 1 month to 15 years with a median age of 8 months (male patients: 8 months and female patients: 7 months, p=0.55). The majority of the patients were between 6 and 12 months of age (343, 51.04%) followed by less than 6 months of age (163, 24.26%). Table 1 shows the age distribution of the patients and their relation with gender, mode of treatment and mortality.
Age distribution of the patients and their relation with gender, treatment and outcome (n=672)
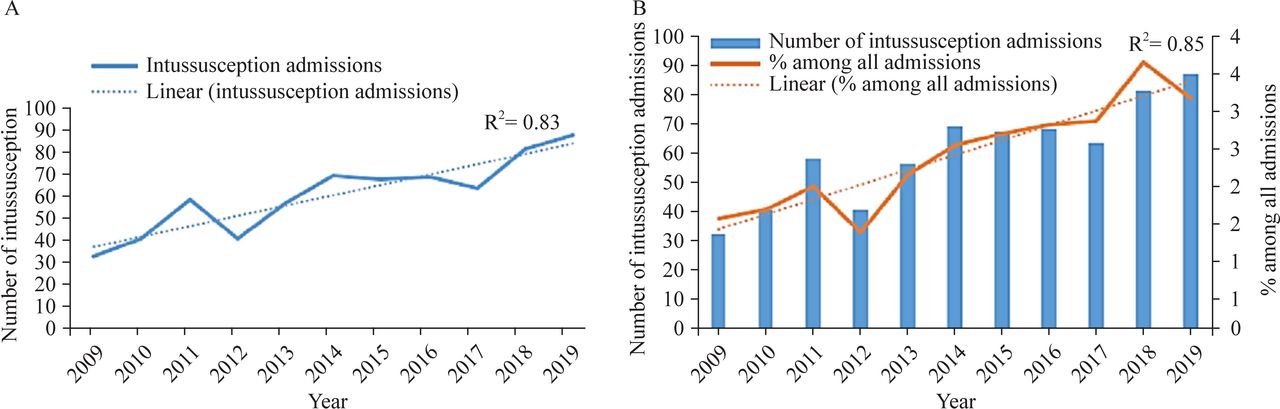
Yearly admission for intussusception ranged from 33 to 88 patients; on average, 61 patients were admitted every year. There was a gradually increasing trend in the number of admissions for intussusception (R2=0.83), and the proportion of patients with intussusception among all admitted patients also increased gradually (R2=0.85) during the 11 years of the study (figure 1).

Yearly numbers and percentages of intussusception admissions (n=672). (A) Gradually increasing trendline of total yearly admissions for intussusception. (B) Yearly percentage for intussusception admissions among all admissions also increased gradually.
Between 2009 and 2019, hydrostatic reduction was performed successfully in 351 (52.23%) patients; 308 (45.83%) patients needed surgery and 13 (1.93%) patients died before any hydrostatic reduction or surgery could be performed. Figure 2 shows the comparison of various types of treatment modalities used on the patients. Among the patients needing surgery, operative manual reduction was done in 185 (27.5%) patients. Intestinal resection anastomosis was done in 101 (15%) patients who had necrosed gut, and exteriorization of gut was performed in 22 (3.3%) patients who had gangrenous gut, along with features of sepsis. The median age of the patients who underwent successful hydrostatic reduction during this 11-year period was 7 months, whereas the median age of the patients who underwent surgery or died before intervention was 8 months (p<0.001). We could analyze the proportion of failed hydrostatic reduction only from 2014 to 2019 (6 years) because prior to that period, only the number of successful reductions was recorded. The patients who experienced failed attempt of hydrostatic reduction and who subsequently needed surgery were recorded as patients needing surgery, and the type of surgery performed and the outcome were recorded. Between 2014 and 2019, among a total of 434 patients of intussusception, hydrostatic reduction was attempted in 312 (71.89%) patients, and it was successful in 257 (82.37%) patients. The remaining 55 (17.62%) patients needed surgery. Although the median age of this cohort of 312 patients was 8 months, median ages of the patients with successful and failed hydrostatic reductions during this period were 9 and 7 months, respectively (p<0.01). There was only one (0.32% among 312 attempts) case of perforation following hydrostatic reduction during the period ‘2014–2019’, and the patient later underwent repair of perforation and survived. We could not analyze the rate of perforation following hydrostatic reduction during the period ‘2009–2013’ as these were not documented properly.

Types of treatment for intussusception during the total study period (2009–2019), n=672.
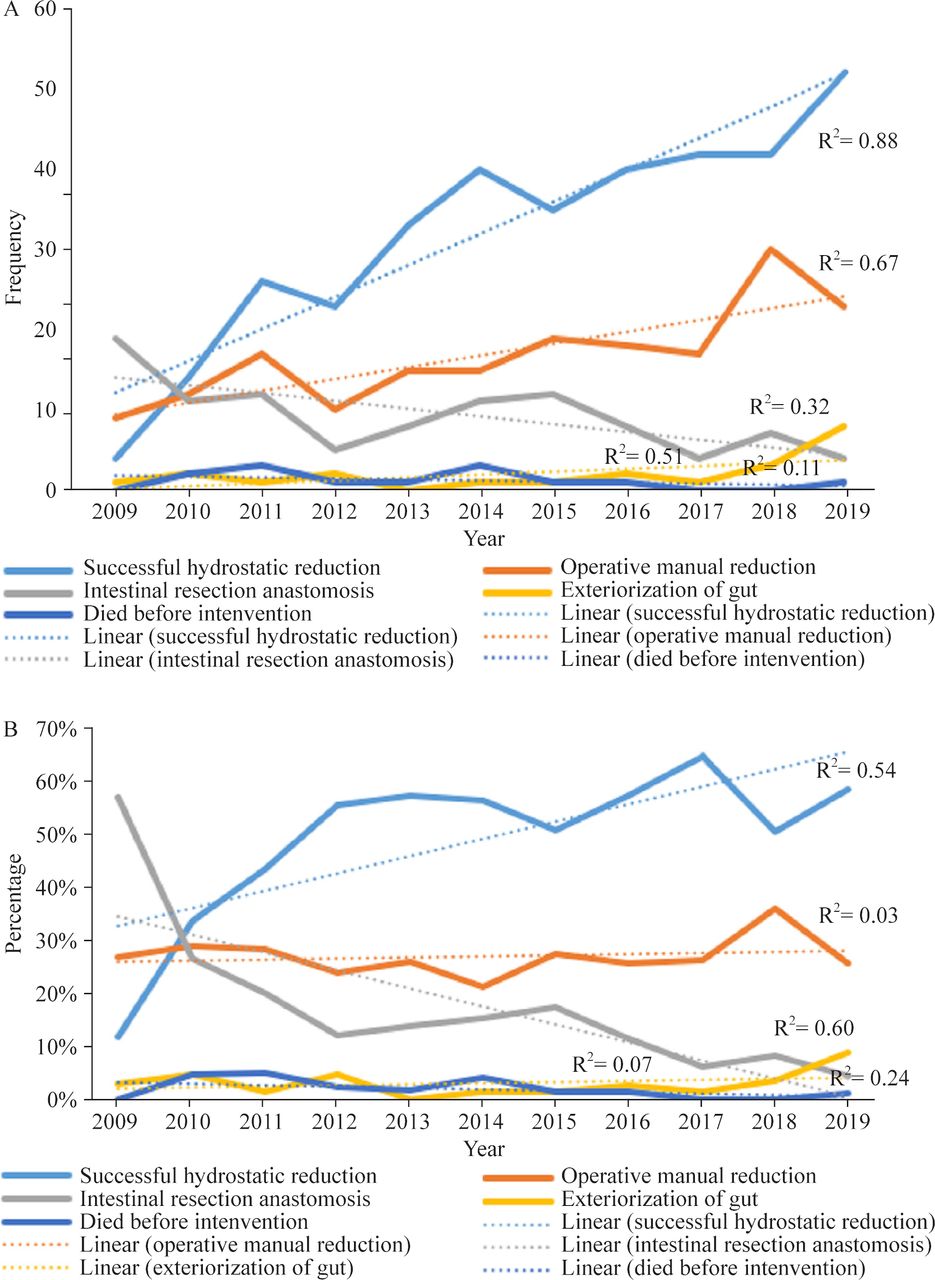
The number and proportion of successful hydrostatic reductions increased over the years, respectively (R2=0.88 and 0.54) (figure 3). Although the number of operative manual reductions also increased (R2=0.67), the proportion remained almost constant (R2=0.83). Both the number and proportion of resection anastomoses decreased over time (R2=0.32 and 0.60, respectively), whereas the number and proportion of exteriorization of gut remained almost constant (R2=0.51 and 0.07, respectively).
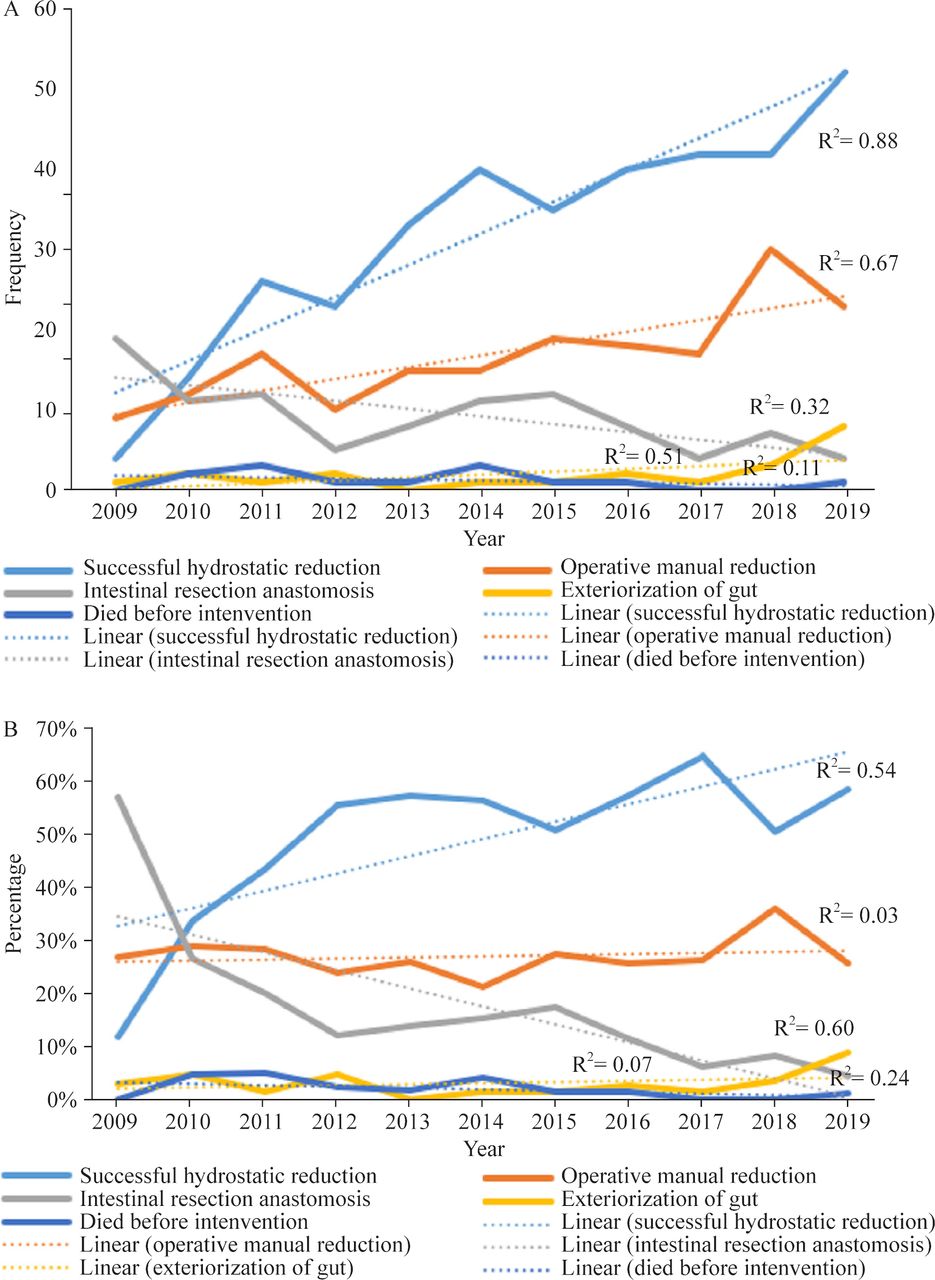
Frequency and percentage of different types of treatment modalities during the total study period (n=672). (A) Yearly frequencies and (B) yearly percentages of treatment modalities.
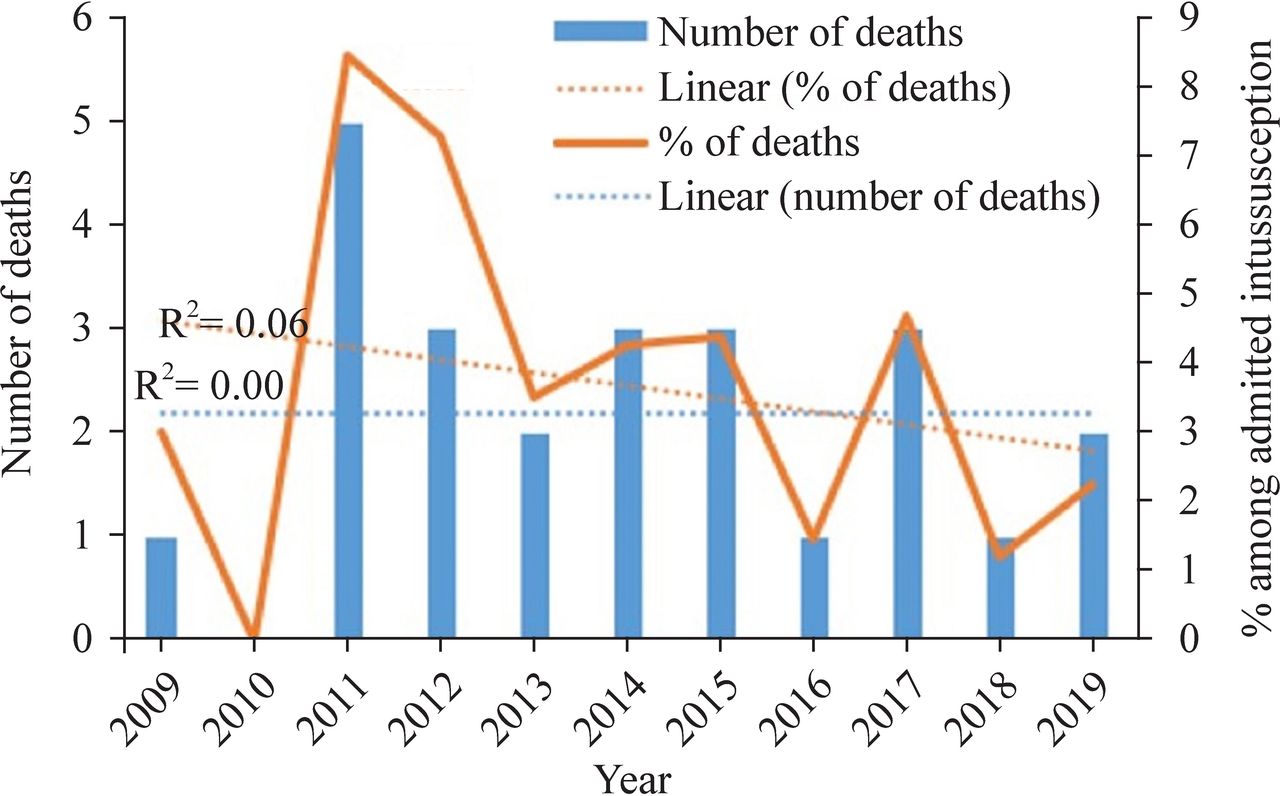
Among all admissions for intussusceptions, 24 (3.57%) patients died in the hospital. Among them, 13 (54.17% of all deaths, 1.93% of all patients) died before any intervention; 10 (41.67% of all deaths, 1.49% of all patients) died after surgery with no hydrostatic reduction attempted previously; and 1 (4.17% of all deaths, 0.15% of all patients) died following surgery after failed attempt of hydrostatic reduction. Yearly death ranged from 0% to 8.47%, and on average, two patients died every year from intussusception. Although the trendline for the number of deaths from intussusception remained almost flat (R2=0.00), the trend for the percentage of deaths among admissions for intussusception decreased gradually (R2=0.06) (figure 4). Among the mortalities, 22 were infants, and 2 patients were between 1 and 2 years of age; however, there were no significant differences in mortality between genders or among age groups (p=0.43 and 0.38, respectively) .

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Yearly frequency and percentage of deaths from intussusceptions during the total study period (n=24).
Discussion
This study shows that hydrostatic reduction with intermittent radiography was performed successfully in about 52% of all cases of intussusception admitted in our department. Although this was lower than that of many high-income countries, it still avoided surgery and anesthesia in more than half of the patients. It is, however, well-known that delayed presentations of surgical conditions are common in LMICS, which might explain the relatively lower proportion of hydrostatic reductions in our series. A recent study that included eight large specialty pediatric hospitals in Chennai, India, reported that 59.8% of their cases were managed non-operatively.1 In these hospitals, either US-guided hydrostatic reduction or fluoroscopy guided air enema reduction was used. In a 14-year study from a UK referral center, 44.48% patients were reduced successfully by non-operative treatment and 48% needed surgery.14 However, air enema was used instead of liquid enema. Another study involving four hospitals in Hunan and Henan Provinces of China between 2009 and 2013 reported that among 1715 intussusception cases, air or liquid enema reduction was performed in 80% cases; 16.3% required surgery without intestinal resection; and 2.6% required surgery with intestinal resection.15
Non-operative reduction of intussusception is not practiced in most centers in Bangladesh, including the major referral centers in the capital city. Occasionally, there have been scattered efforts to establish US-guided or fluoroscopy-guided reduction at some centers, but these efforts could not be sustained. An earlier study involving two centers in our country showed a 90% success rate of US-guided hydrostatic reduction of intussusception, although this procedure could not be sustained in these institutes.11 The main reason may be attributed to the lack of interest from the radiologists as this is a time-consuming procedure, and there is an excessive load of patients with other diseases. There is also a fear of potential perforation of gut. Reduction with US guidance requires a continuous presence of the sonologist and demands a significant amount of time. Many sonologists are also not comfortable with apprehended and crying infants, and sometimes this procedure is chaotic. The method of non-operative reduction varies from center to center. Barium was the contrast agent of choice when the procedure was initially introduced. However, barium is no longer advocated owing to concerns over peritoneal staining if perforation occurs.5 Nowadays, pneumatic enema or hydrostatic enema with saline or water-soluble contrast are the dominant techniques, and most centers perform them under US guidance. However, fluoroscopy-guided contrast enema reduction is also widely practiced.5 Numerous studies have compared air and liquid methods with variable results. However, a meta-analysis of more than 32 000 children from 102 studies showed that air enema reduction had higher success rate than hydrostatic reduction, but both had similar perforation rates.16 They opined that air enema is cleaner, less expensive, and has shorter fluoroscopic time and lower radiation exposure. A Cochrane meta-analysis of six randomized controlled trials with a total of 822 participants also found superiority of air enema over liquid enema, although they described the evidence as of low quality.17 A survey on North American pediatric radiologists conducted in 2015 showed that 96% used fluoroscopy and 4% used US guidance for reduction; 78% used air enema and 20% preferred liquid enema to reduce intussusception.16
In the present study, intermittent radiography was used to monitor the progress of hydrostatic reduction rather than for continuous fluoroscopic guidance. The key to success of this procedure was very gentle and controlled insertion of contrast material through a Foley catheter. Contrast was inserted through a 50 mL syringe rather than from a hanging saline bag. This also saved time, and the technician could subjectively assess the resistance to flow during insertion. However, the established method of hanging saline bag can also be adopted for reduction with intermittent radiography guidance. Fluoroscopy is not available in many centers, and it has added hazards of higher exposure of radiation than plain radiography. On the other hand, USG needs continuous presence of a sonologist. X-ray is available everywhere and is cheap; a radiography technician can perform it successfully and safely if properly demonstrated. This procedure has the potential to be introduced even in remote centers that have X-ray facilities, and it will reduce delays to transfer patients to a tertiary center. Delays in the management of intussusception compromise both anatomical and physiological viability of the intestine and lead to bowel necrosis, gangrene, perforation and peritonitis. These lead to increased rates of surgery and to mortality from intussusception in many LMICs.18 Hydrostatic reduction is reasonably safe. The only case who had a perforation (0.32% among 312 attempts between 2014 and 2019) after an attempted hydrostatic reduction had features of peritonitis and was misjudged by a junior resident and was referred for hydrostatic reduction without consulting a senior resident or a consultant. The patient later underwent surgery, where a perforation in the transverse colon was repaired and proximal ileostomy was performed. The patient was then discharged well. After this event, the radiology team also became vigilant in selecting cases of hydrostatic reduction and refused the procedure in several patients who had been referred with features of peritonitis. However, the rate of perforation (0.32%) is lower than many series with US-guided or fluoroscopy-guided reductions and is comparable to the meta-analysis that compares perforation rates of air enema (0.39%) and liquid enema (0.43%) reduction.16 One patient who died after a failed attempt of hydrostatic reduction had a gangrenous segment in the transverse colon. There was no perforation of gut and no spillage of contrast. The gangrenous gut was excised, and a transverse colostomy was performed because of bad general condition. However, on the fourth day of hospitalization, the patient died of sepsis.
In our study, the magnitude of intussusception admission was 2.38% of all admissions, and it had an increasing trend. A recent systematic review estimated that the annual incidence of hospital admissions for intussusception ranged from 34 to 90 per 100 000 children under 1 year of age.19There has been recent concern about the increased incidence of intussusception due to vaccination against rotavirus. However, it has been suggested from a modeling analysis based on 135 countries that rotavirus vaccines had a favorable benefit–risk profile in LMICs.20 We could not analyze the impact of rotavirus vaccination during the increasing trend in our series because vaccination was not recorded. Moreover, it is difficult to comment on whether the increase in the number of cases in our series was an actual rise of patients or occurred due to an increase in number of patients seeking medical advice.
Although we could not analyze the overall success rate of attempted hydrostatic reduction in our patients, the analysis of patients from 2014 to 2019 (434 patients in 6 years) showed an 82.37% success rate. The meta-analysis of 102 studies estimated the success rates of air enema and liquid enema to be 82.7% and 69.6%, respectively.16 We did not use any anesthesia or sedation for hydrostatic reduction. The use of anesthesia or sedation is not described well in most series. However, some centers are known to use sedatives, such as propofol, morphine or ketamine, for hydrostatic reduction.21 22 Overall, 46% of our patients underwent surgery in our study. A recent review of 1158 cases from seven African countries showed that more than 87% of the patients with intussusception in these countries underwent surgery.8 Mortality from intussusception in our series was 3.57%. However, intussusception (9.94%) was the most common cause of infant mortality, which is also consistent with findings from other countries for this age group. Centers that use ‘surgery only’ for the treatment of intussusception reported mortality rates ranging from 8% to 32%, a sharp contrast to less than 1% mortality rate in high-income countries who have facilities for hydrostatic or air enema reduction and where patients usually present early.23 24 Although delayed presentation is very common in LMICs, hydrostatic reduction with this simpler technique may avoid unnecessary surgery and anesthesia in select cases who present early. However, ‘hydrostatic or air enema reduction alone’ cannot always be successful, and patients who develop peritonitis, bowel perforation or shock usually need surgeries.17 Clark et al, in their systematic review, showed that mortality for African countries was 10%, and that for the rest of the world was less than 0.05%–1.0%.19 A recent WHO-funded report from an active, hospital-based surveillance from seven sub-Saharan countries showed that hospital mortality rate was 13% among 1017 admissions. Female gender, longer duration of symptoms prior to presentation and undergoing intestinal resection were associated with higher mortality.25 The male to female ratio of our intussusception admissions was 2.46: 1.0, and this ratio among mortalities was 3.8:1.0, which implies that more boys died from intussusception than girls in our series. However, this difference was not statistically significant (p=0.43). Among the patients who died in our series, 54.17% died before any hydrostatic reduction or surgery could be performed. These patients presented very late with features of shock or sepsis and died during the resuscitation process. Many patients in the LMICs are initially maltreated by unqualified village. Often, in such cases, they are treated as bacillary dysentery, and by the time they are referred to surgical facilities, bowel compromise and its sequelae become irreversible.23 24
The present study has several limitations. This was a retrospective study, and we could not evaluate signs and symptoms and their duration in the patients, and their relations with modes of treatment. We also could not evaluate presence or absence of pathological lead points because these were not properly documented. Because we lacked a unique patient identity number and the previous history of intussusception was also not always recorded, we did not calculate the recurrence of hydrostatic reduction in these patients. However, in our experience, recurrence was very uncommon and a recent meta-analysis reported similar low recurrence rates among different modalities of reductions.26 We also could not analyze the number of repeated attempts of hydrostatic reduction after the initial failed attempt due to lack of data entry; however, repeated attempts at reduction were also performed very rarely. Nevertheless, we believe this study showed a feasible alternative for the centers in the LMICs who could not establish hydrostatic reduction. Although this procedure is old-fashioned and subjective, it can be reproduced in many resource-limited settings which could not yet adopt other methods of reduction and can avoid unnecessary surgery and anesthesia in children. Some patients were out of evaluation for some variables because of lack of sufficient data, but the number of patients in whom these were evaluated is substantial. It provides sufficient data for the assumption of the success of hydrostatic reduction with intermittent radiography. Other centers may perform prospective comparative studies to evaluate our results.
In conclusion, hydrostatic reduction with intermittent radiography was successfully performed in about half of the patients of intussusception. Both the number of admissions for intussusception and the number of successful hydrostatic reductions increased with time. There was a gradually decreasing trend of intestinal resection–anastomosis.
Acknowledgments
The authors acknowledge all persons involved in the setting up of hydrostatic reduction for the patients with intussusception in this department and all the past and present faculties, trainees and personnel involved in the record keeping of these patients. The authors also acknowledge Dr Md Monjurul Hakim (MPH), assistant professor, Department of Community Medicine, Rangamati Medical College, for his assistance in statistical analysis; and Dr Qumrul Hasan Chowdhury, assistant professor, Department of English, University of Dhaka, for improving the manuscript by editing for correct usage of English.
References
Footnotes
Contributors TKC contributed to data curation, formal analysis and writing-original draft. MQA contributed to conceptualization, investigation and methodology. MZC, MTSC, MSI, MAA contributed to data curation. MAAF contributed to writing, including review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The ethical review committee of Chittagong Medical College approved this study (memo no: CMC/PG/2020/102).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request from the corresponding author.