Article Text

Statistics from Altmetric.com
Sclerosing angiomatoid nodular transformation (SANT) is a rare splenic lesion first described by Martel et al in 2004.1 As reported, SANT is a benign vascular lesion of the red pulp of the spleen, presenting under the microscope as angiomatoid nodules in a fibrosclerotic stroma. Although more than 200 cases have been reported in the English literature,2 only 8 cases have been found in children. SANT is most often suspected from imaging studies performed for another reason. Nevertheless, no signs are specific.3 This motivates surgery to remove the mass and confirm the diagnosis. The surgery could be done either by open, laparoscopic partial or total splenectomy.4 Herein, we reported two pediatric cases of SANT that were well treated by laparoscopic total and partial splenectomy.
A 14-year-old girl was referred to our pediatric surgery department for further investigations of a solid tumor of the spleen. The mass was diagnosed by a routine ultrasonography (US) performed in the pediatric endocrinology department in the context of urinary tract infection and chronic asthenia. The patient’s medical and family history was unremarkable. On physical examination, she had good general condition without anorexia, fever or night sweats. Neither hepatosplenomegaly nor lymphadenopathies were found. The patient’s blood tests showed anemia (hemoglobin 85 g/L) and increased inflammatory markers [C reactive protein (CRP): 18 mg/L and erythrocytes sedimentation rate (ESR): 40 mm/hour]. Abdominal US imaging found a calcified heterogeneous vascularized central splenic mass with a maximal diameter of 7 cm (figure 1A). The US finding was confirmed by an MRI which showed a splenic vascular tissular lesion that had an iso-intense signal on T2 sequence and a progressive signal enhancement of the central portion after injection (figure 1B). Two weeks prior to surgery, she was vaccinated against Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis. Laparoscopic total splenectomy was performed. The spleen was extracted without fragmentation through a suprapubic incision with the use of an endoscopic bag. On gross examination, the spleen weighed 450 g and measured 12×9×5 cm (figure 2). Histological examination showed a well demarcated multinodular lesion respecting the surrounding borders of the splenic parenchyma. The lesion was surrounded by a reactive fibrous tissue and was mainly composed of proliferative fusiform cells without cytonuclear or mitotic anomalies (figure 3A). Immunohistochemical staining showed that cells expressed CD31 and smooth muscle actin (figure 3B), vessels most often expressed CD34 and/or CD31 whereas CD8 showed only rare sinuses trapped within these nodules. CD21, anaplastic lymphoma kinase (ALK) protein detection and in situ hybridization for the presence of Epstein-Barr virus-encoded small RNA were negative. These findings were matched with a SANT. The patient’s postoperative course was uneventful. She was discharged home on day 5 with oral penicillin prophylaxis for 5 years. She remained free of symptoms and her blood tests returned to normal 6 months postoperatively. Abdominal ultrasound showed no recurrence of the lesion after 8 years of follow-up.
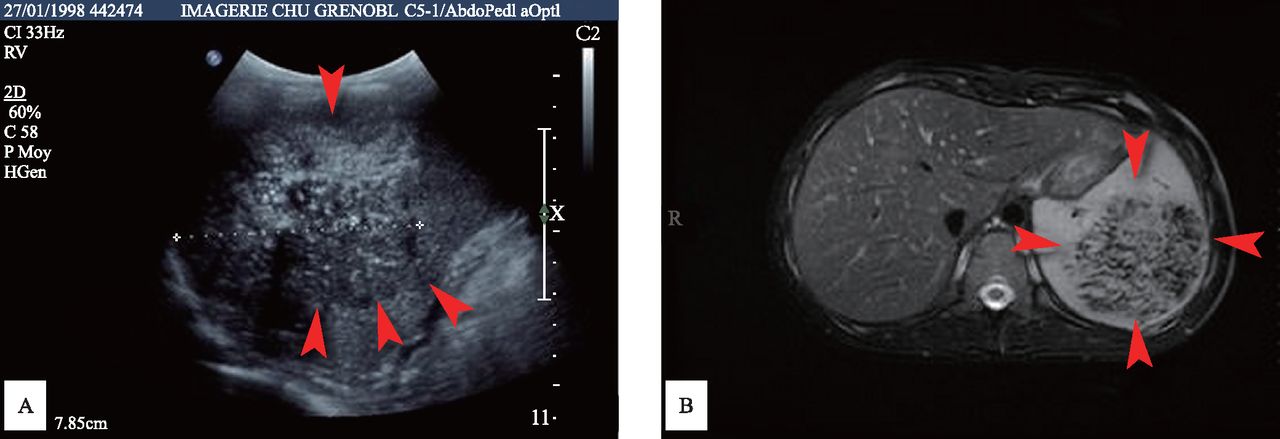
Imaging results of case 1. (A) Abdominal US imaging found a calcified heterogeneous vascularized central splenic mass (arrows) with a maximal diameter of 7 cm. (B) MRI showed a splenic vascular tissular lesion with a maximal diameter of 7 cm (arrows) that had an iso-intense signal on T2 sequence and a progressive signal enhancement of the central portion after injection. US, ultrasonography.

The gross examination of the spleen extracted without morcellation in case 1. The spleen weighed 450 g and measured 12×9×5 cm.

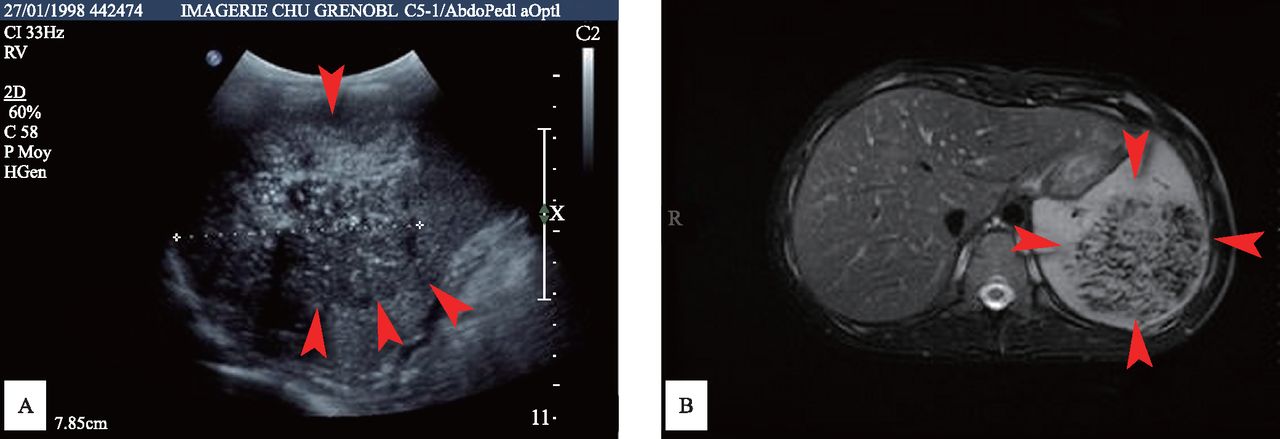
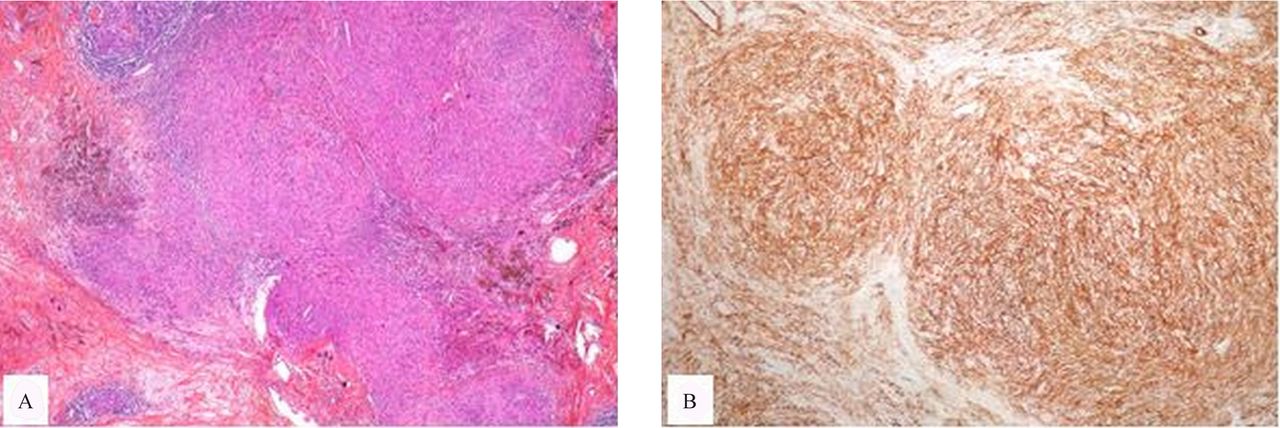
Histopathological results of case 1. (A) Histological (HES ×100). The histological examination showed a well-demarcated multinodular lesion respecting the surrounding borders of the splenic parenchyma. The lesion was surrounded by a reactive fibrous tissue. (B) Immunohistochemical (immunohistochemistry ×100). The immunohistochemical staining showed that cells expressed SMA. HES, hematoxylin and eosin stain; hSMA, smooth muscle actin.
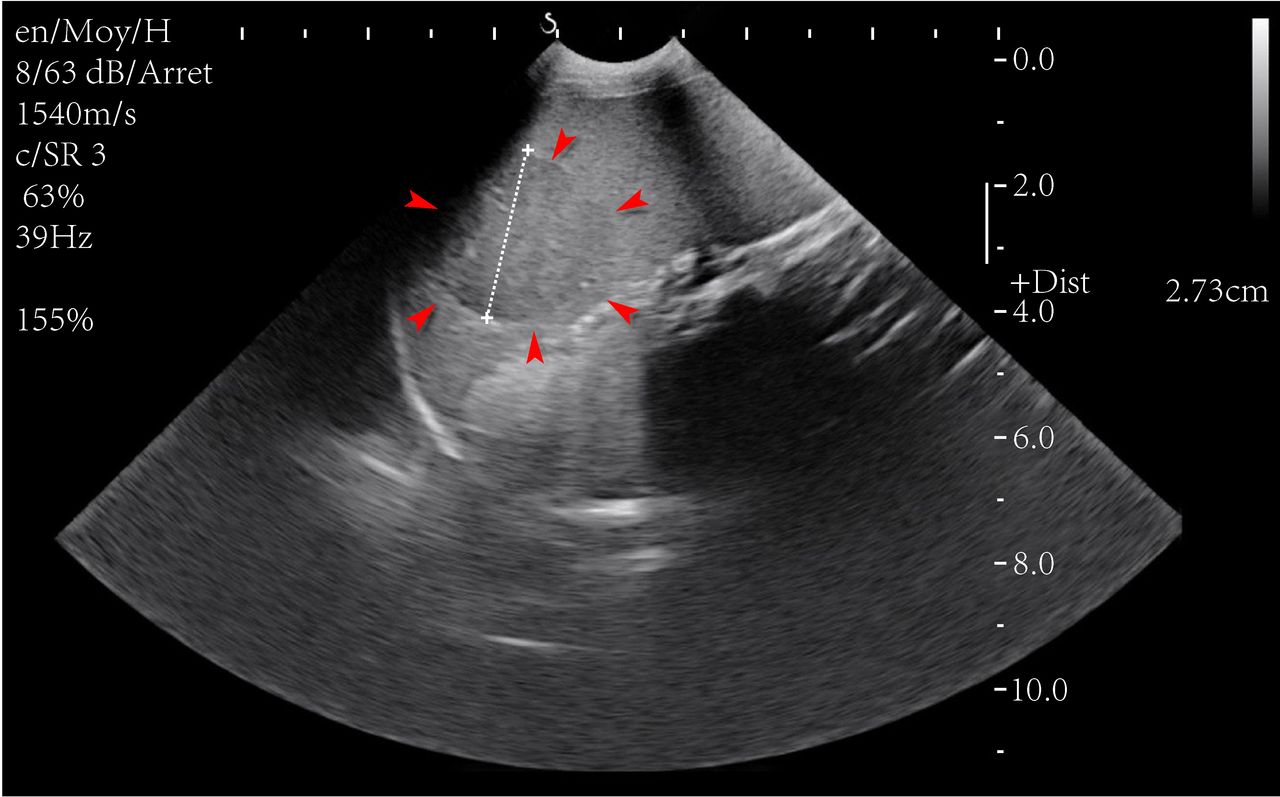
A 4-year-old boy was admitted to our pediatric surgery unit for management of a splenic lesion. His mother reported a history of recurrent bouts of abdominal pain for a year. The patient had been hospitalized for bronchiolitis complicated with respiratory syncytial virus pneumonia at 6 months of age. His mother also reported a history of pyelonephritis at 11 months and adenoidectomy with tympanostomy at 18 months of age. He was referred to our department after an incidental finding of a heterogeneous tissular intrasplenic mass (figure 4) found on ultrasound performed by pediatricians. On physical examination, he was slightly pale without jaundice. He had a soft and non-tender abdomen with no palpable hepatosplenomegaly. A small cervical lymphadenopathy is found. The patient’s white blood cell count, platelet count and hemoglobin were, respectively, 10 000/mm3, 342 000/mm3 and 13.2 g/dL. His inflammatory markers (ESR: 11 mm/hour and CRP 1 mg/L) were on normal limits. A decision was made to monitor the spleen mass with ultrasound imaging every 3 months. The mass increased from 2.5 to 3 cm on an US performed 3 months later. Laparoscopic partial splenectomy (LPS) was performed. Two weeks prior to surgery, she was vaccinated against S. pneumoniae, H. influenzae, and N. meningitidis. The resected spleen was extracted without fragmentation through a suprapubic incision with the use of an endoscopic bag. The gross examination of the resected spleen showed two fragments measuring respectively 6.5×4×3 cm and weighed 29 g with cystic architecture, 3×3×2 cm weighing 13 g with homogenous nodular aspect (figure 5). The histological analysis showed many confluent fibrotic nodules centered by vessels, associated with plasma cells, lymphocytes and macrophages (figure 6A). The immunohistochemical examination showed positive staining with CD31 and CD34 (figure 6B) by these vessels, while macrophages stained positive with CD68 and CD163. Histological and immunohistochemical findings were in favor of SANT. Postoperative course was uneventful and the patient was discharged from hospital on day three with oral penicillin prophylaxis for 5 years. An US performed 3 years postoperatively found a homogeneous spleen measuring 7 cm in diameter without recurrence of the mass after 6 years of follow-up.

Imaging results of case 2. Ultrasonography showed a heterogeneous tissular intrasplenic mass (arrows), located on the lower pole of the spleen and measured 3 cm of maximal diameter.

The gross examination of the resected spleen showed two fragments measuring respectively 6.5×4×3 cm and weighed 29 g with cystic architecture, 3×3×2 cm weighing 13 g with homogenous nodular aspect (arrows) in case 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
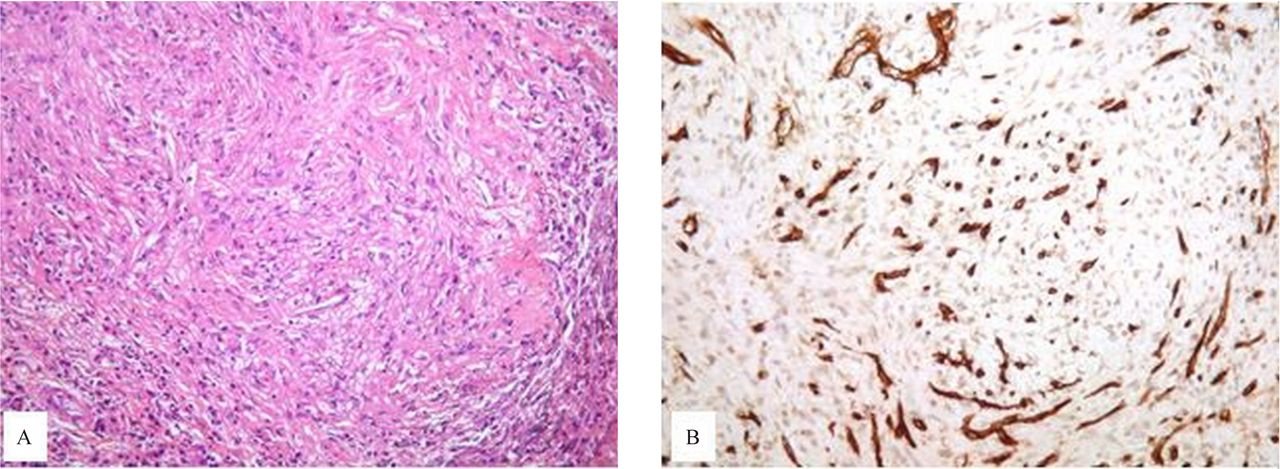
Histopathological results of case 2. (A) Histological (HES ×200). The histological analysis showed many confluent fibrotic nodules centered by vessels, associated by plasma cells, lymphocytes and macrophages. (B) Immunohistochemical (immunohistochemistry ×400). The immunohistochemical examination showed positive staining with CD31 and CD34 by these vessels, while macrophages stained positive with CD68 and CD163.
SANT has a female predominance and mainly affects adults in the fourth to seventh decades of life.5 Although reports of SANT in the pediatric population are extremely rare, the subject seems to generate interest as some authors believe that pediatric cases may harbor a more aggressive form of the disease.6 Currently, there are no pathognomonic imaging signs. However, imaging may help to distinguish SANT from other solid splenic masses. The first imaging appearance of SANT was described by Li et al.7 Thereafter, Karaosmanoglu et al reported the spoke-wheel pattern.8 It is a lesion that presents diffuse peripheral enhancement on the early arterial phase with progressive centripetal filling in a radiating pattern, while its center remains, respectively, hypodense and hypointense on the late phase images of CT and MRI. Despite this imaging progress, the diagnosis of SANT is based on histopathology and immunohistochemistry.9
To date, only eight cases of SANT have been reported in children. Among these cases, there were five males and three females. In contrast to adult series, herein we found a male predominance. In this study, the median age was 9 years (range, 0.2–17 years). Symptoms at presentation were recurrent abdominal pains, vomiting, asthenia and growth retardation. The physical examination revealed a splenomegaly, anemia, abdominal pain and cervical lymphadenopathy. However, in two patients, the diagnosis was made incidentally. Demographics, physical features, surgical treatment and follow-up of children with the SANT of the spleen were summarized in table 1. The present study reports the first child operated by LPS and advocates its safety and efficiency in children on the basis of literature review. Improvement of laparoscopic equipment and techniques have made LPS widely used in digestive surgery as well as in the treatment of focal benign splenic lesions. This has been facilitated by the understanding of splenic anatomy, especially knowledge of the intrinsic and extrinsic vascularization of the spleen.
Demographics, physical features, surgical treatment and follow-up of children with the sclerosing angiomatoid nodular transformation of the spleen
Recently, Jin et al4 suggested that LPS appeared to be a technically feasible and therapeutically effective approach for SANT. Authors have reported 37 adult patients managed by open splenectomy (12 patients), laparoscopic splenectomy (12 patients), or LPS (13 patients). The authors found no difference regarding the operation time, blood loss, length of hospital stay, or postoperative complications among the three groups. Thus, current partial laparoscopy is based on the surgical anatomy of the spleen. Devascularization of a specific segment creates a demarcation line, which allows resection of the segment.4
In our study, the choice of partial or total splenectomy was based on size and/or location of the lesion. Thus, in our first clinical case, the spleen lesion was central and was measured to be 7 cm in diameter (that is, more than half of the spleen itself). In this circumstance, partial splenectomy was not feasible. In addition, because the etiology of this mass remains unknown, resection of the mass should respect rules of surgical oncology even though malignant spleen tumors are extremely rare in children. In the second clinical case, the lesion was located on the lower pole of the spleen and was measured to be 3 cm in diameter, allowing easier for LPS within an experienced surgeon. An approximately 5 cm suprapubic transversal incision was done to extract the spleen specimen without fragmentation and avoiding any fluid spread. In both cases, no recurrence of the lesion was reported after 8 and 6 years of follow-up, respectively. Effectively, laparoscopy splenectomy studies in children revealed no recurrence after follow-up.2 6
According to literature, patients treated by LPS are at low risk of serious complications, such as overwhelming postsplenectomy infection.4 Within an experienced surgeon, LPS shortens length of hospital stay, reduces medical expenses with fewer wound complications and offers better cosmetic outcomes. Among the existing literature, no serious short-term or long-term complications have been reported after LPS. Therefore, we believe that when possible, LPS should be regarded as the first-line treatment of SANT in children.
Acknowledgments
We thank patients and their parents for allowing us to publish these case reports.
Footnotes
Contributors IS conceived the study and drafted the manuscript. RY, CES and PC Christian participated in surgery. RPY has been involved in drafting and critical revision of the manuscript. PC has revised the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Study ethics approval was obtained on 05 August 2020 (CECIC Rhône-Alpes-Auvergne, Clermont-Ferrand, IRB 5891).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available on the network database (cristal net) of the Department of Pediatric Surgery, Children’s Hospital, University Hospital of Grenoble.