Article Text

Abstract
Background Empty scrotum may be due to many reasons; besides true undescended testis these are monorchia, retractile testis, atrophy of testis due to torsion and ectopic testis. The location of testis in an aberrant site after passing through the inguinal canal and leaving it via external ring is a condition called ectopic testis. The most common aberrant locations of ectopic testes are superficial inguinal pouch (Denis Browne pouch), within anterior abdominal wall, perineum, femoral canal, contralateral scrotum (transverse testicular ectopia) and prepenile area.
Methods Description of management of five different cases of ectopic testes over a period of 10 years’ experience in pediatric surgery have been done with review of the literature about this rarity.
Results Five different cases of ectopic testes were as follows: infants 3 months of age with right ectopic testis in anterior abdominal wall near anterior superior iliac spine, 4 months of age with left perineal testis, 6 months of age with an ectopic femoral testis on left side, 8 months of age with transverse testicular ectopia on left side and 10 months of age with right true undescended testis and left perineal testis.
Conclusions Search for ectopic sites of testes should always be in mind during examination of patients with empty scrotum. Early surgical repair of ectopic testes is recommended, as there is no chance of spontaneous correction to the normal location. Long-term follow-up is necessary due to relatively high incidence of infertility and malignant transformation. Surgeons should be aware of the rare possibility of transverse testicular ectopia in cases of inguinal hernia with impalpable testis on the contralateral side.
- Empty scrotum
- undescended testis
- ectopic testis
- orcheopexy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Several causes of an empty scrotum other than undescended testis.
Ectopic testis is rare entity in pediatric surgical practice.
Ectopic testis is frequently missed during management of empty scrotum with impalpable testis.
What are the new findings?
The ectopic sites of testes should be kept in mind in every case of impalpable testis even in anterior abdominal wall away from groin and genitalia.
Transverse testicular ectopia may be expected in cases of incarcerated inguinal hernia with contralateral undescended testis.
Early surgical repair is encouraged and no benefit of waiting for spontaneous descent of ectopic testes.
How might it impact on clinical practice in the foreseeable future?
The surgeon should do thorough examination looking for ectopic sites of testes when dealing with impalpable testis or before doing diagnostic laparoscopy for impalpable testis.
Introduction
Testicular descent is finished at childbirth and the two testes are usually found in the scrotum. About 3%–4% of term newborns and up to 30% of premature babies may have delayed testicular descent.1 The testis may fail to drop down totally and stops at some point along its typical way from retroperitoneum to scrotum, a condition called undescended testis (cryptorchidism). Cryptorchid testis may be seen in the abdominal wall, within inguinal canal or in prepubic region, but there might be several other reasons for an empty scrotum other than undescended testis including anorchism, retractile testis, atrophied vanished testis after torsion and ectopic testis.2
Relocation of testis in an atypical site after going through the inguinal canal and leaving it through the external ring is named ectopic testis. The most widely recognized aberrant locations are superficial inguinal pouch (Denis Browne pouch), perineum, femoral canal, contralateral scrotum (transverse testicular ectopia (TTE)) and prepenile area.3 4 Ectopic testis happens in just 5% of instances of empty scrotum.5
The superficial or shallow inguinal pouch (a pocket shaped by scarpa and external oblique fascia near outer inguinal ring) is a common indwelling site for ectopic testes.6 Perineal ectopic testis is usually evident by palpating the testis in the perineum, it is seen roughly in 1% of all instances of undescended testes and the first case was reported in 1786 by John Hunter.7 TTE ‘crossed ectopic testis or testicular pseudo-duplication’ is a condition when the two testes slip through the same inguinal canal and situated in one hemiscrotum, or sometimes the patient presents with unilateral non-palpable testis and contralateral inguinal hernia in which both testes are in one hernial sac,8 9 and usually the diagnosis in such case is made intraoperative. The other rare sites of ectopic testis like the femoral canal, prepenile and retro vesical ectopic testis have also been reported.2
This paper aims to highlight the significance of doing perfect clinical examination in every case of testicular maldescent or empty scrotum looking for ectopic sites of testicular positioning.
Case presentations
Case 1
An infant 3 months of age was referred by pediatrician to my clinic with an unusual palpable mass in the lower lateral abdominal wall on right side for suspicion of enlarged inguinal lymph node, a detailed history and careful physical examination showed a healthy infant with an empty and poorly developed right hemiscrotum, normally located contralateral testis, the mass was mobile, non-tender, solid in consistency and away from regional distribution of inguinal lymph nodes. The parents were told that their baby might be having ectopic right testis. After sonographic confirmation of the aberrant location of right testis at anterior superior iliac spine, surgery was decided at this age to relocate the testis in scrotum. Surgical exploration was done via right inguinal incision tracing the spermatic cord reaching the testis which was embedded deeper to fascia near anterior superior iliac spine, it was of good size and with adequate length of vas and vessels so orchiopexy was done with ease in the subdartos pouch of right hemiscrotum (figure 1). A follow-up of this patient for 6 months reveals no complication with normal looking location of both testes in scrotum.

(A) Ectopic right testis in anterior abdominal wall near anterior superior iliac spine. (B) Delivery of ectopic testis via inguinal incision. (C) Right orchiopexy with closure of inguinal wound.
Case 2
Parents of an infant 4 months of age were advised by the nurse to visit a doctor because of accidental finding of non-palpable left testis in scrotum during circumcision procedure since the age of 3 months. When the parents consulted me, there was impalpable left testis neither in the scrotum nor in the inguinal canal with retracted underdeveloped hemiscrotum. An oval-shaped soft tissue mass was detected in the perineum (figure 2), a clinical diagnosis of perineal ectopic testis was suggested and confirmed by an ultrasound examination. Operation was offered and surgical exploration was performed through left inguinal incision, the spermatic cord was delivered to the wound, the testis with its gubernaculum was released from its attachment to the perineum, gently delivered into the inguinal wound and fixed in the ipsilateral scrotum using dartos pouch technique (figure 2). Postoperative follow-up after 2 months revealed a normally located left testis in the scrotum and the parents were satisfied with the outcome of surgery.

(A) Palpation of left ectopic perineal testis. (B) Intraoperative delivery of ectopic testis with sufficient length of cord. (C) Left orchiopexy in sub-dartos pouch.
Case 3
A mother accidentally noticed during bathing her neonate at the age of 10 days that there is no left testis in scrotum with palpation of abnormal lump in the inner aspect of upper thigh. At age of 2 months the parents consulted a pediatrician who diagnosed the case as left undescended testis and referred the baby to a general surgeon. The surgeon reassured the parents, advised to monitor for spontaneous descent with a trial of hormonal therapy for this undescended testis after age of 6 months. The parent consulted me because they refused hormonal therapy. During examination, there was empty left hemiscrotum with palpation of a testis-like mass at an abnormal position between the penoscrotal raphe and the genitofemoral fold and it was really outside the normal pathway of testicular descent (figure 3). An ectopic femoral testis was confirmed by an ultrasound examination and surgical intervention was performed successfully via left inguinal incision and orchiopexy was done in the subdartos pouch of left hemiscrotum.

Left ectopic femoral testis.
Case 4
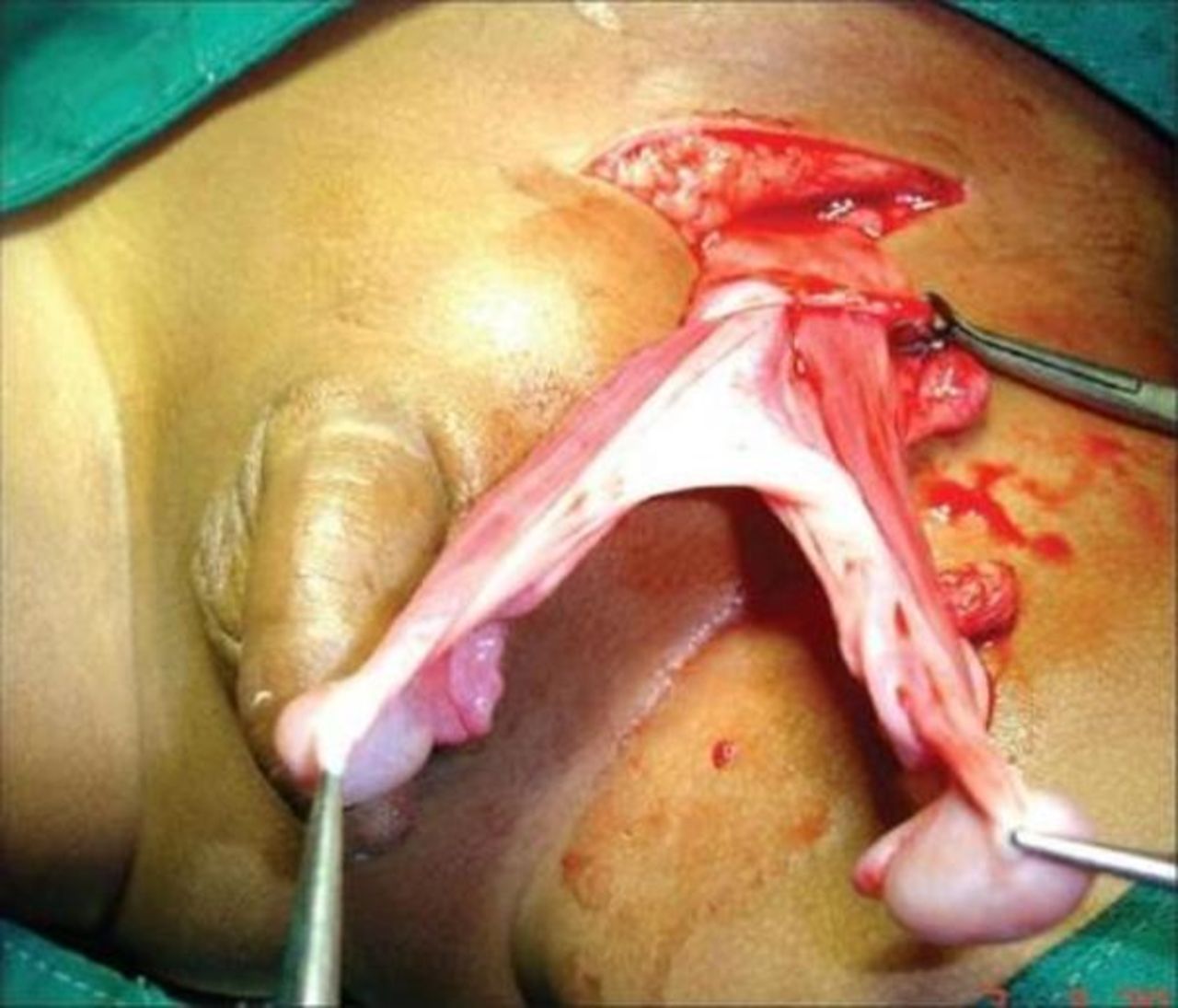
An infant 8 months of age was admitted to emergency department with incarcerated left inguinal hernia. After a trial of unsuccessful manual reduction, the baby was taken into theatre for surgical exploration during which we discovered an empty right hemiscrotum and both testes were located in the left inguinal canal at the level of external inguinal ring with two separated vasa deferentia but partially fused proximally (figure 4). A diagnosis of TTE was made intraoperatively, the hernia sac was separated and tied high up, both testes were brought down to scrotum through the same incision and trans-septal orchiopexy was performed.

Transverse testicular ectopia with fused vas deferens.
Case 5
An infant 10 months of age was diagnosed as a case of bilateral undescended testes since neonatal life and kept on observation and follow-up. He then received pregnyl hormonal therapy (human chorionic gonadotrophin) 100 IU/kg twice weekly for 2 months. After that, the right testis was palpable in the upper inguinal canal but the left testis was impalpable. A diagnostic laparoscopy was offered for this patient after explanation to parents. During thorough physical examination of external genitalia under general anesthesia before laparoscopy, a surprising soft tissue mass was palpated in the perineum (figure 5) and then confirmed by ultrasound to be an ectopic left perineal testis, bilateral orchiopexy was then performed via inguinal approach with satisfactory results.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Right undescended testis with left perineal testis.
Discussion
The development of testes and their descent from abdomen to scrotum pass through complex stages, it begins from 7th week of gestation and usually completed at 35th week. Several androgenic hormones and certain mechanical factors control the normal migration of the testis.10 It has been proposed that calcitonin gene-related peptide (CGRP) liberated from the genitofemoral nerve will provide a chemical gradient and hence indirectly promote growth of the gubernacular tip leading to its movement and progress in the right direction toward the scrotum.11 Normally, the testis follows the course of scrotal extension of gubernaculum and any disturbance in this process leads to maldescent. The testis that is stopped at some point within its normal pathway is true undescended testis while the testis that follows one of the other tails of the gubernaculum to an aberrant pathway is termed ectopic testis. Another rare congenital anomaly that must be kept in mind as a cause of undescended testis is splenogonadal fusion, especially when there is unusual scrotal mass or when there are associated anomalies.12
In spite of the several suggested theories trying to explain the occurrence of testicular ectopia, its clear etiology remains unknown. These theories focused on different concepts like gubernacular abnormalities, genitofemoral nerve disorders, endocrine disorders and intra-abdominal pressure.13 The ‘Tails hypothesis of Lockwood’ is the most famous one, he suggested that there are several tails of insertions extended from inferior gubernaculum so the normal descent will lead to scrotal insertion as dominant one. If the other insertions are more potent and larger during the transinguinal phase of testicular descent, the testis will be dragged in wrong direction and lodged in an aberrant location to be ectopic.14 15
Hutson suggested that abnormal position of genitofemoral nerve leads to an abnormal movement of the gubernaculum and pushes the testis to abnormal position.10 The chemotactic gradient resulted from hormone imbalance between androgen and CGRP released by the genitofemoral nerve play important role in testicular descent as it acts as a guide to gubernacular progress.4 16 On the other hand, Middleton et al17 suggested that the normal descent of gubernaculum is facilitated by increased intra-abdominal pressure and in case of inadequate pressure there will be testicular ectopia.17 18
Various hypotheses have been proposed to clarify the development of TTE,17 Berg proposed that both testes develop from the ‘same germinal ridge’.19 Kimura accepted that if the two vasa deferentia emerged from one side, there had been one-side root of origin however on the off chance that there were two-sided origins, one testis will be crossed over.20 Gupta proposed that during early development there is cohesion and coalition of Wolffian ducts and that descent of one testis made the 2subsequent one pursue.21 Frey also noticed that TTE might be due to defect in gubernacular development on the ipsilateral side.22 Indeed, the pathogenesis of TTE still stays misty.
Ectopic testis can be found at five different sites, these are femoral canal, suprapubic region, perineum, opposite side of the scrotum and anterior abdominal wall.3 4 Some authors include the superficial inguinal pouch (Denis Browne pouch) as a site of ectopic testis (about 75% cases of testicular ectopia),20 but others put it under the name of undescended variant, as they notice that a testis located at the superficial inguinal pouch behaves as a true cryptorchid testis regarding histological changes and response to hormonal therapy.6
Perineal
Ectopic testis is seen very rarely in pediatric surgical practice with approximately 175 reported cases in the literature, the majority of these cases are unilateral.21 We encountered two cases of perineal testis out of five reported cases of ectopic testis, both were on the left side, so the palpable soft tissue mass in perineum on the same side of an empty hemiscrotum perineum is very suggestive of ectopic testis. Surgical exploration for perineal ectopic testes is usually done through inguinal approach as a standard but some surgeons prefer low scrotal approach. The hernia sac was not identified in our patient and we found that gubernaculum is fixed to the perineum so the testes are placed in ipsilateral hemiscrotum easily without retroperitoneal dissection because of adequate length of the testicular vessels and vas deferens.
The anterior abdominal wall is exceptionally variant site for ectopic testis. The deviation of a testis from its typical course of descent to a location in the anterior abdominal wall cannot be clarified on embryological basis,23 it might be because of entrapment of a testis in spigelian hernia, or because of neonatal omphalitis that compellingly pulled the testis upward during ensuing healing.24 True undescended testis is commonly associated with indirect inguinal hernia, the same thing is noticed with ectopic testis. Siddiqui et al15 and Haseeb et al16 reported the association of anterior abdominal wall testes with ipsilateral inguinal hernia in their cases, during their open groin exploration they found that the testes were migrating between fat planes and muscles of the abdominal wall so they performed herniotomy with subdartos orchiopexy. Nevertheless, Yeap et al25 reported a case of abdominal ectopic testis without any hernia, similarly in our case report 1, there was no association of hernia with ectopic testis.
Since the first description of TTE by Lenhossek in 1886 until 2008, >100 cases have been reported in literature as claimed by Naouar et al. There are three types of TTE according to the presence of associated anomalies:
Type I (50%) associated with inguinal hernia.
Type II (30%) associated with persistent or rudimentary Müllerian duct structures.
Type III (20%) associated with other disorders (inguinal hernia, hypospadias, pseudo-hermaphroditism and scrotal abnormalities).
Patients with TTE usually present with right ectopic testis with clinical signs of inguinal hernia on contralateral side or sometimes present with incarcerated hernia.5 26 The diagnosis of such case is usually made during exploration for inguinal hernia and it is very difficult to made preoperatively. Nevertheless, some articles stated that it can be diagnosed preoperatively by ultrasonography of an experienced sinologist or by CT and MRI.27 28 In this paper, we presented intraoperative diagnosis of TTE on left side (case report 4) after trial of unsuccessful manual reduction for incarcerated left inguinal hernia (type I TTE). Vascular structures and vas deferens of the testicles might be separated or united; TTE associated with fused vas deferens is extremely rare. This condition may prevent the testis from being placed into the scrotum easily during orchiopexy.29 There were two options for management of TTE; either extraperitoneal orchiopexy or trans-septal orchiopexy,30 which is recommended in case of fused vas deferens like our case when we traversed the testis across the scrotal septum and fixed in the proper contralateral side. While in the extraperitoneal approach, the testis is released from its surroundings and passed near root of penis to be located in the contralateral hemiscrotum.
Ideally speaking, when two gonads have been encountered on one side during inguinal surgery, complete evaluation of abdominal structures should be performed through diagnostic laparoscopy or mini laparotomy for detection of Müllerian structures and any associated congenital genitourinary abnormalities, a biopsy should be taken from gonads or any tissue remnants.
In spite of the fact that patients with TTE are at expanded danger of threatening histological changes and malignant transformation like seminoma, embryonal carcinoma, teratoma and yolk sac tumor,31 there is no reported case of malignancy arising from the retained associated Müllerian structures, and the absence of Mullerian inhibitary factor (MIF) does not seem to be additional risk factor of testicular malignancy. Therefore, hysterectomy is not indicated routinely for every patient with TTE and obvious retained Müllerian structures as excision of structures will add risk of extra injury.32
Although an ectopic testis is uncommon condition in pediatric surgical practice, it should not be disregarded in cases of void scrotum. Appropriate clinical examination should be done in warm and relaxed surroundings beginning by putting one finger on each side of scrotum neck to prevent the testes from being withdrawn out of the scrotum. Each side of the scrotum is then palpated for presence of testis; in case that is not there, the fingertips are put just medial to the anterior superior iliac spine and moved firmly toward the pubic tubercle where the other hand holds back to catch the testis if it shows up.
The ectopic location of the testes make them vulnerable to a number of complications like trauma, torsion, infertility and malignancy. The association of ectopic testis with a contralateral undescended testis (as in our case report 5) suggests that ectopic and undescended testes are variants of the same congenital anomaly, having the same pathological findings with increased incidence of subfertility and testicular malignancy.3 Although the complications of ectopic testes are the same as for undescended testes, the timing of surgery should be different; there is no need to delay surgery in ectopic testis and surgery is indicated even if there is no hernia present. Any attempt to move the ectopic testes into the scrotum with hormone therapy have been found to be ineffective.20
Conclusion
A careful search for ectopic sites of testes should be fundamental part of clinical examination of patient with an empty scrotum. Easiness of the operative procedure for such cases recommend early surgical repair when diagnosed, as there is no chance of spontaneous correction to the normal location. Long-term follow-up is necessary due to relatively high incidence of infertility and malignant transformation. Surgeons should be aware of the appropriate intraoperative surgical management when they unexpectedly identify two testes on one side during inguinal exploration. They should keep this rare clinical entity in mind, in cases of incarcerated inguinal hernia with contralateral undescended testis.
References
Footnotes
Contributors AEJ participated sufficiently in contributing to the intellectual content, concept, design of this work, data acquisition, analysis and interpretation of the data. AEJ also contributed in writing of the manuscript, critical revision and takes public responsibility for it. AEJ is the corresponding author responsible for making necessary changes as per the request of the journal.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work. No data are available.