Article Text

Abstract
Objective To evaluate the effect of inguinal hernia (IH) on the spermatic cord using spermatic cord ultrasonography (SCU).
Methods From January 2016 to January 2017, boys with IH who received SCU at the start of open herniorrhaphy (OH) were enrolled in this study. The age and weight at SCU, width of the spermatic cord (SC-W), peak systolic velocity (PSV) in the spermatic artery (SA-PSV) and velocity in the pampiniform plexus (PP-V), and the interval between the initial and the second OH in boys with metachronous inguinal hernia (MIH) were recorded, and the relationship among them was studied. Boys with unilateral IH comprised the IH group, and boys with MIH comprised the MIH group. Boys with polydactylism served as the control. One-way analysis of variance tested the differences among groups. Spearman’s r tested the relationship between SC-W in the MIH group and the interval.
Results A total of 80 boys were enrolled in this study (IH group 29, MIH group 26, and control group 25). SA-PSV and PP-V in the hernia side were faster and slower than the control, respectively. There was no significant difference in PP-V and SA-PSV of the treated side in the MIH group and in the control group. After herniorrhaphy, SC-W was tapered down to normal size. SC-W, SA-PSV, and PP-V in the treated side were all highly correlated to the interval in a curvilinear manner.
Conclusion PSV was positively correlated with SC-W in boys with IH, and PP-V was negatively correlated; herniorrhaphy could reverse the impairment.
- spermatic cord ultrasonography
- metachronous inguinal hernia
- inguinal hernia
- herniorrhaphy
- peak systolic velocity
- velocity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- spermatic cord ultrasonography
- metachronous inguinal hernia
- inguinal hernia
- herniorrhaphy
- peak systolic velocity
- velocity
Introduction
Pediatric inguinal hernia (IH) is the most common congenital defect in daily practice. An IH or hydrocele may impair testicular blood flow, and preoperative testicular blood flow in the hernia-sided testicle is significantly reduced compared with the normal-side testicle.1–3 Fortunately, the blood flow is normalized through herniorrhaphy.3 As far as we know, no previous study has investigated the blood flow of hernia-sided spermatic cord. Thickened spermatic cord that accompanies IH in boys is well documented, but whether herniorrhaphy can reverse this phenomenon is unknown yet.4 The effect of IH on the spermatic cord is still unclear. Ultrasonography is a safe and non-invasive method to visualize and evaluate the spermatic cord,5 6 so we evaluated the effect of IH on the spermatic cord using spermatic cord ultrasonography.
Methods
From January 2016 to January 2017, boys aged 1–2 years with IH who received an ultrasound examination at the start of open herniorrhaphy in the operation room of the Department of Ambulatory Surgery were enrolled in this study. The age and weight at spermatic cord ultrasonography, sonographic width of the spermatic cord, peak systolic velocity (PSV) in the spermatic artery (SA-PSV) and velocity in the pampiniform plexus (PP-V), and the interval between the initial and the second open herniorrhaphy (interval) in boys with metachronous inguinal hernia (MIH) were recorded, and the relationship among them was studied. Boys with initial unilateral IH comprised the IH group, and boys with MIH comprised the MIH group. Twenty-five boys with polydactylism served as the control.
Spermatic cord ultrasonography
Both sides of the spermatic cord were examined by one radiologist (attending doctor) and her assistant (fellow) in the operation room of the Department of Ambulatory Surgery using a 7.5 MHz linear transducer at the start of open herniorrhaphy. The radiologist was blind to the clinical diagnosis, but her assistant was not. Grayscale ultrasound was performed to show long-axis section of the spermatic cord, then color Doppler flow imaging was performed to show the flow signal with the scale adjusted to 2 mm/s. The cremaster muscles were clearly shown (hypoechoic by grayscale ultrasound). At the external ring, we measured the diameter between the inner edges of the cremaster muscles. The diameter of the cord was recorded. The velocities of the spermatic artery (the largest one) and the pampiniform plexus were measured by pulse wave Doppler (PWD). SA-PSV and PP-V were also recorded at the external ring level.
Open herniorrhaphy
The procedures were performed under caudal anesthesia combined with intravenous anesthesia. Briefly, a small transverse dermatoglyphic incision was made on the hernia side, and then the Scarpa’s fascia was spread. The external oblique was kept intact and the cord was identified near the external ring. As soon as the sac was identified and opened, and the deferent duct and vessels were bluntly separated toward the neck of the sac. Then, the sac was only doubly ligated without resection, and the thickness of the empty sac was measured. Finally the incision was closed with one single suture.
Statistical analysis
Continuous data are expressed as mean±SD and were analyzed using one-way analysis of variance (ANOVA) followed by least significant difference (LSD). Logistic regression was used to assess the association between the width of the treated side spermatic cord, SA-PSV and PP-V and the interval, respectively. Spearman’s rank correlation coefficient (Spearman’s r) was used to examine the relationship among the width of the spermatic cord, the interval, and velocities of spermatic vessels. P<0.05 was considered statistically significant. Statistical analyses were performed with SPSS (IBM SPSS Statistics V.22).
Results
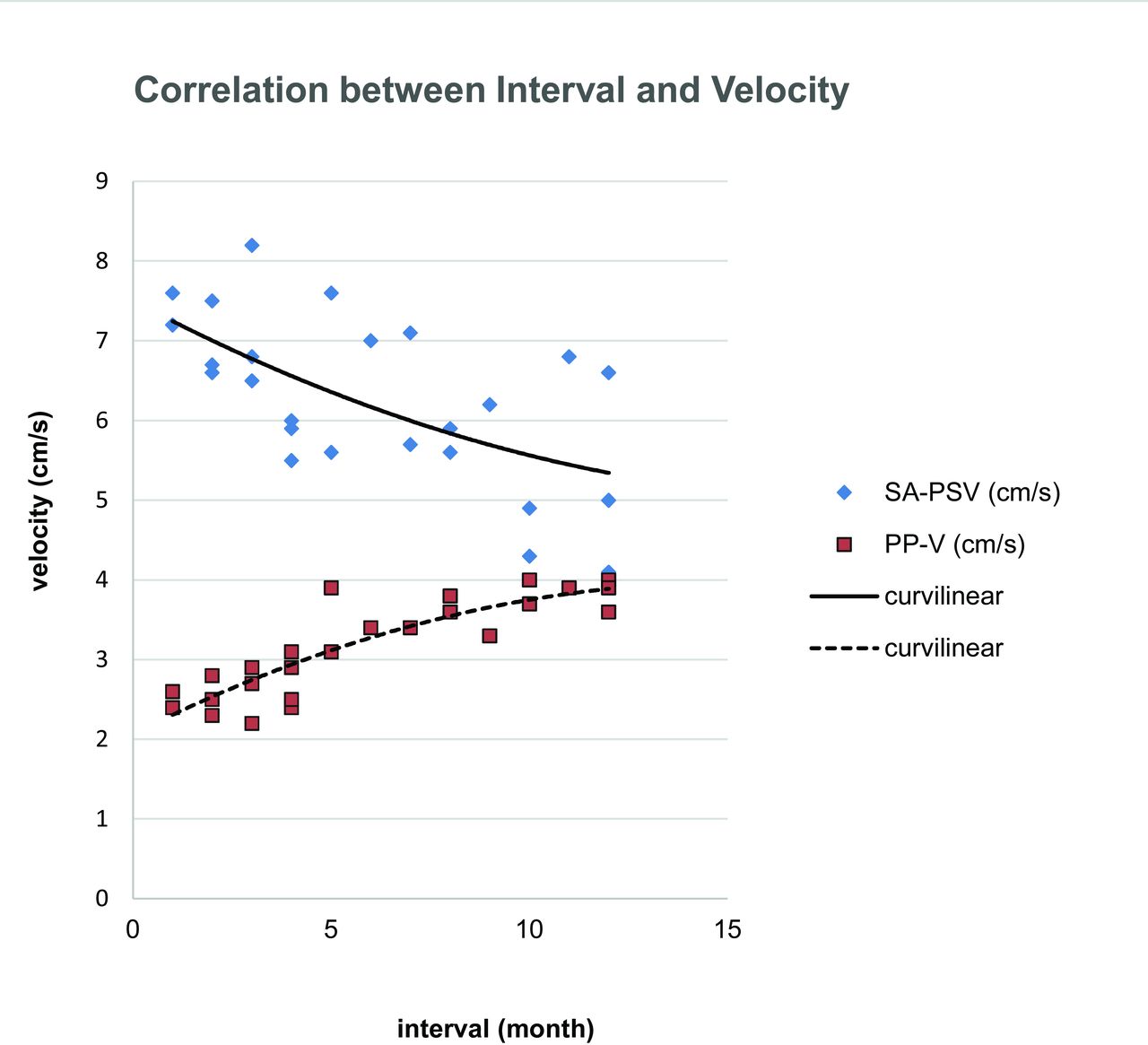
A total of 80 boys were enrolled in this study (IH group, n=29; MIH group, n=26; and control group, n=25). The age and weight at spermatic cord ultrasonography were not significantly different among the groups (table 1). The sonographic widths of hernia-sided spermatic cord of the IH group, normal side of the IH group, treated side of the MIH group, and the control were 0.61±0.12 cm, 0.14±0.04 cm, 0.25±0.11 cm, and 0.15±0.04 cm, respectively (one-way ANOVA, p<0.001). Significant differences were identified in SA-PSV and PP-V, respectively, among the groups (one-way ANOVA, p<0.001). Furthermore, SA-PSV in the hernia side of the IH group (7.90±2.07 cm/s) was faster than the control group (6.48±1.92 cm/s; LSD following one-way ANOVA, p=0.002), in the normal side (5.60±1.55 cm/s) was slightly slower than the control (LSD following one-way ANOVA, p=0.055), and there was no significant difference in SA-PSV between the treated side of the MIH group (6.27±1.02 cm/s) and the control (LSD following one-way ANOVA, p=0.650). PP-V in the hernia side of the IH group (2.75±0.65 cm/s) was slower than the control (3.24±1.13 cm/s; LSD following one-way ANOVA, p=0.036), there was no significant difference between the normal side (3.68±1.03 cm/s) and the control (LSD following one-way ANOVA, p=0.057), and there was no significant difference in PP-V of the treated side of the MIH group (3.17±0.59 cm/s) and the control group (LSD following one-way ANOVA, p=0.752) (table 2). Following herniorrhaphy, the widths of the treated side spermatic cord, SA-PSV, and PP-V were all associated with the interval in a curvilinear manner (r2=0.833, p<0.001; r2=0.317, p=0.005; and r2=0.748, p<0.001, respectively) (figures 1 and 2). SA-PSV, PP-V, and the width of the spermatic cord was highly correlated to the interval (Spearman’s r=−0.581, p=0.002; r=0.865, p<0.001; and r=−0.902, p<0.001, respectively). SA-PSV and PP-V was highly correlated to the width of the spermatic cord (r=0.621, p=0.001 and r=−0.790, p<0.001, respectively).
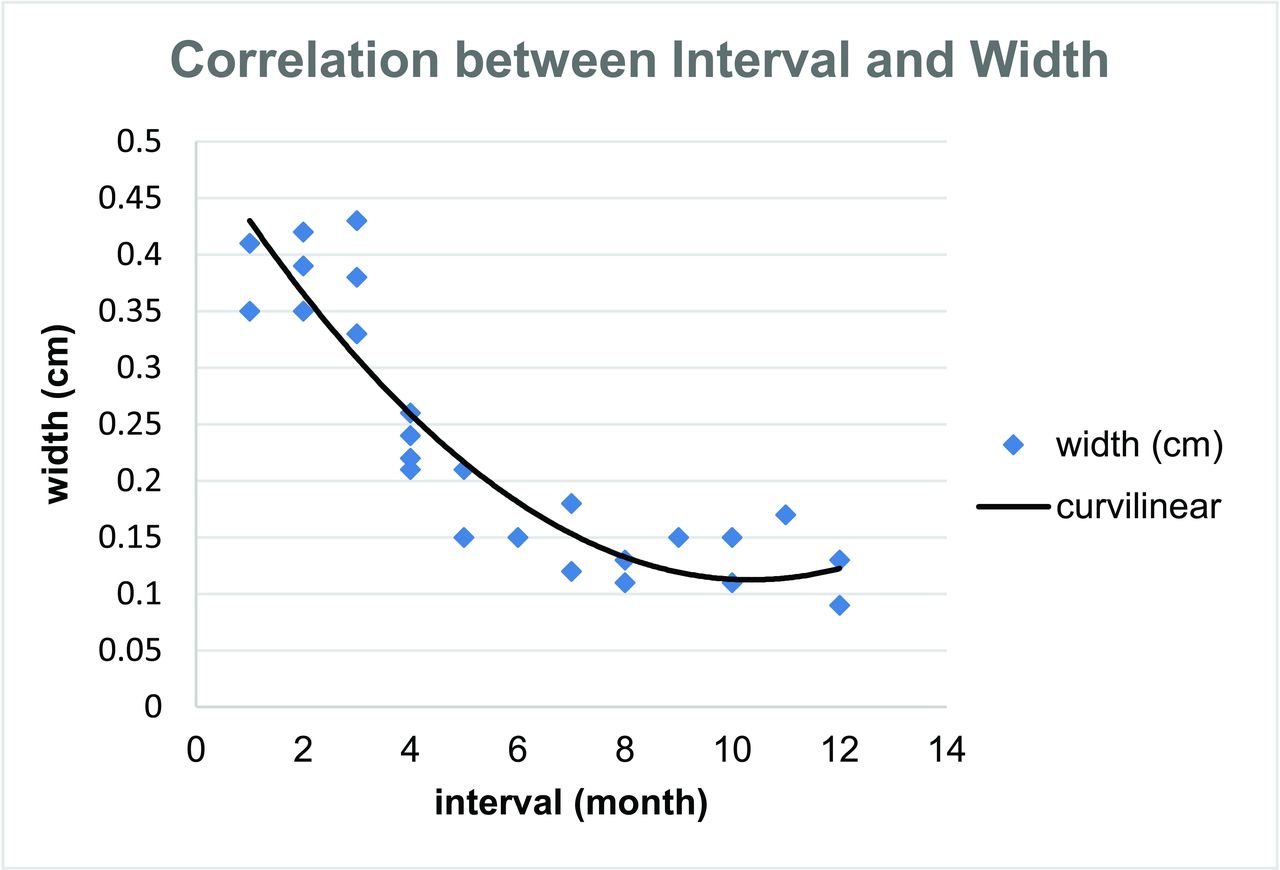
Correlation between the interval during the initial and the second open herniorrhaphy and the width of the treated side spermatic cord.

{kind=link}
{kind=link}
Correlation between the interval during the initial and the second open herniorrhaphy and blood flow of the treated side spermatic cord vessels. PP-V, velocity in pampiniform plexus; SA-PSV, peak systolic velocity in spermatic artery.
Comparison of age and weight among groups
Comparison of velocity in spermatic cord vessels (cm/s) among groups
Discussion
The spermatic cord is composed of the pampiniform plexus, testicular artery, cremasteric artery, artery of the ductus deferens, lymphatic vessels, testicular sympathetic nerves, tunica vaginalis, or hernia sac, and the ductus deferens all run deep to the internal spermatic fascia.7 The cord is invested completely with cremasteric muscle and fascia. At the external ring, the cord is characterized by numerous external spermatic veins and multiple spermatic arteries,8 9 so it is convenient to use ultrasonography to evaluate the thickness and blood flow of the spermatic cord at the external ring level.
Cremasteric muscle hypertrophy accompanies IH in children in the manner of fiber size variation and increase in perimysial connective tissue.10 11 Therefore, we measured the diameter between the inner edges of the cremaster muscles of the cord. Except for cremaster muscles, our observation found that the hernia-sided spermatic cord was still thickened, and spermatic cord thickening could gradually reverse after herniorrhaphy. The amount of smooth muscle was greater in the hernia sac group where it appeared as a layer; and in contrast, the smooth muscle present in the form of sparse bundles around the connective tissue in the processus vaginalis.12 The sac was only doubly ligated without resection, and the thickness of the sac was less than 2 mm (data not shown), measured during surgery. So the content between the cremaster muscles and the sac contributed to the thickening, and the spermatic vessels were the major constituent of the content.
The tendency of testicular ischemia in infants with IH is mostly due to vascular structures where there is no rich collateral vessel network of the testicle.13 14 The hernia content in a relatively narrow inguinal canal could trigger an intermittent mechanical compression effect on the spermatic cord; furthermore, inflexible superficial inguinal ring might lead to congestive testicular infarction with venous obstruction, especially in infants.2 3 So we hypothesized that reducible inguinal mass that caused an intermittent mechanical compression effect on the spermatic cord would impair blood flow of the spermatic cord.
Our investigation confirmed the hypothesis. At the external ring level, we used PWD to measure PSV in the biggest artery and PP-V. In the hernia side, SA-PSV became faster and PP-V became slower. According to anatomical physiology, the testis receives blood supply primarily from the testicular artery, except for the artery to the vas deferens and the cremasteric artery.7 15 After herniorrhaphy, PSV and PP-V reversed gradually. This finding was consistent with previous studies, except that they tested testicular blood flow.3 16
Our study has a very interesting finding, showing that SA-PSV and PP-V in the treated side of the MIH group were highly correlated to the width of spermatic cord. After herniorrhaphy, SA-PSV could gradually slow down with time and PP-V could gradually quicken accompanied with tapering down of the width of the treated side spermatic cord. Further investigations should be carried out to reveal the mechanism underlying the correlation between thickness and blood flow of the spermatic cord.
To the best of our knowledge, this is the first study to reveal the correlation between thickness and blood flow of the spermatic cord in boys with IH. PSV was positively correlated with the width of the spermatic cord and PP-V was negatively correlated; herniorrhaphy could reverse the thickening and impairment of blood flow of the spermatic cord.
Acknowledgments
The authors acknowledge all surgeons, anesthetists, and ultrasound physicians who contributed to data collection, and the ward staff who contributed to providing and caring for study patients.
References
Footnotes
Contributors SH and XY: study conception and design; CL, XY and DW: data acquisition; JL: analysis and data interpretation; SH: drafting of the manuscript; SH and DW: critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This retrospective study was approved by the Institutional Review Board of the Children's Hospital, Zhejiang University School of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.