Article Text

Abstract
Objective Patella fractures in children are rare, with an incidence of less than 1% of all pediatric fractures. Literature describes different surgical techniques and outcomes, but there is not a specified superior technique for children. The aim of this study is to assess the functional outcome after screw fixation of transverse patella fractures in children.
Methods Two boys at 11 years of age were presented with a transverse fracture of the patella within the same week. Open reduction and fixation of the fractured patella with periost sutures and a 4.0 mm titanium screw inserted from the distal fragment. Afterward, the quadriceps expansion was meticulously repaired with sutures.
Results The patients could fully weight bear immediately on a fully extended knee in an orthosis. After 4 weeks, radiological healing was obtained. At the 8-week and 6-month follow-up, the modified Hospital of Special Surgery knee score was 100 points in both patients.
Conclusion Single screw fixation provides an excellent outcome after 8 weeks with a full range of motion and full weight bearing, providing a faster recovery.
- patella
- fracture
- transverse
- pediatric
- osteosynthesis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Two cases of transverse fracture of the patella were reported, both with a clear mechanism of injury and both treated operatively with screw fixation. Radiological follow-up was evaluated and the modified Hospital of Special Surgery (HSS) knee score was assessed. Our clinical results are promising and patient satisfaction is high.
Introduction
Patella fractures in children are uncommon with an incidence less than 1% of all pediatric fractures.1 The low incidence of patella fractures in children may be due to the fact that the osseous portion of the patella is less subject to both impact and tensile forces in children than in adults, because of a thick layer of cartilage and periosteum surrounds and protects in case of direct impact together with softer and more flexible ligament. Thus, more laxity protects the patella from fractures.1 As with adults, the different types of fracture are caused by various accident mechanisms: direct blow, sudden contraction of the extensor mechanism, or a combination. Known patella fracture patterns in children are those of transverse or comminuted fractures, osteochondral defects and sleeve fractures. Sleeve fractures being the most common one followed by transverse fractures.2 3 Despite the differences in patella and the tensile forces between children and adults, the treatment protocol for children and adults are the same.4 Restoration of the extensor mechanism and realignment of the articular surface are essential.3 5 The most common treatment is by open reduction and internal fixation. Various techniques have been used for transverse and sleeve fractures, such as tension band wiring and absorbable anchor sutures. The evidence regarding patella fracture treatment in children is very weak. Only few studies describe the use of single screw fixation of transverse fracture.6 We believe that transverse patella fractures in children can be treated with a better outcome and with less complications by using a single cannulated 4.0 mm titanium screw with a washer. The aim of this study is to assess the functional outcome after screw fixation of transverse patella fractures in children.
Case presentations
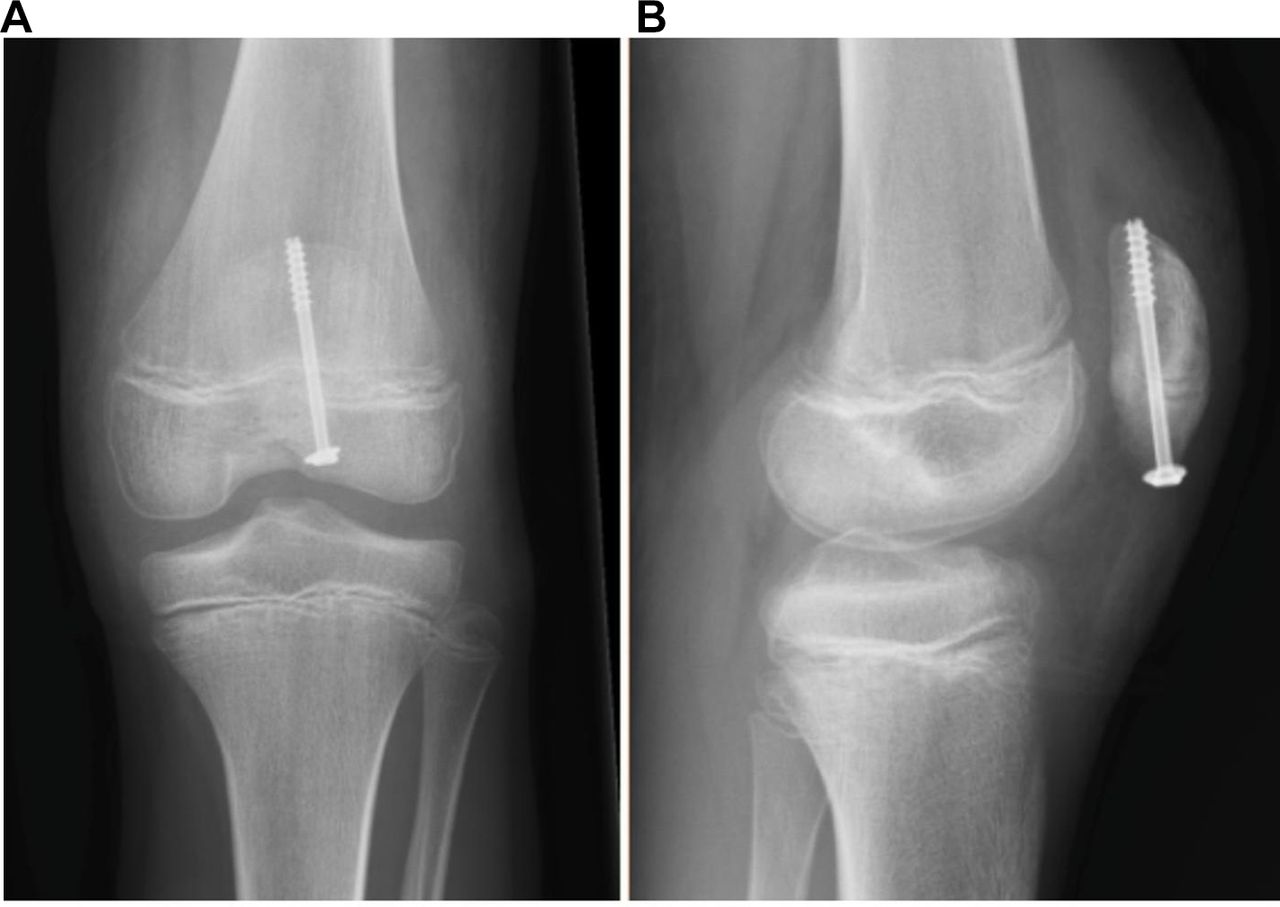
Two boys of 11 years of age were presented to the emergency department within the same week. Both boys were normal in their development and physically active on a daily basis before the injury; thus, a specified HSS score preinjury at 100. Both had a direct trauma of their left knee and experienced pain and swelling right after injury, difficulty in standing and weight bearing and increasing pain trying to do so. Examination findings showed a significantly limited range of movement and while lying down it was impossible for the patients to elevate a fully extended leg. One patient had a minor superficial wound treated with four stitches and antibiotics preoperative until surgery. Radiograph (both anterior–posterior and lateral views) showed displaced, transverse fracture (figure 1). Time to surgery was 1 and 2 days, respectively. During general anesthesia, the collateral and cruciate ligaments were found to be stable. Open reduction was performed using a vertical 5 cm midline incision while using tourniquet (25 and 35 min, respectively). Periosteum was removed and pulled out of the fracture and patella was reduced by a reduction forceps. The fractured patella was fixed with a 4.0 mm half treated titanium screw (Asnis, Stryker; Stryker Global Haedquarters, 2825 Airview Boulevard, Kalamazoo, Michigan, USA) with a washer, inserted from the distal fragment (figure 2). The screw penetrated just through the proximal cortex. Afterward, the quadriceps expansion and periosteum were meticulously repaired with sutures. A single shot of antibiotics (intravenous) was given prior to the surgery and in one of the cases 7 days (orally) after the operation due to a superficial wound.

Preoperative radiographic. (A) Lateral view and (B) anteroposterior view.

Perioperative radiographic. (A) Anteroposterior view and (B) lateral view.
The outcome was evaluated by patient examination, radiographs, functional tests and a questionnaire using the modified HSS knee score7 after 8 weeks and 6 months. The functional test included one-leg stand, squatting, lifting of the extended leg and sports abilities.
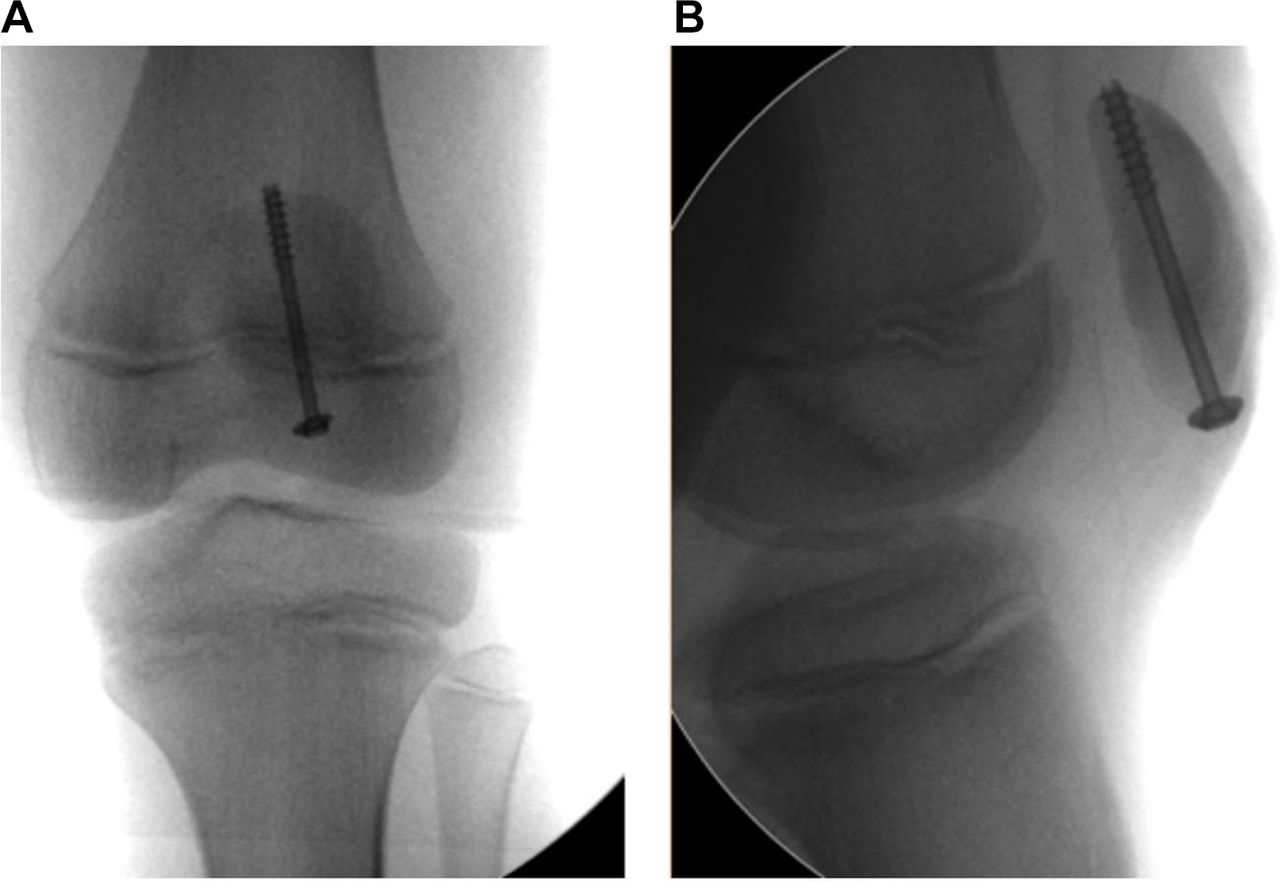
The time needed for operative stabilization was 48 min and 38 min, respectively. After surgery, our patients were immediately allowed weight bearing with the knee immobilized in extended position and after 4 weeks full movement was allowed. No infections were identified. After 4 weeks, radiological healing was obtained (figure 3). After 8 weeks, there was no pain or tenderness and no swelling. There was no limping, the range of motion was identical to the contralateral knee except a less than 5° flexion deficit in one of the cases and we found full ligament stability. No patella dislocation or signs of meniscal tears were found. At the 8-week and 6-month follow-up, the modified HSS knee score was 100 points in both patients. After 2 years, none of the cases have had any complications.
{kind=link}
{kind=link}
{kind=link}
Postoperative radiographic. (A) Anteroposterior view and (B) lateral view.
Discussion
To our knowledge, fractures of patella in children are sparsely mentioned in the literature. The evidence for different surgical techniques of patella fractures is weak regarding adults8 9 and even weaker for children. Only a few studies describe the treatment in children and all are retrospective. Dai and Zhang1 described four cases of transverse fractures in children. One treated by tension band wiring, the rest fixed with a circumferential wire or suture loop. They did not describe surgery time, time to mobilization, complication rates or postoperative range of motion. Schmal and colleagues6 described retrospectively the treatment of 23 patella fractures in children and adolescents. Eleven fractures treated by immobilization in a cast or brace without operation, 12 patients operated using tension band wiring, screw osteosynthesis, fixation with biodegradable pins or transosseous sutures. No specification on subgroup of transverse fractures operated with screw osteosynthesis. The time needed for operative stabilization was 73±29 min (range 42–132 min). No infections were noted after operative treatment. Schmal and colleagues6 found, after an average of 40 months, for transverse fractures a HSS score of 86. We have not found any other study describing patients weight bearing and mobilized as fast as ours after surgery, or a functional score of 100 points this early.
The most common complication to fixation by tension band is postoperative pain due to symptomatic fixation implants and reoperation due to removal of osteosyntering. The literature does not describe complications after surgery in children, and therefore the complication rates in adults are presented. Lazaro and colleagues10 reported 11 out of 30 (37%) patients requiring removal of symptomatic hardware. LeBrun and colleagues reported11 14 out of 27 (52%) requiring secondary surgery due to symptomatic implant and 5 of 13 (38%) with retained implants reporting anterior knee pain, an average in these three studies is 42%. Even though complication rates of secondary removal were lower in children, we assume that a considerable number of children treated with tension band wiring or circumferential wire will have to undergo a second surgery for hardware removal. Using screw fixation this will presumably not be necessary. The washer is placed close to the bone deeply into the patella tendon, and therefore the potential discomfort from the hardware is minimized. Reducing the number of secondary operations will improve the outcome for the individual patient and furthermore being an economic incentive.
This method is suitable for sleeve fractures in children as well, if the osseous/cartilage fragment is large enough to support the screw with washer. We believe that, due to the lower tensile forces, the thick periosteum, meticulously restoration of the extensor retinaculum by sutures and the faster healing time in children, fixation by a single screw is strong and stable. Our case report highlighted the excellent outcomes provided by the single screw fixation in transverse patellar fractures in children, including early restoration of knee motion and full weight bearing.
The advantages of this method compared with other surgical alternatives and conservative methods includes, fast recovery, high functional outcome and less risk of secondary surgery due to hardware removal.Despite the successful fixation described, considering the skeletal immature subjects, we suggest this surgical method should be used cautiously. A future comparative multicenter study is required to support an improved treatment protocol for transverse and sleeve fractures of the patella in children. In our study, the follow-up time was too short to observe any disturbances of patella growth and potential cartilage damage. The small sample size is a weakness. However, due to the very low incidence and lack of focus in the literature, we find our study is relevant to pediatric trauma surgeons. The fact that we do not have a control group in this study is a limitation, but due to the rarity of the fracture type, this was not possible.
Footnotes
Contributors All listed authors have contributed sufficient to the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.