Article Text

Statistics from Altmetric.com
Congenital esophageal stenosis (CES) is a rare anomaly with an incidence of 1 per 25 000–50 000 live births.1 Patients with CES often present early in life with dysphagia and poor weight gain due to reduced intake of solid food. A stenosis higher and closer to the respiratory tract also produces respiratory symptoms, while lower lesions produce only abdominal symptoms. Although the symptoms start early during the weaning period, we report a case where the diagnosis was made in an 8-year-old child who presented to the outpatient department with dysphagia.
Case report
An 8-year-old male child visited the outpatient department with complaints of inability to swallow solid food. On examination, general condition and nourishment were good. The child was not anemic. Vital signs were examined and were normal. Examination of cardiovascular and respiratory systems did not show any abnormality. Examination of the abdomen was also normal. Upper gastrointestinal endoscopy was performed; however, the scope could not be passed beyond the lower one-third of the esophagus (figure 1). Esophagogram was performed following upper gastrointestinal endoscopy, which showed the presence of a long stenotic segment in the lower end of the esophagus (figure 2). The patient was then taken up for oral contrast CT, which again showed a long segment of stenosis in the lower end of the esophagus (figure 3). This resulted in the proposition of three differential diagnoses, namely CES, stenosis secondary to reflux esophagitis and achalasia cardia, and surgery was planned. After performing a right lateral thoracotomy in the sixth intercostal space, a dilated esophagus with narrowing and thickening of about 2.5–3 cm was found in the lower one-third. Fogarty catheter was inserted, inflated, and pulled up. However, the distal esophagus near the gastroesophageal junction was normal. The stenotic part was excised and an end-to-end anastomosis was done. Intercostal drain was kept and the wound was closed in layers.

The scope not passing beyond the lower third of the esophagus.

Esophagogram showing distal stenosis.

Oral contrast CT showing a long segment of the distal esophagus narrowed.
Ryle’s tube was removed on the day of surgery. Anastomotic leak was present on the sixth postoperative day. A feeding jejunostomy Stamm-type was done on the ninth postoperative day. Ryle’s tube was reintroduced under fluoroscopic guidance on the 19th postoperative day. Esophagogastroduodenal endoscopy showed esophageal narrowing noted at 21.5 cm and there was also an anastomotic dehiscence. Contemplating on the surgical procedure, we decided to proceed with endoscopic Niti-S esophageal stent. Esophagogastroduodenal endoscopy under fluoroscopy was done on the 33rd postoperative day. The scope could not be passed beyond 21.5 cm. A guidewire was passed under fluoroscopy and a self-dilating stent with flanges measuring 8 cm × 14 mm × 16 mm flanges was introduced through the guidewire. The stent was placed at the site of the anastomosis. The proximal end was kept at 16 cm. Postprocedure, the child was doing well. There were no leaks. The child began to take oral feeds, and the jejunostomy feeding tube was removed (figure 4).

Postoperative image showing the stent.
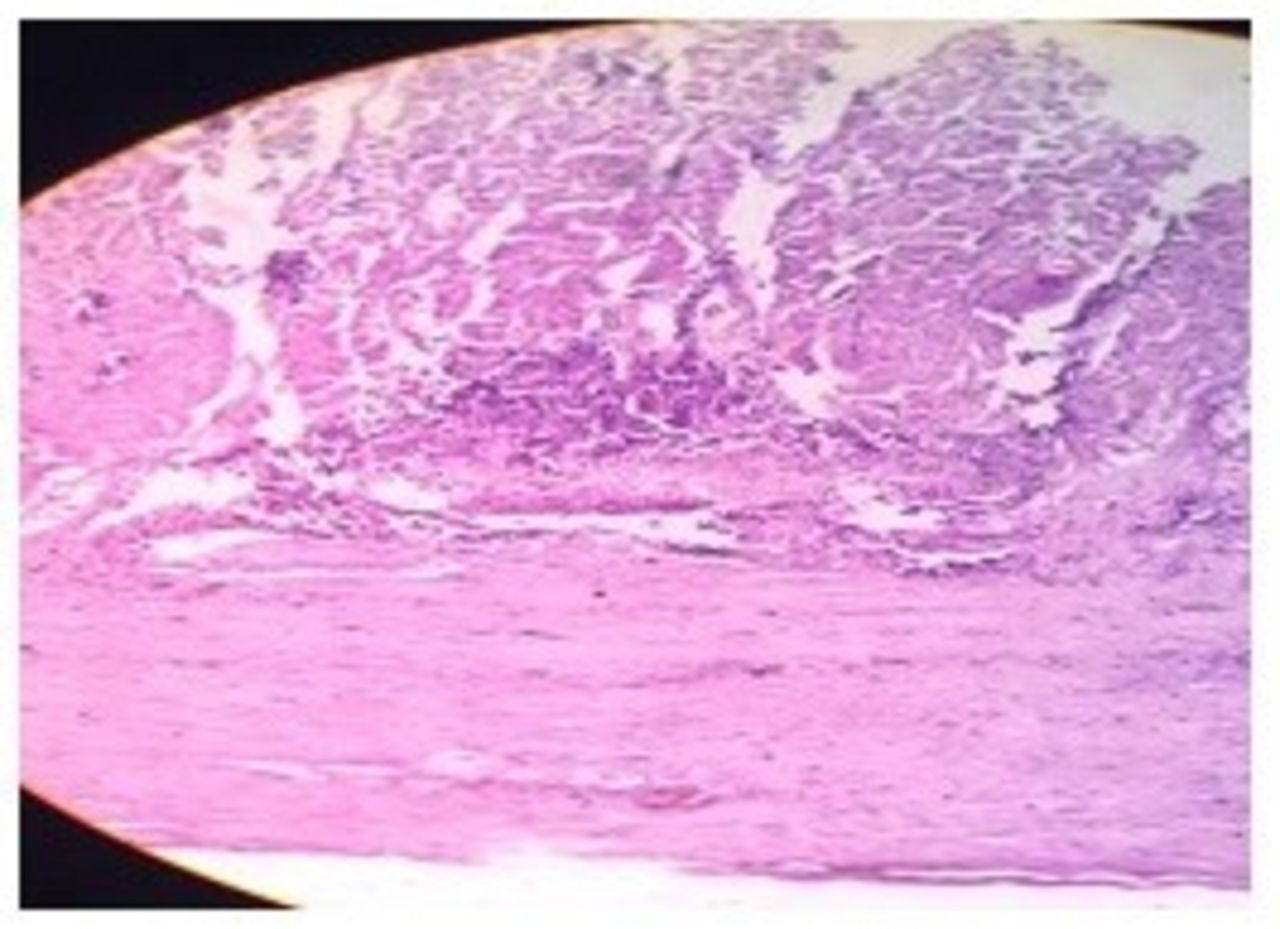
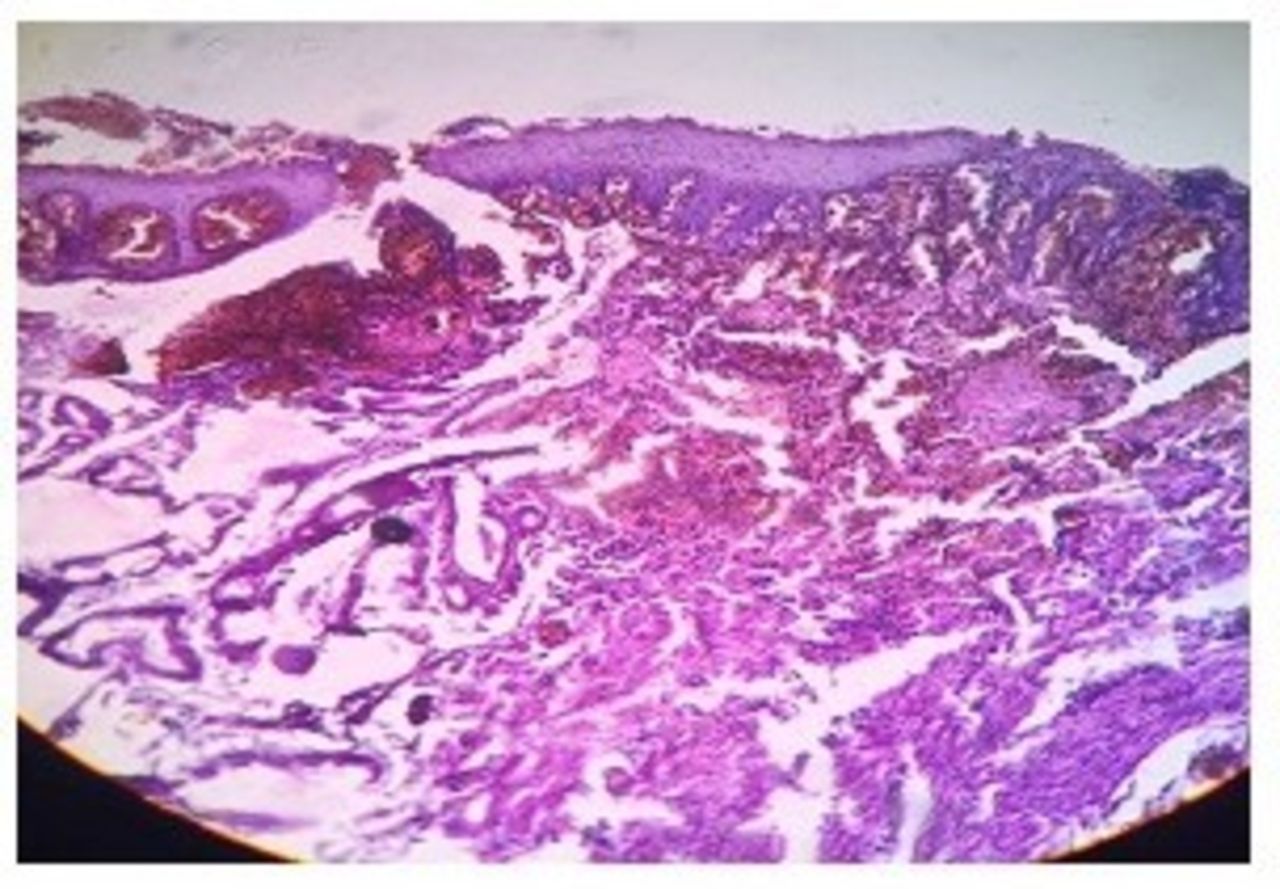
The excised fragment was sent for histopathologic examination. The gross findings reported the presence of a portion of esophagus with thickened wall with marked congestion of the external surface. The cut section showed complete loss of normal mucosa. The wall was rigid and thickened. The esophageal wall showed the presence of ulcer in the mucosa, hemorrhage in the submucosa layer, edema of the entire wall, and destruction of the smooth muscle layer by dense aggregates of inflammatory cells (figure 5). There was a complete loss of squamous epithelium replaced by inflammatory granulation tissue; expansion of the submucosa with dense bundles of collagen and fibrocytes was present. Loss of smooth muscle and neovascularization in the adventitial layer was also seen (figure 6). Dense aggregates of mononuclear inflammatory cells, disorderly arranged fibrous tissue and smooth muscle bundle were seen (figure 7). A very thick layer of fibrous tissue was found replacing the muscle layer (figure 8). There was no normal architecture in the upper portion.
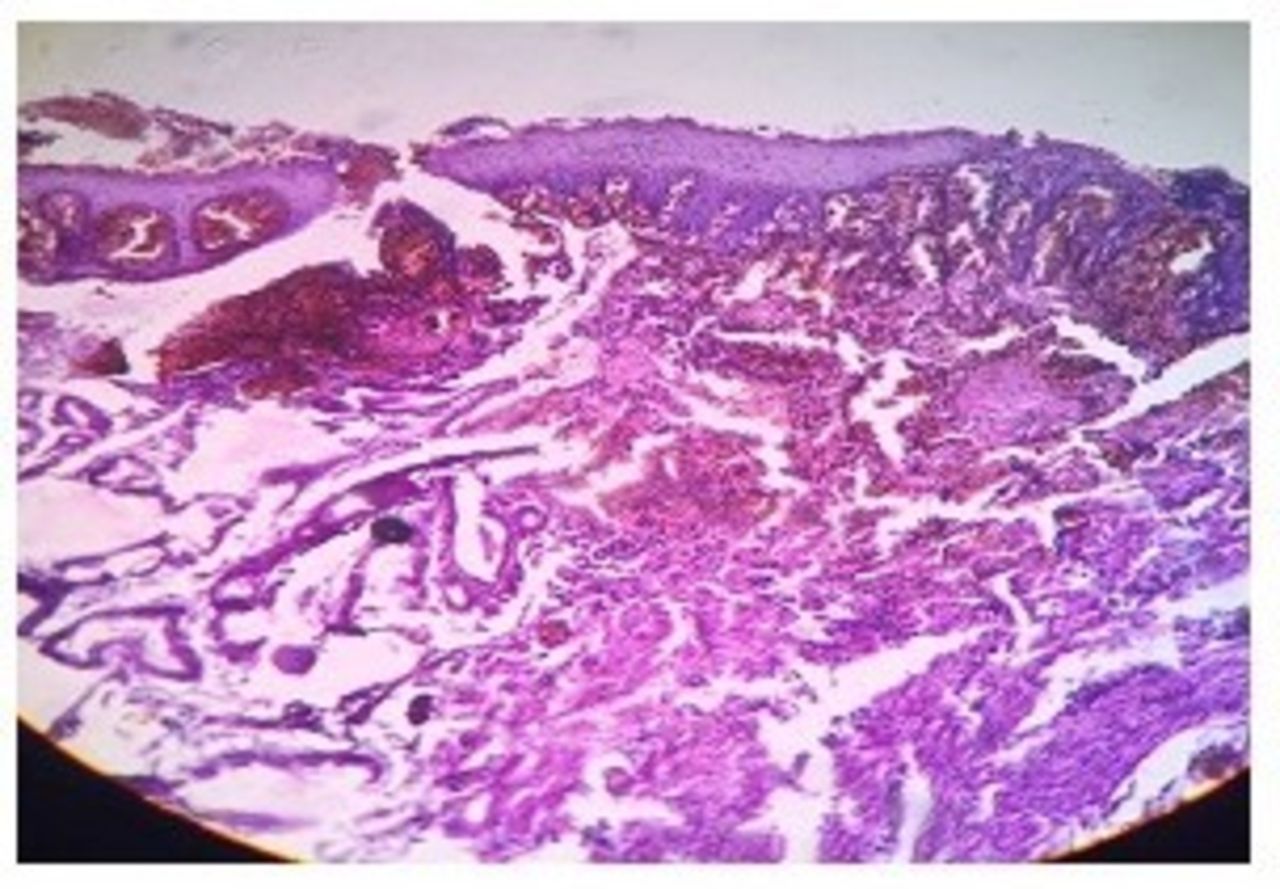
Histopathology showing the esophageal wall with ulcer in the mucosa, hemorrhage in the submucosa, edema of the entire wall, and destruction of the smooth muscle layer by dense aggregates of inflammatory cells.
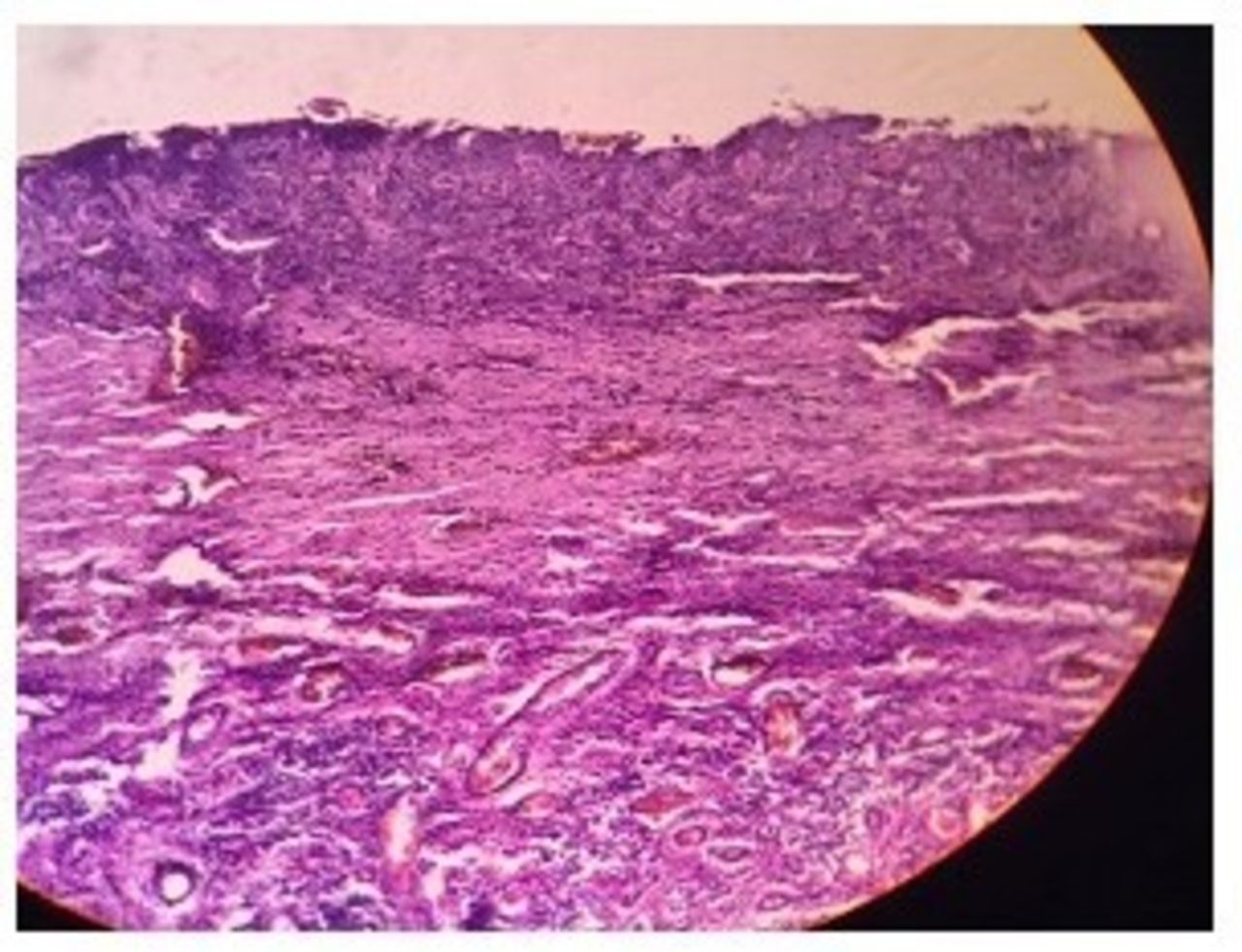
Complete loss of squamous epithelium replaced by inflammatory granulation tissue, expansion of the submucosa with dense bundles of collagen and fibrocytes, and loss of smooth muscle and neovascularization in the adventitial layer.

Dense aggregates of mononuclear inflammatory cells, disorderly arranged fibrous tissue and smooth muscle bundle.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A very thick layer of fibrous tissue replacing the muscle layer. In the upper portion, no normal architecture was maintained.
Discussion
CES is a congenital anomaly resulting from intrauterine stress or anoxia during the 25th day of life, leading to incomplete separation of the respiratory tract from the primitive foregut.1 The disease is said to have a slight predominance among males, although both genders are equally affected. The symptoms start presenting during the weaning period, after 4–6 months of life. In very rare cases, it presents in childhood and adulthood. CES is often said to be associated with other anomalies such as esophageal atresia, which has been reported in over 17% of cases.2
There are three anatomical types of CES: congenital web or membrane type, fibromuscular stenosis (FMS) type, and tracheobronchial remnants (TBR) type. The TBR type is said to be more common, involving the lower one-third of the esophagus.3 Despite several radiologic and imaging modalities that guide in the diagnosis, a confirmative diagnosis is made only postoperatively, after histopathologic examination. In older patients, achalasia cardia and esophageal neoplasms could also be possible differential diagnoses. However, the classic bird beak appearance in achalasia cardia is often absent radiologically. Moreover, the peristalsis is often absent or disorganized, accompanied by a vascular ring caused by double aortic arch due to bilateral and posterior compression of the esophagus.4
Some other modalities which help in the diagnosis include monitoring of pH and manometry. Endoscopic ultrasonography is useful in distinguishing the type of CES, apart from its gold standard use in visualizing the lumen and for presurgical assessments. CT shows diffuse circumferential asymmetric and non-enhanced wall thickening of the upper mid-esophagus or distal esophagus. MRI provides a more accurate diagnosis, showing diffuse circumferential and asymmetric wall thickening of the upper mid-esophagus or distal esophagus with intermediate signal.5
The management of CES varies with the type. The membrane type is best corrected by endoscopic dilatation or excision, while the FMS type can be treated by bougienage or dilatation. The TBR type can be surgically corrected by excision. Postoperative anastomotic leaks are best managed by endoscopic stent insertion. Intrathoracic leakage of esophagointestinal anastomosis is a devastating complication and a major reason for postoperative mortality. Persistent contamination of the mediastinum and pleural cavity results in complications such as mediastinitis, pleural emphysema, early sepsis, and septic shock. The mortality rates are as high as 60%–100%. Endoscopic stent implantation involves insertion of a self-expanding stent, a minimally invasive procedure that provides immediate sealing of the dehiscence. A self-expanding metal stent, Nitinol stent, 8 cm in length, is inserted between 6 and 12 weeks. The procedure is carried out using esophagogastroduodenal endoscopy with a ‘C’ arm guidance. The anastomosis is well achieved and is usually complete. The leak is reduced to 10%. The presence of esophageal anastomotic leak if any is treated conservatively/reopened.
Conclusion
CES is a rare anomaly with unknown etiology. It is often detected when the child presents with dysphagia, vomiting, and other gastrointestinal symptoms during the weaning period. The etiology of the disease remains unknown, although theories propose intrauterine stress and anoxia. There are several imaging modalities used to diagnose this condition. Surgical excision and dilatation remain the mainstay in the management of this rare condition. There is a growing need to explore the genes responsible for this disease so as to develop tools to detect the anomaly during the intrauterine period.
Footnotes
Contributors All authors have equally contributed to all aspects of the study and to manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.