Article Text

Statistics from Altmetric.com
Key messages
What is already known about this subject?
Fistula, meatal and urethral stenosis, and dehiscence are among the most common complications following the hypospadias repair.
Complications of hypospadias surgery increase with age during childhood.
Proximal hypospadias may be considered a separate entity because of its different repair techniques and varied outcomes.
What are the new findings?
Location of urethral meatal was the main independent predictor of the development of complications in distal mid-shaft hypospadias repair in toddlers.
Postsurgical infection at the repaired site may be followed by neourethrocutaneous fistula.
How might it impact on clinical practice in the foreseeable future?
Learning about the most important predictors of complications in hypospadias repair of early childhood—which may differ from later stages of life—can result in improvement in surgery outcomes.
Introduction
As a common congenital anomaly, hypospadias typically requires surgical repair during the early years of life. Hypospadias is a consequence of defective closure of the urethral fold and can be accompanied by chordee. Despite the fact that numerous procedures have been described, today the most common repair method for distal hypospadias is the tubularized incised plate urethroplasty (TIPU).1
Fistula, meatal and urethral stenosis, and dehiscence are among the most common complications following the primary repair of hypospadias.2 3 A central question in this field is to determine what preoperative or intraoperative factors are able to predict future complications. Identifying these parameters would allow the surgeon to assess the risks before surgery and can potentially lead to the development of new techniques to circumvent the adverse outcomes.
In the current literature, the prognostic factors useful in the management of hypospadias remain poorly defined, and a wide discrepancy exists regarding prognostic factors related to the urethral plate (UP) and other anatomical features.1 3–8 In the present study, we assess several possible prognostic factors for complications in a rigorous, homogenous series of toddlers with distal to mid-penile hypospadias cases, aged 1–3 years, and undergoing the first-time TIPU. Thereafter, we will briefly review the studies on the prognostic factors of this subgroup regarding the pertaining study methodologies.
Methods
This Institutional Review Board-approved study was performed prospectively on a cohort of children undergoing primary hypospadias repair using TIPU in a referral hospital within 12 months of the study. From a total of 420 consecutive patients of all ages with hypospadias, 101 cases were finally enrolled in the observational study according to the inclusion criteria. The inclusion criteria included the first-time TIPU cases of distal to mid-shaft hypospadias with an age between 1 and 3 years. The meatal location was determined visually, meaning that the orifice located in the proximal one-third of the penis was considered as proximal hypospadias. Based on Hadidi’s classification, we did not include glanular or coronal hypospadias in the study.9
The exclusion criteria were the coexistence of moderate to severe chordee, micropenis, or a history of hypospadias surgery or circumcision. Micropenis was defined as a dorsal length of a stretched penis less than 1.9 cm in length for a term infant or if the length was less than 2.5 SD below the mean. Chordee or ventral curvature (VC) was recorded visually with parents’ cell camera photos while erection or micturition at the first or second visit and most reliably and quantitively after performing the erection test before making skin incisions. Chordee was defined as a penile shaft curvature and is categorized based on its degree measured by a goniometer: mild (<30), moderate (30–45), and severe (>45) curvature.10
The variables were measured and the operations were performed by a single surgeon to remove potential interobserver variations in the measurements and observations and surgical outcomes. The largest point of UP was recorded as the width.
The evaluation was performed in terms of characteristics of the UP dimensions in erect and flaccid states, penile stretched length, glans characteristics, and chordee (figure 1). Subsequent acute events and postoperative complications during the follow-up period were carefully monitored and were recorded by collecting the data with the help of a survey based on Hadidi’s classification form.9 The Strengthening the Reporting of Observational Studies in Epidemiology cohort reporting guidelines were used to report the study results.11
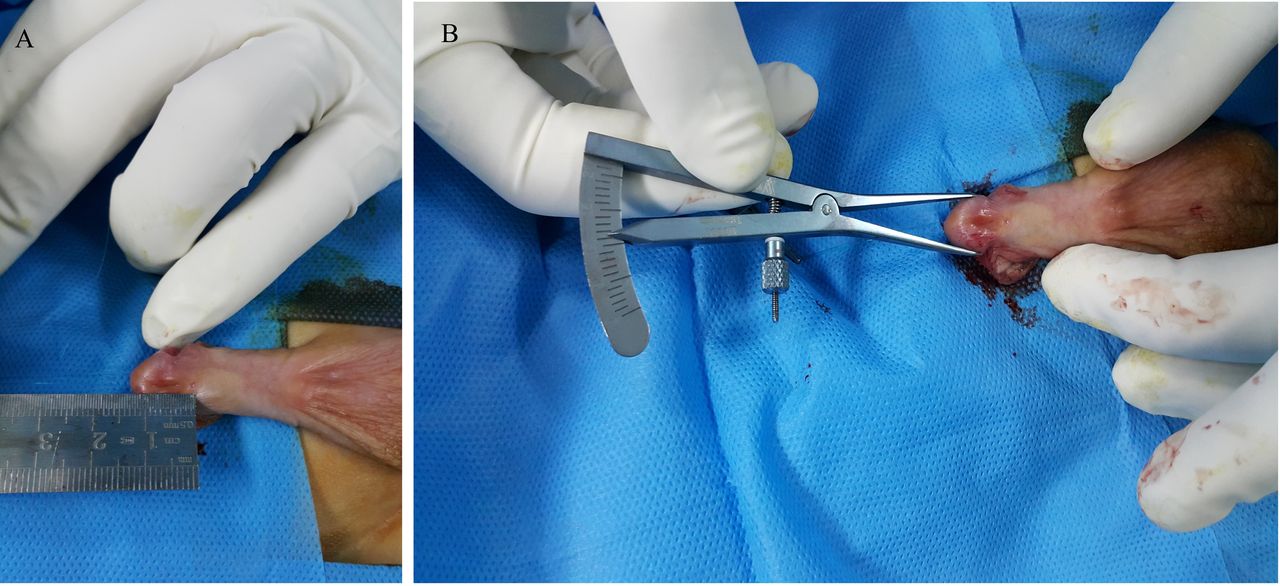
Measurement of (A) urethral plate length, (B) glans diameter.
Procedure
After the induction of anesthesia in the operation room, the diameter of glans, and the length and width of the UP were determined in both flaccid and erect conditions. Chordee was corrected by degloving, and ventral dissection of dartos and ventral tethering tissues as well as dorsal plication if needed. All patients underwent tubularized incised plate repair. The UP was tubularized over an 8 Fr Nelaton stent with a three-layer reconstruction using 5/0 polyglactin sutures. A ventral dartos flap was mobilized for additional coverage and secured on each side as the third layer. The skin was closed by subcuticular continuous 6-0 polyglactin stitches. Additional coverage of the glandular urethra was provided by using a separate dartos flap for glanular urethral protection. Two-layer closure of the glans wings was carried out for glanuloplasty. The neomeatus was reconstructed approximately 3 mm below the normal location. As a final step, we replaced the 8 Fr stent with a 6 Fr one. Postoperatively, the patients were dressed using Vaseline gauze, and for 7 days were provided with the stent as well as cephalexin while the catheter was in place. Surgeries were done by a single high-volume attending pediatric urologist. No kind of androgen was used. In the postoperative phase, emerging complications were divided into two categories: reversible acute events and persistent complications. Follow-up visits for the study were scheduled for 1 and 6 months after surgery. At the second follow-up visit, at least one of the parents was assessed regarding their cosmetic outcomes using a survey filled by healthcare professionals addressing parents’ overall perception regarding meatal location, shape, and general cosmetic appearance and also functional outcomes (voiding without splitting, spraying, or straining) with yes or no questions comparing their perception before and after repair.
Statistical analysis
All data analyses were performed with SPSS V.24.0 (IBM). The t-test and Fisher’s exact test were used to compare quantitative and qualitative variables, respectively, in univariable analyses. The UP width was assessed in two conditions: dichotomous variable and continuous variable (≥1 cm and <1 cm). Furthermore, a logistic regression model was used for multivariable data analysis to determine independent prognostic factors. P values <0.05 were considered statistically significant.
Results
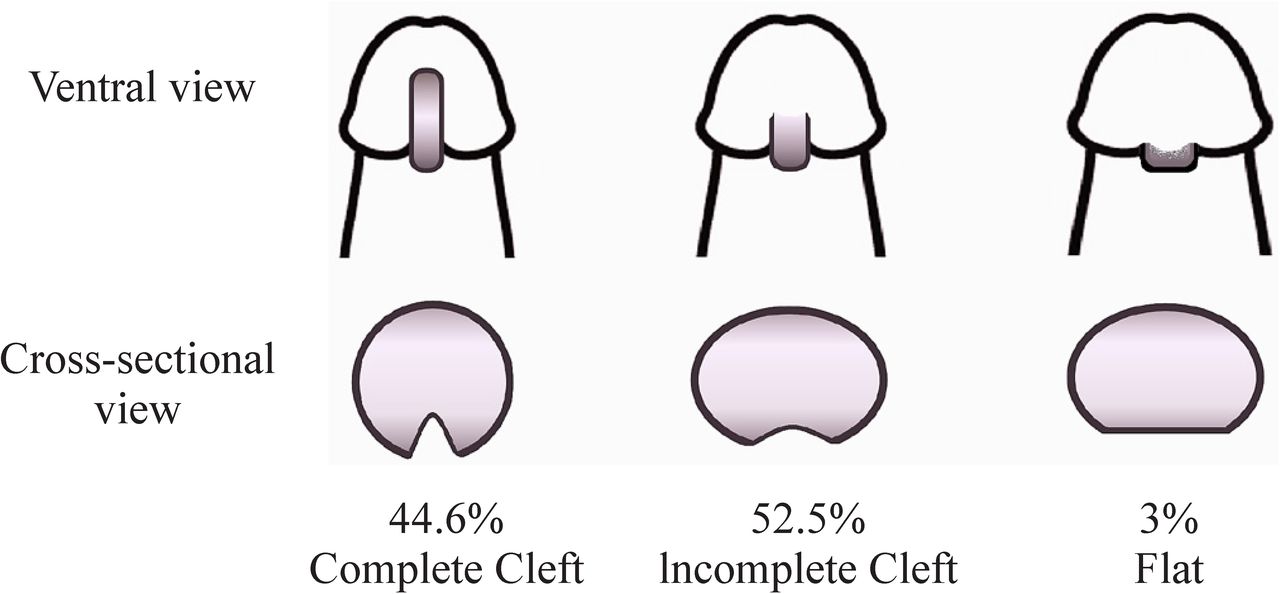
One hundred and one patients were included with the mean age of 19.86±8.60 months (range 12–36 months). Urethral meatus was located distally in 88 patients (87.1%) and at mid-shaft in 13 patients (12.9%) (figure 2). The mean dorsal length of the stretched penis was 22.99±4.03 mm (range: 15–32 mm). The median length of the penis at the ventral surface was 19.04±3.81 mm (range: 10–29 mm). Thirty-one patients had mild VC (30.7%). Glans was categorized in terms of depth of the shape and urethral groove by the visual qualitative measurement in the flaccid state into glans with a complete cleft (45 cases, 44.6%), an incomplete cleft (53 cases, 52.5%), and a flat group (3 cases, 3%) (figure 3).
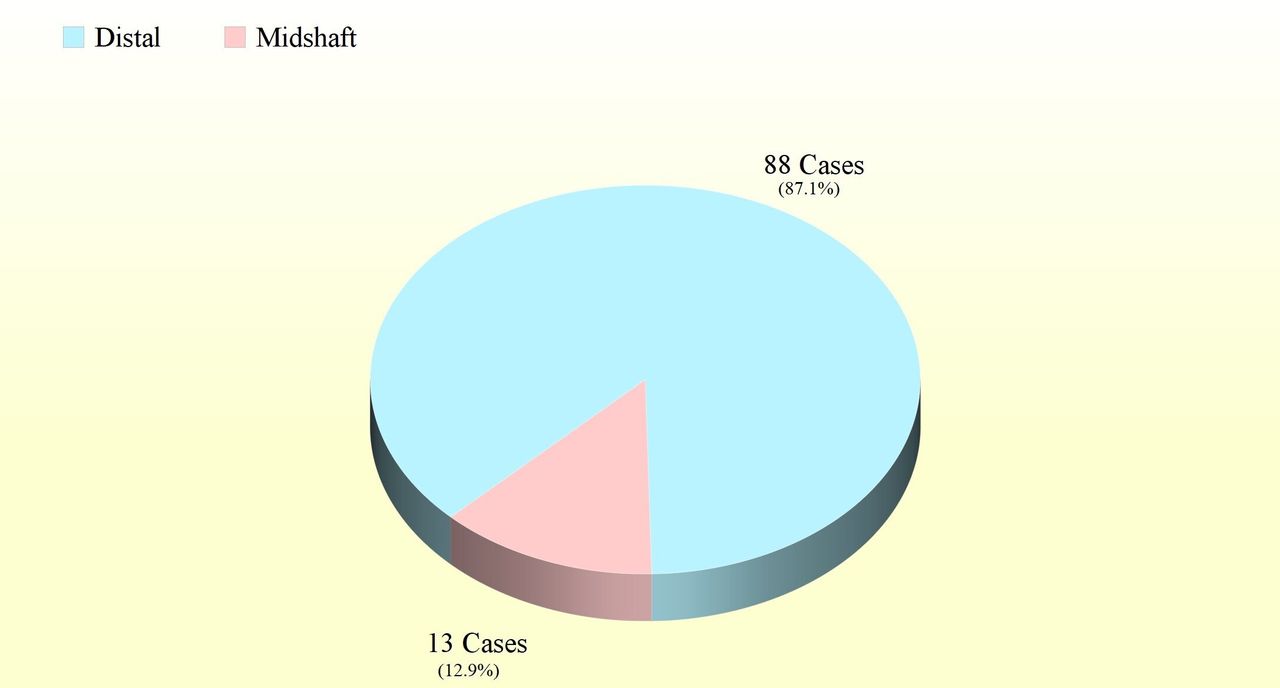
Prevalence of meatal locations in the study population.

Glans types according to the glanular urethral plate cleft and the prevalence in the study (figure illustrated by MRR).
The mean width of the UP was 9.51±2.50 (range 4–20) mm in flaccid condition and 10.59±2.62 (range 5–21) mm in the erect state. Accordingly, the width of the UP was less than 1 cm in 46 cases (45.5%) and 1 cm or more in 55 cases (54.5%). The mean length of UP was 10.52±2.88 (6–18) mm when erect and 11.86±2.41 (range 8–22) mm when flaccid. The mean diameter of glans was 17.18±3.08 (range 12–23) mm (when flaccid).
Postoperative findings
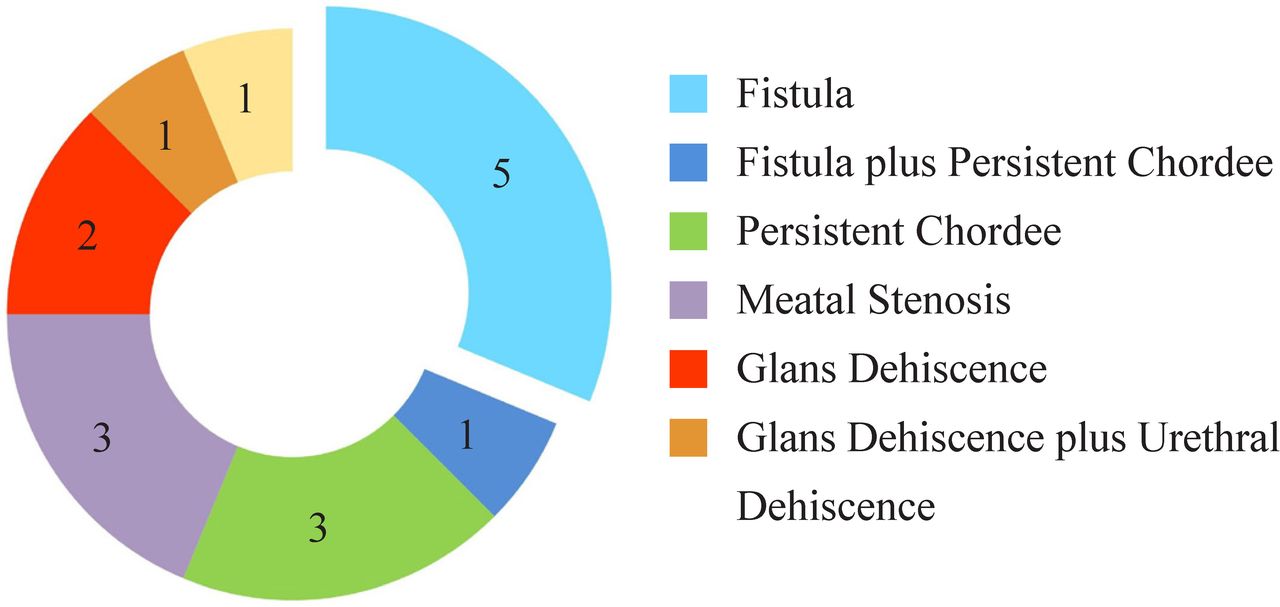
The mean length of the reconstructed UP was 12.42±2.51 (range 8–20) mm. The reversible acute events were observed in 42 cases (41.6%) including edema, erection, inadvertent removal of the urethral stent, surgical wound infection, bladder spasm (defined by a sudden and temporary urinary leakage), hematoma, or hemorrhage. The mean time to the development of acute events was 2.67±1.16 (range 1–5) days. Acute reversible events were considered different entities from persistent complications, which consisted of fistula formation, the persistence of chordee, meatal stenosis, glans, and urethral dehiscence. The mean follow-up time was 6.58±3.36 months. A total of 85 (84.2%) patients did not have any persistent complications, in contrast to 16 cases (15.8%), the most prevalent of which was fistula observed in five cases (3%). The cases with fistula, particularly larger ones accompanied with meatal stenosis, underwent reoperation around 6 months after the first surgery. Other complications included recurrent chordee, glans, urethral dehiscence, and ventral scarring of the glans (figure 4 and table 1).

Donut chart of complications and pertaining number of patients.
Presurgical findings and acute postsurgical events* in the complicated† (group 1) and uncomplicated (group 2) patients
Postoperative edema was seen in eight cases (7.9%) on the first day after surgery. This could be because of the interruption of lymphatic drainage during dissections. Dysuria and urinary tract infections (positive in urinary culture) were reported in 23 (22.8%) and 2 (2%) cases, respectively.
The study variables in the complicated and uncomplicated groups are compared and summarized in table 1. In the single-variable analysis, the width of the UP in the flaccid penis, length of UP in the erect penis, and location of meatus were significantly associated with the complications. The number of cases with distal meatus was significantly higher in the uncomplicated group (91.8% vs 62.5%, respectively, p=0.01%). Counterintuitively, the UP width was also reversely associated with the complications. The complicated group had a higher percentage of patients with a width of ≥1 cm (87.5% vs 48.2%, p=0.004). In all other measures, no statistical difference was observed in this phase of analysis (table 1).
In the multivariable analysis, to find independent risk factors for complications, the association of width of the UP was not significant (Relative Risk (RR)=0.94, p=0.61); neither was the length of the UP (RR=0.9, p=0.93). Only the location of the urethral meatus (orifice) was significantly associated with postoperative complications (RR=7.69, p=0.01). Postoperative acute events were not significantly associated with the complications (RR=0.25, p=0.06).
In patients with acute surgical site infection, four cases developed fistulas (50%), whereas in patients without acute infection the fistula was observed in two cases (2.1%). Fistula formation was found to be considerably notably higher in the group with acute surgical site infection (p<0.001) (figure 5).
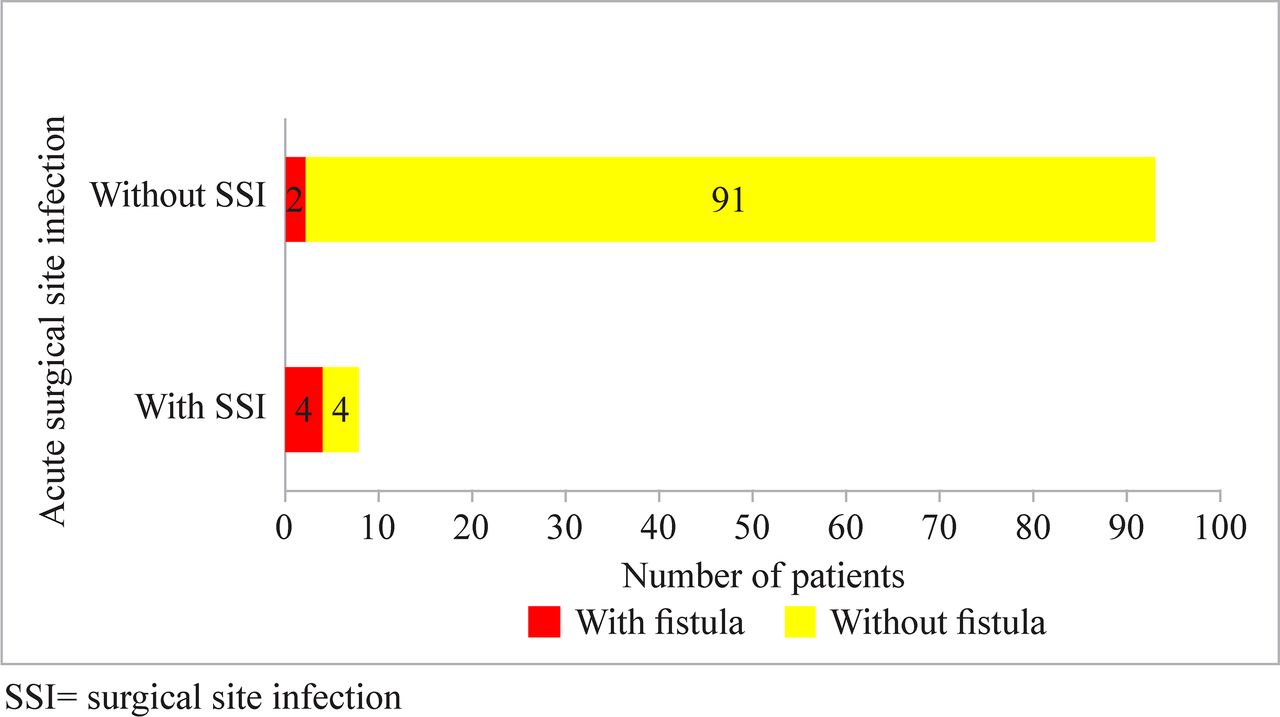
Surgical site infection (SSI) and future fistula development.
Discussion
Approximately 1 out of every 10–20 distal hypospadias surgeries develop a complication. Surgeons attempt to identify risk factors for complications to make modifications in techniques to improve their results.12 In the present study, we evaluated the results of the mid-shaft and distal hypospadias surgery in terms of potential factors predictive of complications. The persistent complications were noticed in 15.8% of our patients, which were within the range of previous studies (figure 6).13–17

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-chart of complicated and uncomplicated percentages in distal and mid-shaft hypospadias.
Fistula and surgical site infection
Fistula developed in six cases and wound infection in eight cases (figure 5). We found a significant association between fistula formation and surgical site infection (p<0.001). None of the fistula cases had meatal or urethral stenosis. Infection along with relatively low vascularity may result in poor wound healing and resultant fistula. Consequently, interventions that would reduce the infection rates can result in better outcomes.
Chordee
In terms of the presence of mild chordee, no significant differences were found between complicated and uncomplicated cohorts. Severe chordee cases were excluded from our study. Severe chordee (or penile curvature) can be indicative of underlying severe hypoplasia of corpus spongiosum, dartos, or Buck’s fascia in the urethral area, which suggests that the severity of hypospadias defect is more profound and blood supply is more limited to the area. For this reason, the existence of severe chordee per se may be a major risk factor for complications particularly fistulas, and more importantly may affect other variables in the study,18 which, similar to proximal hypospadias, may lead to undervaluing or obscuring the role of other prognostic factors.
Glans
Smaller glans can be accompanied by technical difficulties at the surgery. However, no significant differences in glans diameters or groove shapes (complete cleft, incomplete cleft, flat) were found between the two cohorts in our studies. This finding is consistent with a study by da Silva et al19 contrary to some others.20 21 One possible explanation for these discrepancies can be the variations in glansplasty techniques.12
Width
Contradicting results have been demonstrated in studies on the width of UP. Some studies have found the width of the UP to be directly associated with the development of complications.5 22–24 However, other studies have failed to find any significant associations.19 25–27 In our study, the width showed an association with complications in the single-variate analysis, but the association was not statistically significant in the multivariable analysis (p=0.61).
Meatal location as the single most important factor
In contrast to single-variable analysis, in the multivariable study the presurgical meatal location was the only factor associated with complications (p=0.03). Consistently, the closer the meatal orifice was to the coronal margin, the fewer the complications existed (RR=7.69, p=0.01). It is worth mentioning that marginal differences around this value (1.5 mm) might not be considered from the surgical technical point of view.
A brief review of prognostic factors in the current body of literature
Multiple studies have tried to identify prognostic factors for the development of complications. Studies on hypospadias outcomes in the current literature included a broad spectrum of ages, some of which with adult cases as well. It has been shown that complications can increase with age when comparing early childhood with late childhood.28 29 UP dimensions vary as age increases, and considerable changes develop in the UP structure. Older UPs consist more of collagen content, fewer cells, and elastic tissue and are depleted of vascular sinusoids.30 On the other hand, the extent of self-care (which may influence the surgical results) differs at different ages in childhood.
Furthermore, proximal hypospadias has been included in many studies. Proximal hypospadias as the severe form of the disease may be considered a separate entity because of its different outcomes, considerable variabilities in techniques, and higher complication rates.31 32 Moreover, only a few studies have used a single repair technique (eg, TIPU) for their study population.
Finally, the factors that studies have been investigated are various, and inability to perform multivariable analysis has resulted in confounding factors that impacted the results in some studies. These problems can be responsible for the different results in the current body of literature3 14 15 21–23 29 33–39 (table 2).
Evaluation of studies on distal to mid-shaft hypospadias
Taking into consideration these points, our study was performed with the inclusion of homogenous cohorts of toddlers aged 1–3 years with similar severity of the disease, using a single repair technique, and performing multivariable analysis.
A possible criticism of our study can be the follow-up period of 1 year, which might be considered short for hypospadias. However, studies have shown that a considerable number of complications (46%–100%) occur within the first year of TIPU and other types of distal repair.40–42 Another potential limitation of our study is the limited sample size that can result in the overfitting of the regression model. However, this was a result of the restricted number of target population groups. As another potential limitation, since our cohorts were consisting of children aged 1–3 years, the results might not be practical for other age groups and may require further investigations.
Conclusion
The current body of literature on the hypospadias prognostic factors has been plagued by lack of age-matched patients or control for meatal location, diversity in surgical techniques, the multiplicity of surgeons, or non-uniform distributions of study population ages. Our study proceeded to overcome these vulnerabilities by eliminating confounders, employing a single repair technique performed by a single surgeon, and enrolling an age-homogeneous study population of 1–3 years old with mid to distal hypospadias cases with no substantial chordee. Our study revealed that the location of urethral meatus was the only independent predictor of the development of complications. However, measures for modification of the risks related to the meatal location still need to be determined.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
IR.TBZMED.REC.1396.852
References
Footnotes
Contributors MRR contributed to conceptulization, data curation, formal analysis, writing – original draft, writing – review & editing and supervision. TAB contributed to data curation, writing – original draft and writing – review & editing. FKR contributed to resources, investigation, and writing – review & editing. SS contributed to writing – original draft and writing – review & editing. SMG contributed to writing – review & editing. FAF contributed to validation and writing – review & editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.