Article Text

Abstract
Introduction There are many techniques to treat congenital concealed penis (CP). Skin resurfacing is the most difficult step in severe cases. We aim to show medium-term results of coronal sulcus–based triangular ventral mucosal flap (CBVMF) as a treatment of prepubertal severe CP, a recently reported technique. We aim to determine whether results are durable and if the technique is associated with persistent mucosal redundancy or with a permanent unequal penile color pattern.
Methods CP cases reconstructed with CBVMF were reviewed. Preoperative complaints, degree of motivation of the child/parent to surgery, satisfaction of parent/child with results, and surgical complications were described.
Results Seven patients (6 months to 6 years old) were treated with CBVMP. Two patients showed megaprepuce and another was submitted to a limited postectomy 3 years before. One family was not fully satisfied (expected “bigger penis”), but acknowledged that the penis was now well exposed. No child talked about the problem preoperatively, but all of the boys were fully satisfied with the results of the surgery and verbalized this in the interviews. Flap edema resolved after 3 months in all but one patient. The flaps assumed the color of penile skin in the medium term.
Conclusions CBMVP results were satisfactory. Serious complications did not occur. Flap edema does not persist in the medium term, and redundancy was not a problem. The color of the flap tended to evolve into a pattern similar to the penile skin.
- surgery
- plastic
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant for the study are included in the manuscript.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Severe congenital concealed penis (CP) typically presents as an inconspicuous but easily palpable penis, ill-fixed on its basis, usually with a conical contour, as opposed to the normal cylindrical form. The disease is usually associated with dartos dysplasia and may relate to severe social and psychological problems from pre-pubertal age, due to penile appearance and to the inability to void standing.
Many surgical techniques have been described. They are based on extensive penile degloving, resection/releasing of abnormal dartos/abnormal skin fixations, and eventual division of the suspensory ligaments and/or pubic lipectomy, followed by resurfacing of the organ. This last step is frequently the most difficult because there may be insufficient skin to cover the now well-exposed penile shaft. Skin coverage under tension is doomed to failure: retraction of the stretched skin cause recurrence of CP. Scrotal flaps, preputial unfurling, and skin grafts are proposed to resolve paucity of local skin in the most severe cases, but these procedures may be associated with esthetic problems, such as growth of hair after puberty (scrotal flaps), dyschromia, and loss of skin elasticity (grafts).
Concerning penile esthetics, the dorsal surface should be prioritized over the ventral because the dorsal surface is usually the most exposed part of the penis to the patient, to other people in public toilets/locker rooms, and to sexual partners. A normal penile appearance is fundamental to guarantee a good self-image, especially during genital exposure and sexual encounters. Whenever scars, atypical skin, or esthetical defects are unavoidable, they should be diverted to the ventral surface of the penis.
Considering (1) the need to expand penile coverage beyond the native penile skin in severe cases of concealed penis, (2) the convenience of preserving normal genital skin as the dorsal penile surfacing material, and (3) the drawbacks of scrotal flaps, skin grafts, or preputial mucosa after preputial unfurling, Alexander et al recently described a coronal sulcus–based triangular ventral mucosal flap (CBVMF) as an additive to ventral penile resurfacing.1
Our aim in this paper is to review the immediate and medium-term results of seven prepubertal cases of congenital concealed penis treated with CBVMF. We hypothesized that CBVMF repair offers durable results after the treatment of severe cases of concealed penis, but we wanted to study whether the mucosal flap would show redundancy or would maintain a different color compared with native penile skin in the medium/long term.
Methods
Data collection
CP was defined as congenital unsatisfactory exposure of the penile shaft due to abnormal dartos and/or skin tethering, leading to an inconspicuous penis. All patients showed a normal urethra; CP cases showing urethral abnormalities, such as hypospadias or megalourethra, were excluded, as well as cases of scrotal webbing, operative cases without redundant preputial mucosa, and micropenis.
The data we collected were age of the patient on the date of the surgery and the last follow-up, preoperative complaints, degree of motivation of the parents for the surgery (Likert scale 1–5, 1 low to 5 high), satisfaction of the parent (Likert scale 1–5, 1 low to 5 high), whether the parent would consider the surgery for another child in need, and whether the parent would choose reoperation with the same technique if needed to get a better result. Surgeons were asked to evaluate postoperative results and to detail specific problems. All patients were called by telephone and asked to come to the hospital for a clinical evaluation, to take photographs of the penis, and to complete a questionnaire. Clinical evaluations were done by two experienced pediatric urologists (one of them did the operations). Subjective data were collected from the parent and the child whenever possible.
Each family signed an authorization form agreeing to participate in this research.
Surgical technique
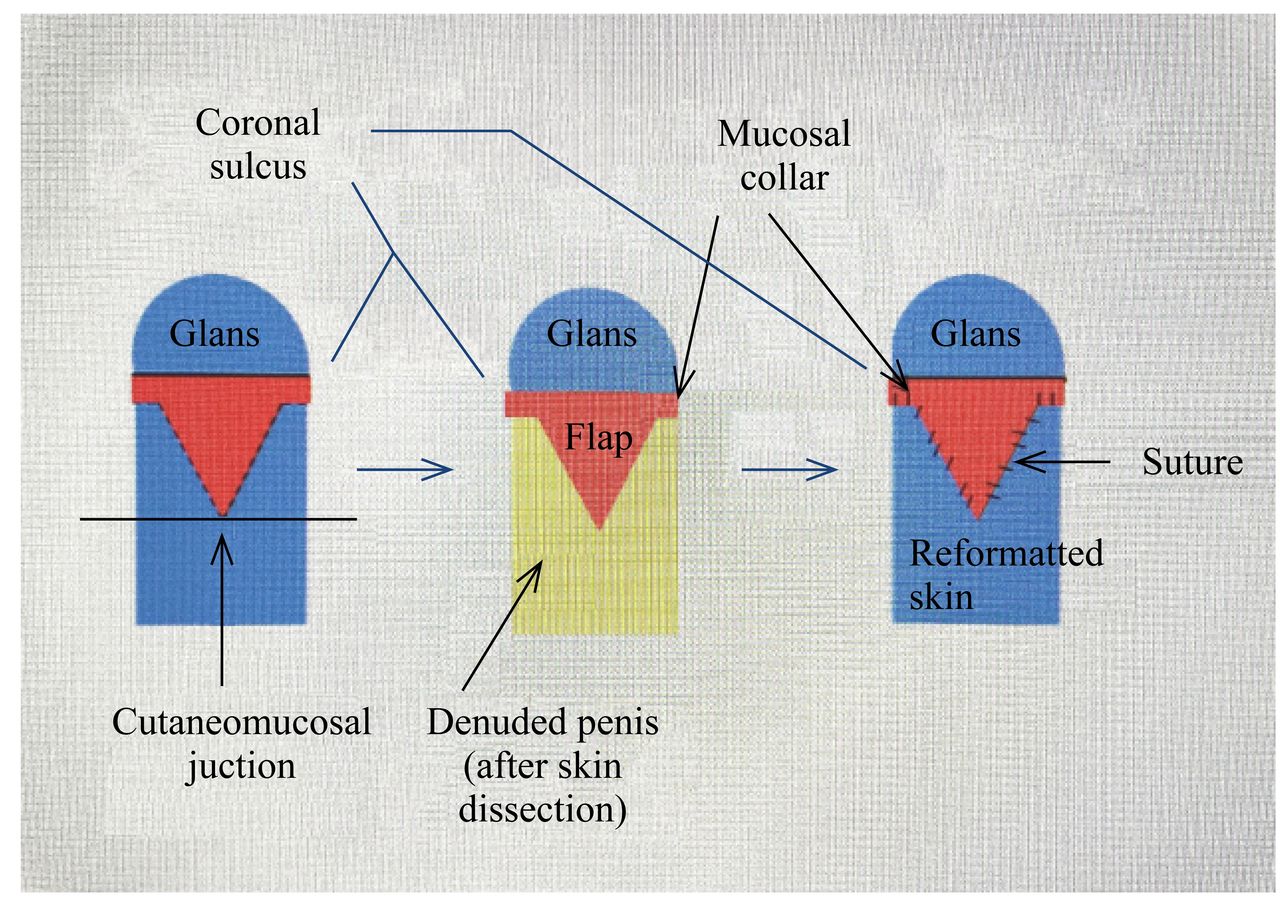
A CBVMF was planned in all primary cases of CP that showed redundant preputial mucosa. The flap was based on the central 1/3 of the ventral sulcus. A triangular flap with the apex in the phimotic ring/cutaneo-mucosal junction was designed and cut. The rest of the coronal sulcus circumference was treated with a circumcision incision 5 mm proximal to the sulcus. The surgery continued with penile degloving extending to the basis, division of abnormal skin fixations, dysplastic dartos, and suspensory ligaments (figure 1). During dissection, the urethra was evidenced and protected with catheterization. Patient 5 was also submitted to pubic lipectomy. The adventitia of the corpora was then fixed to the dermis of the proximal penile skin to reconstruct penoscrotal, penopubic, and lateral penile angles.
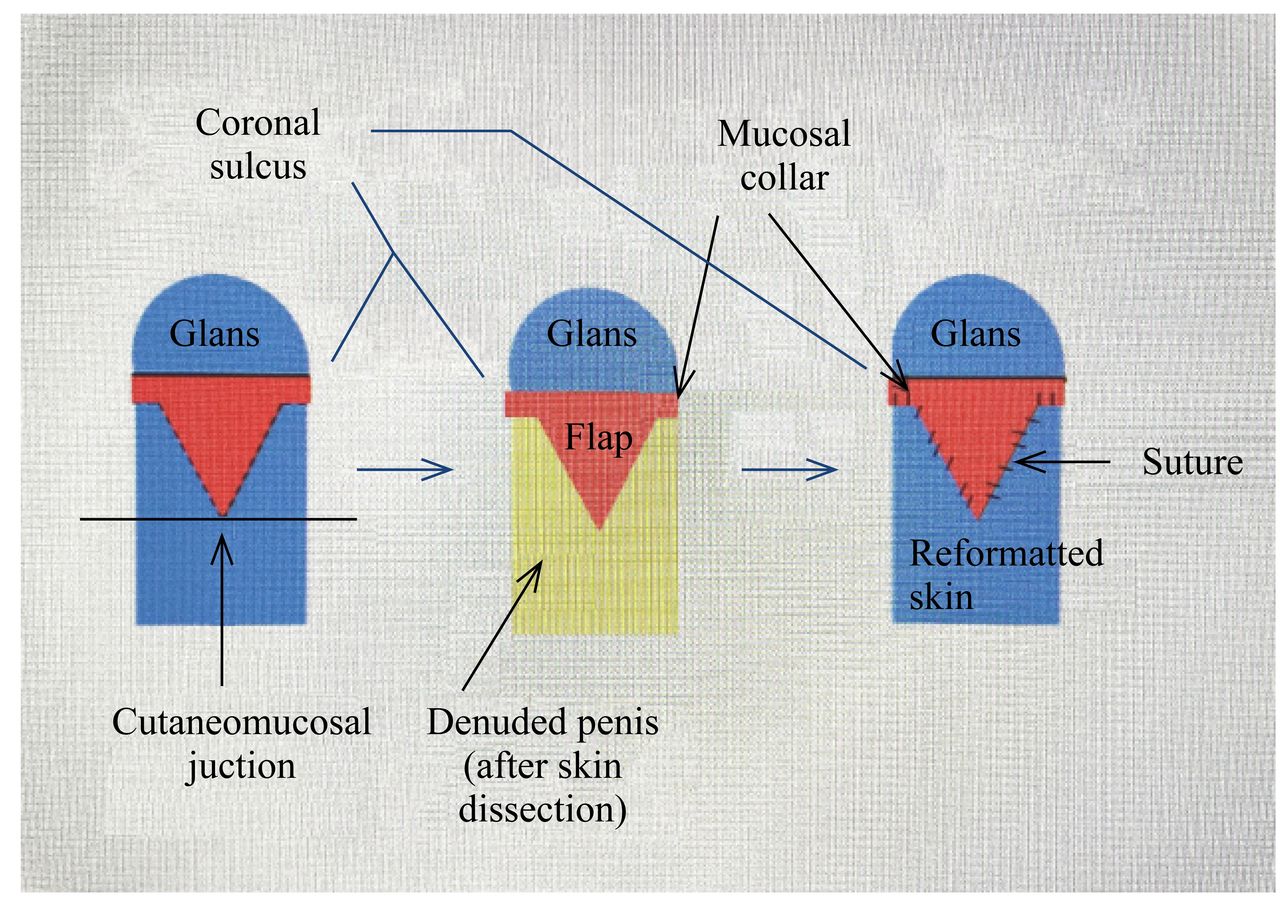
Diagram illustrating the main steps of the surgery (ventral face of the penis). Left: design of the flap (vascularized by the superior margin, based on the coronal sulcus mucosa). Center: dissected flap after penile degloving. Right: final result, showing the flap sutured to the reformatted skin (also shown in figure 3, immediate postoperative).
Dorsal penile resurfacing was the next step. Ventral/lateral penile skin was redistributed to the dorsum as needed. Ventral resurfacing was the final step. In patients without enough available penile native skin for complete ventral covering, CBVMF was trimmed and sutured to penile skin. The triangular ventral skin defect created by skin redistribution to the dorsum was covered with the mucosal flap, with care to maintain the flap stretched but not tense (figure 1).
Results
A CBVMP was used for reconstruction in seven patients (six primary cases and one reoperation after surgery for phimosis with a limited postectomy elsewhere) in our Pediatric Urology Clinics from 2012 to 2017. They are the object of this research.
This research presents medium-term results (6 months to 1 year) and long-term results (4 and 6 years) in 5 and 2 patients, respectively. Six of seven attended a clinical consultation and completed a non-standardized questionnaire. A single primary case refused to come to the hospital owing to social and financial constraints, but the mother was satisfied with the results of the surgery, as asserted in a telephone interview.
The results are summarized in tables 1 and 2. Ages at surgery varied from 3 to 11 years. Follow-up varied from 6 months to 6 years. Two patients showed megaprepuce (cases 1 and 3) and one was previously operated on to treat phimosis, 3 years before at another institution, with a limited postectomy that left mucosal redundancy (patient 5). No patient needed scrotal flaps. In all patients, the postoperative result showed a typical circumcised penis (morphologically normal exposed glans), a normal urethra, and voiding function postoperatively. Only one family was not fully satisfied (expected bigger penis), but acknowledged that the penis was now well exposed. No child expressed himself about the problem preoperatively, but all boys were satisfied with the results of the surgery and verbalized this in the postoperative interviews. The flaps took the color of penile skin in the long term, as shown in patients 1 and 3 (figures 2 and 3). The flaps tended to show some redundancy and it was essential to exactly adjust the flap to the skin defect exactly.

Patient 1, photographs showing clinical progress: preoperative status, post-operative short-term (3 months) and long-term (4 years). Please see that the penis remains well exposed and with a good cosmetic outcome.

{kind=link}
{kind=link}
{kind=link}
Patient 3, Concealed penistable 1 associated to megaprepuce, 6 years follow-up.
Patients and follow-up data
Patients and parents’ evaluations of the surgery
One patient (case 7) reported oversensitive glans and showed a small degree of flap edema (that did not bother the patient). In all of the other patients, the edema resolved after 3 months.
Discussion
Severe cases of CP cause serious problems to the patients (bad self-image, psychological problems, sexual avoidance, locker room panic) and difficulties to void (retention of urine in the prepuce leading to pseudo-incontinence, impossibility to hold the penis, and urine spraying). Balanitis and difficulties with hygiene are also common.
Congenital CP in children differs from acquired CP in adults. Most adult cases are caused by severe obesity, whereas congenital CP is associated with dartos dysplasia, non-fixation of the penile angles, and phimosis, despite obesity also being common. CP associated with megaprepuce is a rare variety, but we noticed that these patients responded very well to CBVMP (cases 1 and 3).
The most difficult problem in the reconstruction of severe CP usually is skin deficiency. Many techniques have been described, generally based on coverage of the cutaneous defect with unfurled preputial mucosa, local flaps (mostly scrotal flaps), and/or skin grafts obtained from glabrous skin sites.2 Unfortunately, long-term results are rarely reported. Many patients report dissatisfaction with their postoperative results.3 The esthetic results of unfurled prepuce may be unsatisfactory, as a significant area of the distal penis becomes covered by mucosa, frequently redundant and with a different color, including the dorsal surface.4 Scrotal flaps imply new scrotal scars and are associated with hair growth over the penis after puberty. Skin grafts may be inelastic, associated with abnormal sensation, and show unsatisfactory esthetics.
When the surgeon fixes pubic and scrotal penile angles and reconstructs the dorsal surface of the penis by redistributing the available penile skin in severe cases of CP, a ventral triangular skin defect with its basis on the coronal sulcus appears. The coverage of this ventral defect with a triangular preputial flap is the idea that led to the development of Alexander’s technique.1 The advantages are the use of local flaps without new scars on the scrotum or donor graft sites and the positioning of the flap limited to the ventral surface of the penis, preserving dorsal esthetics.
We observed a high degree of satisfaction among patients and parents, and there were no serious complications. However, acknowledging that psychological immaturity limits the consideration of children’s opinions concerning the need for genital surgery, penile problems are perceived by pre-pubertal boys. In our experience, most young boys do not speak out about their problems preoperatively, but they usually show their opinion and/or modify their social behavior postoperatively and are usually enthusiastic with good surgical results. Other authors attest that pre-pubertal patients show concerns about their genital appearance.5 6 Mucosal edema, especially ventral, is common after penile surgery and is also expected to affect the ventral flap; however, mucosal edema resolved in all patients in the medium term. The color of the flap tended to evolve into a pattern similar to the penile skin in the long term. Glans hypersensitivity, due to glans exposition, also resolved in the medium term, presumably after glans re-epithelialization.
To the best of our knowledge, no other publications have reported on the treatment of CP using Alexander’s technique and no long-term cases were described. We acknowledge the limitations of our research, the most important being the small number of patients. However, considering the exclusions (less severe cases, reoperative cases, cases associated with hypospadias), our cohort is highly selective. We also acknowledge the limitations of any statistics interpretation in such a small cohort, inferring that the usage of Likert scales should be interpreted only as a proxy of the parents’ opinions. Also, comments about sexual function are not possible owing to the age of the patients, but all children/parents report normal erections.
To conclude, CBVMF is an easy and efficacious technique to treat CP and is not limited to classical megaprepuce cases. The results are durable. Mucosal edema and skin dyschromia are not a problem in the medium term.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant for the study are included in the manuscript.
Ethics statements
Ethics approval
The ethic committee waived ethic approval of this study because it was a retrospective review of a recognised and conventional technique.
Footnotes
Contributors LJ contributed to conceptualization, methodology, formal analysis, and writing (original draft, review and editing). FAJ performed conceptualization, data curation, formal analysis, and writing (review and editing). FG was responsible for conceptualization, data curation, formal analysis, and writing (review and editing). TDR involved in conceptualization, data curation, formal analysis, and writing (review and editing). SD developed conceptualization, methodology, supervision, formal analysis, supervision and writing (review and editing).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.