Article Text

Statistics from Altmetric.com
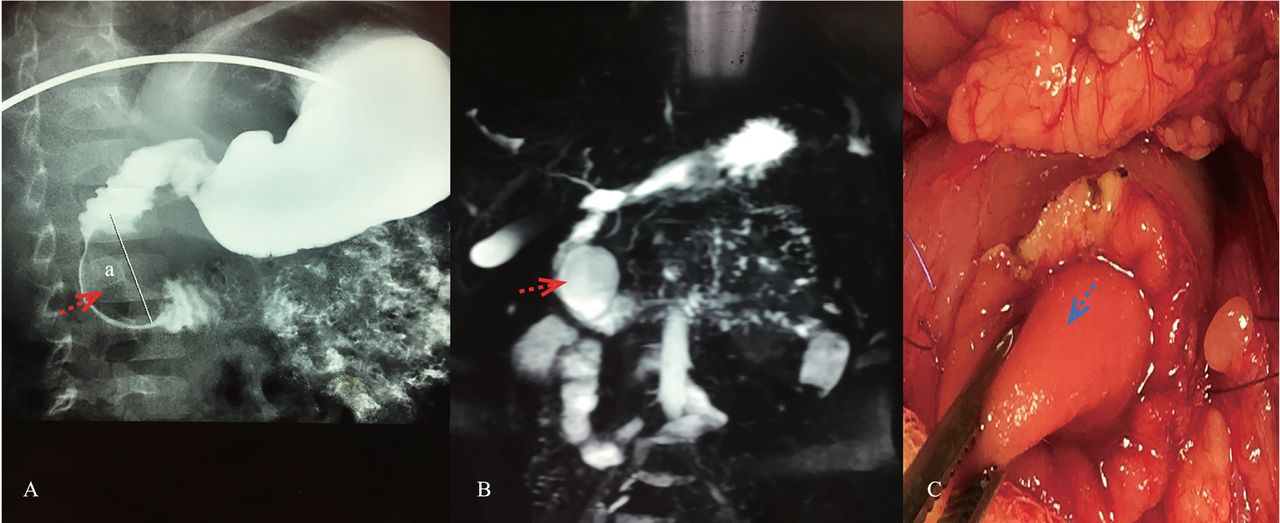
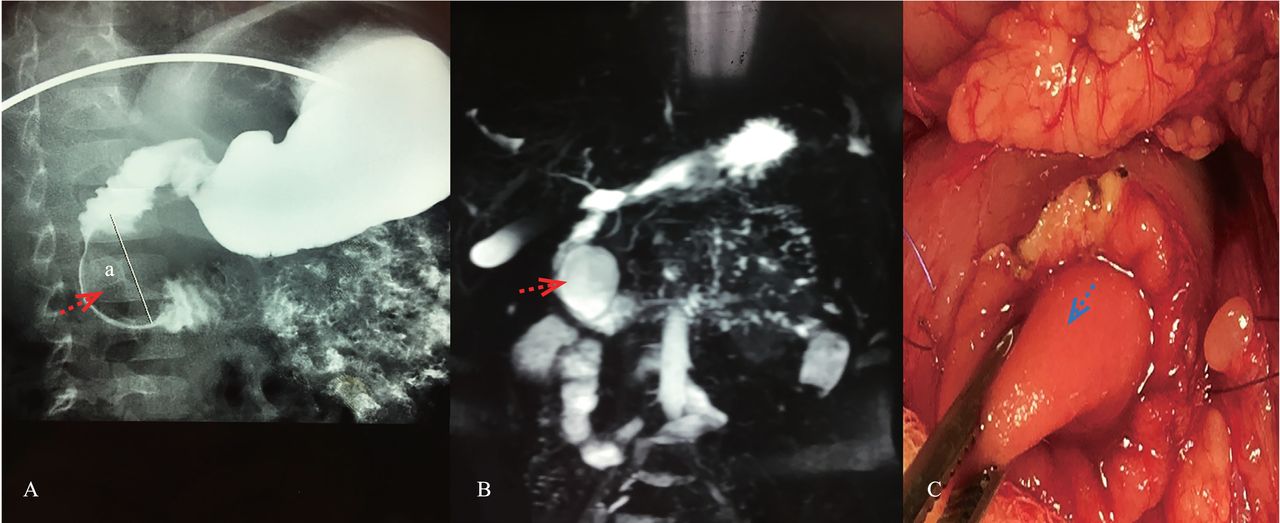
A 3-year-old female child with a history of intermittent abdominal pain and postprandial vomiting presented with fever, vomiting, and abdominal pain. The epigastrium was mildly sensitive on examination. Laboratory studies showed elevated leukocyte count (13 000/L), amylase (667 U/L), and lipase (2332 U/L). Abdominal CT showed pancreatitis with a cystic lesion repressing the pancreatic head. The radiographs were taken after drinking gastrointestinal contrast medium and showed ovoid filling defect on the medial aspect of the descending duodenum (figure 1A). Magnetic resonance cholangiopancreatography (MRCP) suggested the diagnosis of a duodenal duplication (DD) measuring 4 cm×3.2 cm repressing the Vater-ampulla (figure 1B). The patient operated with the resolution of symptoms. Surgery was decided to prevent recurrences of pancreatitis and complications of the cyst. During laparotomy, the cyst was palpated within the lumen of the duodenum. The second part of the duodenum was opened longitudinally and was found to share a common wall with the cyst (figure 1C). The Vater-ampulla was located on the duodenal cyst wall and drained the bile duct. Stripping mucosal lining after excising the resectable portion of the cyst was performed. The postoperative course was uneventful, and the girl was discharged on the fourth postoperative day. Histopathology confirmed the diagnosis.
{kind=link}
Radiologic and peroperative aspects of the duodenal duplication. (A) Gastrointestinal tract contrast radiography showed oval-shaped lacunar image located in the second duodenum (arrow pointed). “a” meaned the distance was 38 mm. (B) Magnetic resonance cholangiopancreatography showed duodenal duplication measuring 4 cm×3.2 cm in contact of the Vater-ampulla and biliary duct (arrow pointed). (C) Perioperative view of the duodenal duplication and the opened duodenum (arrow pointed).
DDs account for 5% to 9.6% of all gastrointestinal duplications.1 A recent meta-analysis identified fewer than 50 published cases.2 Most of the cases did not communicate with the intestinal lumen.3 Symptoms are non-specific, such as abdominal pain, hemorrhage, cyst infection, or intussusception.1–4 DD is a rare cause of acute pancreatitis in childhood. Upper gastrointestinal contrast radiographs and MRCP are useful for an accurate diagnosis. They may demonstrate communication with pancreatic and/or bile duct. Complete surgical resection is the treatment choice.2 3 However, in front of close proximity with the main pancreatic duct and the common bile-duct like our case, marsupialization may be chosen. Although DD is considered a benign entity, a few cases developed complications and malignancies. Therefore, a long-term follow-up would be necessary mainly for patients who underwent marsupialization.
Footnotes
Contributors AS and MBM contributed to original draft writing, review and editing. ZH, FW, GL, and MR provided critical review of the manuscript. All authors approved the draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Ethics approval This study has been approved by the hospital ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.