Article Text

Abstract
Aspiration and evaluation of gastric residuals are commonly performed interventions before each feeding in intensive care units, especially in very low birthweight infants. However, there is no sufficient evidence about the necessity of routine gastric residual aspiration. In this study, we aimed to investigate the time to full enteral intake and the incidence of necrotizing enterocolitis (NEC) in preterm infants in the period with gastric residual aspiration performed before each feeding, and those in the period without gastric residual aspiration.
Methods Preterm infants with a gestational week ≤33 were included in the study. The group with gastric residual control before each feeding consisted of 169 infants, and the group without routine gastric residual aspiration included 122 infants.
Results The mean gestational week was 30.37±2.58 and 29.31±3.37 in the group with gastric residual control and in the group without routine residual control, respectively (p<0.05). Birth weight, male gender, and mode of delivery were similar between both groups. The time to full enteral intake was shorter in the group without routine residual control (p<0.05). Total durations of parenteral nutrition, ≥grade 2 NEC, weight at discharge and duration of hospitalization were similar between the groups. Duration of invasive mechanical ventilator support was shorter in the group without routine residual control.
Conclusion Avoidance of routine gastric residual aspiration in preterm infants shortens the time to full enteral intake without increasing the incidence of NEC.
- neonatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Aspiration and evaluation of gastric residuals are commonly performed interventions before each feeding in intensive care units, especially in very low birthweight infants.
There is no sufficient evidence about the necessity of routine gastric residual aspiration.
What are the new findings?
Avoidance of routine gastric residual aspiration in preterm infants shortens the time to full enteral intake without increasing the incidence of necrotizing enterocolitis.
The number of studies reporting that routine gastric residual control should not be performed in the absence of other clinical findings, and recommending to increase enteral intake is increasing.
How might it impact on clinical practice in the foreseeable future?
The time to full enteral intake will be decreased in preterm infants.
INTRODUCTION
Aspiration and evaluation of gastric residual aspiration before each feeding are commonly performed procedures in intensive care unit especially in very low birthweight infants feeding with orogastric tube. Despite limited studies published on this issue, increased gastric residual volume or discoloration was considered as an early finding of nutritional intolerance or necrotizing enterocolitis (NEC).1 2 It has been reported that gastric residual volume is influenced by lying position of the patient, diameter of feeding tube, gastric localization of the tube, warmth and viscosity of the food intake.3–5 Increase in gastric residual volume and change in its character due to delays in gastric emptying and decreased intestinal motor activity because of gastrointestinal system immaturity in premature infant may be physiological.6 7 Therefore, routine gastric residual control in preterm infants before each feeding may be unnecessary. In recent years, the number of studies reporting unnecessity of routine gastric residual control before each feeding is increasing.8–10 In this study, we investigated clinical features especially the time to full enteral intake and the incidence of NEC in preterm infants in the period with gastric residual aspiration performed before each feeding, and those in the period without gastric residual aspiration in our tertiary neonatal intensive care unit.
Methods
As in many other units, gastric residual control has been also performed in our tertiary neonatal intensive care unit in preterm infants feeding with orogastric tube until 1 September 2017. We introduced a new application in our unit from 1 September 2017 and began to avoid routine gastric residual control if there were no other clinical findings (vomiting, abdominal distension, abdominal tenderness, abdominal discoloration, not looking well and bloody stool) accompanying NEC. Patients with a gestational week ≤33, hospitalized during 1 year between 1 September 2017 and 31 August 2018 were defined as the ‘group without residual control’ and the patients hospitalized during 1 year before 1 September 2017 were defined as the ‘group with residual control’. A total of 291 patients were enrolled in the study. Residual control group consisted of 169 infants, and non-residual control group included 122 infants. Patients with congenital anomalies, diagnosis of syndrome, gastrointestinal system anomalies, and patients in whom enteral nutrition could not be initiated within postnatal 2 days were excluded from the study. All infants were fed with 6F orogastric feeding tube. In the application of unit, all infants were laid and fed in supine position. Increasing nutrition, discontinuing nutrition, time to discontinue parenteral nutrition, taking the patient to orogastric drainage, laboratory and radiologic assessment of the patient were decided in accordance with written protocol of the unit (figure 1).
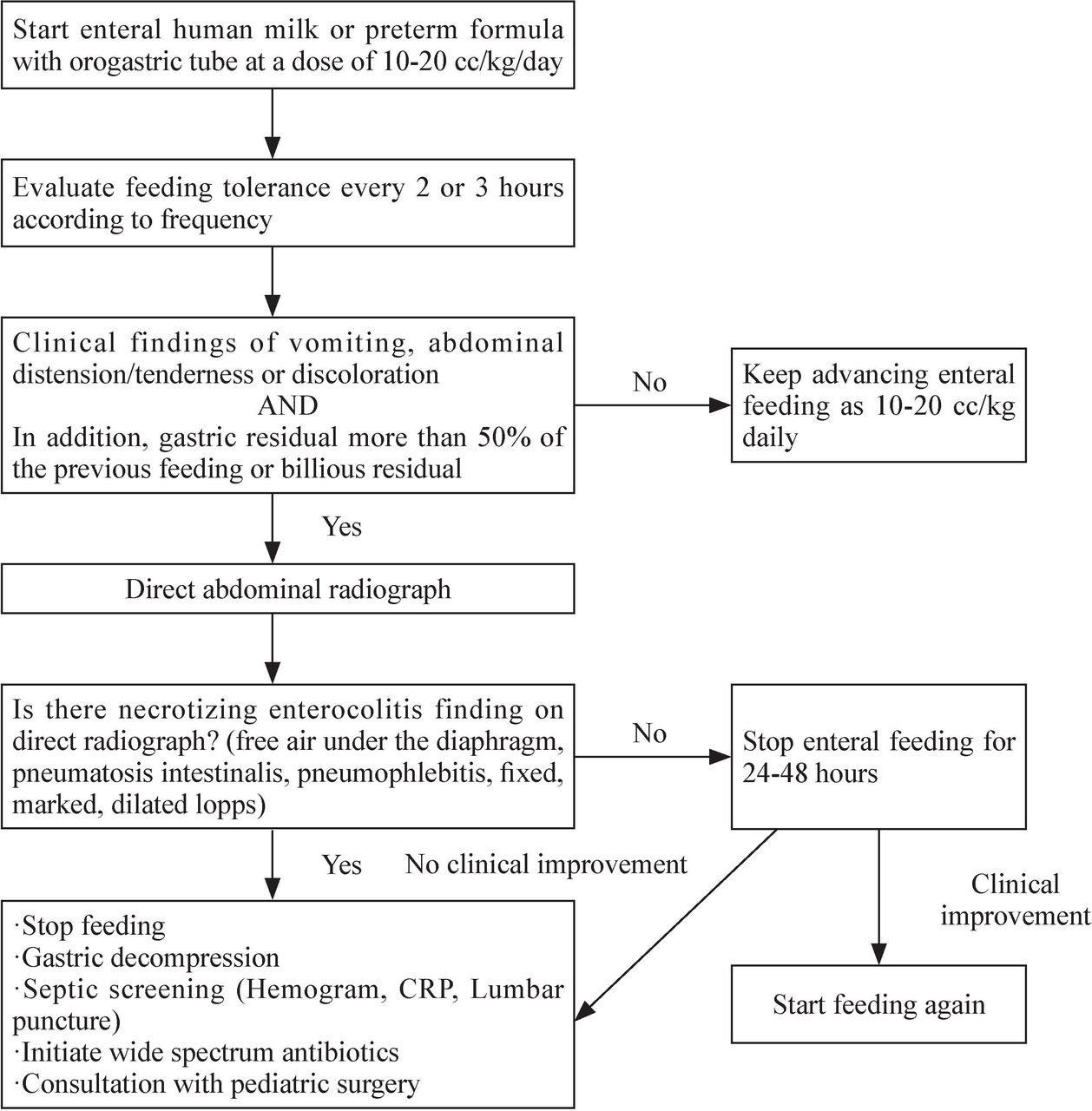
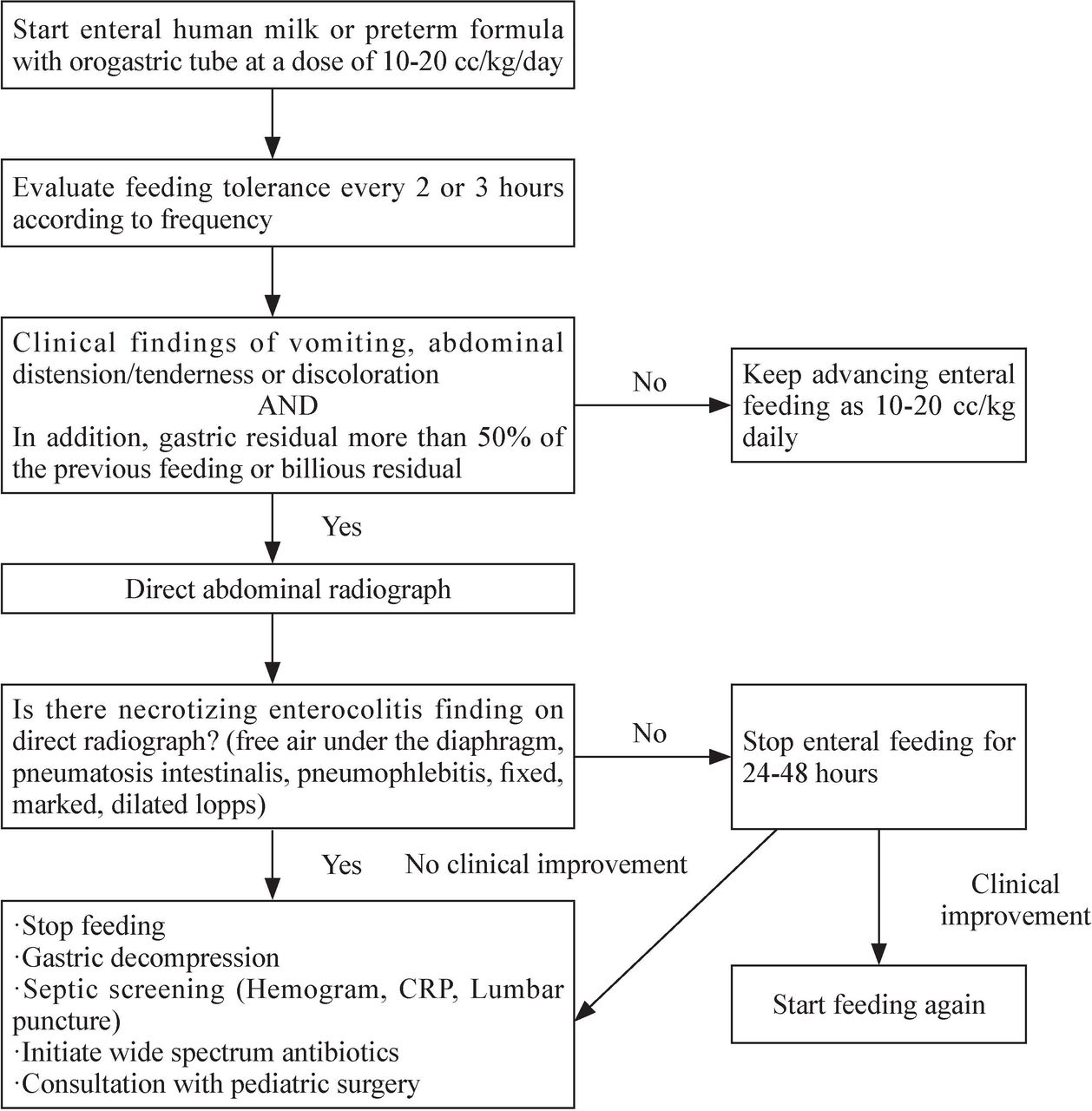{kind=link}
Enteral feeding algorithm of preterm infants, which is used in our neonatal intensive care unit. CRP, C-reactive protein.
Data of the patients were obtained from epicrisis reports and patient files in the hospital archive.
Statistical analysis
Statistical analyses were performed using SPSS software (V.16, SPSS). To test the normal distribution of variables, visual (histogram and probability graphics) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk tests) were used. Clinical characteristics of infants were described by mean values and standard deviation (SD), or rates and percentage. Univariate statistical analysis was performed using the Student’s t-test for continuous variables with normal distribution, Mann-Whitney U test for continuous data with no normal distribution, and Fisher’s exact test or χ2 test for categorical variables. A p value <0.05 was considered statistically significant.
RESULTS
The group with gastric residual control consisted of 169 infants, and the group without routine residual control included 122 infants. The mean gestational week was 30.37±2.58 and 29.31±3.37 in the group with gastric residual control and in the group without routine residual control, respectively (p<0.05). Birth weight, male gender and mode of delivery were similar between both groups (table 1). Both groups were similar in terms of the type of nutrition (only mother’s milk, only formula, mix of mother’s milk and formula). The time to full enteral intake was shorter in the group without routine residual control (p<0.05). Total duration of parenteral nutrition, ≥grade 2 NEC, weight at discharge and duration of hospitalization were similar between the groups (p>0.05). In addition, late sepsis diagnosis, patent ductus arteriosus and intraventricular hemorrhage were also similar between both groups. Duration of intubation was shorter, while duration of mechanical ventilation with nasal continuous positive airway pressure (nCPAP) was longer in the group without routine control (table 2).
Comparison of the baseline characteristics of the groups
Comparison of the outcome measures in the groups
Discussion
It was known that enteral feeding initiated immediately after birth affects maturation of the gastrointestinal system, decreased nutritional intolerance and provided a better neurodevelopmental outcome, especially in very low birthweight preterm infants.11–13 However, nutritional intolerance is more commonly seen as gastrointestinal system is immature in preterm infants compared with term infants. Gastric residual control is a commonly performed intervention to evaluate the presence of nutritional intolerance in most neonatal intensive care units.14 There is no consensus on how much gastric residual volume should be to define nutritional intolerance, but a gastric residual volume higher than 50% of the amount of previous nutrition has been more adopted.14–16 However, variable gastric residual volume without other clinical findings may be physiological in premature infants. Shulman et al reported that evaluation of gastric residual volume was not an appropriate indicator for transition to full enteral intake in infants feeding with gavage.17 Again Mihatsch et al reported that green colored gastric residuals were a poor indicator of nutritional intolerance, and it should not pose an obstacle for increasing enteral feeding intake in the absence of other clinical findings or symptoms.14 The time to full enteral intake was reported to be short when gastric residual volume was not controlled.18 19 In their study including critical patients’ follow-up with mechanical ventilation, Poulard et al reported that avoiding gastric residual control was associated with increased enteral intake without increasing the risk for nutritional intolerance, vomiting and ventilator-related pneumonia.20 Riskin et al reported that total parenteral feeding was discontinued 1 day earlier, and transition to enteral intake was made 1 day earlier in patients in the group without gastric residual control.9 In their randomized controlled study, Torrazza et al reported that premature infants without routine gastric residual control began to enteral intake 6 days earlier, and the need for central venous catheter ended 6 days earlier in these infants.8 In our study, the mean duration to full enteral intake was 10.08 days in the group with routine gastric residual control, and 8.10 days in the group without routine residual control, while the difference was statistically significant. No statistically significant difference was found between the groups in terms of the duration of total parenteral feeding.
The incidence of NEC, which progresses with morbidity and mortality especially in very low-birth-weight preterm infants is between 7% and 11%.21–23 A gastric residual volume higher than normal can be considered as an early finding of NEC.15 Cobb et al reported that a residual gastric volume of 4.5 mL or 40% of the previous feeding was an early indicator of NEC compared with a residual volume of 2 mL or 14% of the previous feeding.24 Similarly, in their case control study, Bertino et al reported that increased gastric residual volume was associated with NEC.15 Torrazza et al compared the group with and without gastric residual control, and reported that the incidence of NEC did not increase in the group without routine gastric residual control.8 In their study including preterm infants with a gestational week ≤34, Riskin et al found the incidence of ≥stage 2 NEC as 1.7% in the group without routine gastric residual control, and 3.3% in the group with gastric residual control. At the same study, earlier transition to full enteral intake was reported in the group without routine gastric residual control.9 In our study, the incidence of NEC was found as 1.8% in the group with routine gastric control, and 3.3% in the group without routine gastric control, but the difference was not statistically significant. The mean duration to full enteral intake was 10.08 days in the group with routine gastric residual control, and 8.10 days in the group without routine residual control, and the difference was statistically significant. Duration of total parenteral feeding was similar between the two groups (p>0.05). Li et al reported that routine gastric residual control was not necessary, and a residual volume higher than 50% of the previous feeding should be further evaluated only in the presence of clinical findings of nutritional intolerance and NEC (vomiting, visible bowel loops, increased abdominal circumference, abdominal distension, and abdominal tenderness).25 In our unit, we do not perform gastric residual control before each feeding if there is no other finding of accompanying NEC from 1 September 2017.
In their study, Riskin et al reported a longer duration of non-invasive mechanical ventilation in the group with routine gastric residual control.9 Whereas in our study the duration of invasive mechanical ventilation was shorter and the duration of non-invasive mechanical ventilation was longer in the group with routine gastric residual control.
Limitations of this study include being conducted in a single center and designed as a before and after study. In addition, the lack of sample size calculation and power analysis for NEC outcome was another limitation.
In conclusion, today routine gastric residual control before each feeding is still performed in most neonatal intensive care units. The number of studies reporting that routine gastric residual control should not be performed in the absence of other clinical findings, and recommending to increase enteral intake is increasing. Avoidance of routine gastric residual control before each feeding shortens the time to full enteral intake without increasing the incidence of NEC and duration of parenteral feeding. Further well-designed multicenter randomized controlled studies especially including larger series of very low birthweight infants are needed to further enlighten this issue.
References
Footnotes
Contributors SA designed, executed the study, and interpreted the results. MT analyzed the data, prepared the methodology, and performed literature searching.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Adiyaman University Ethics Committee (No: 2017/8-13). Written consent was received from families of the infants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Data is included in the main text.