Article Text

Abstract
Background Acute kidney injury (AKI) occurs in 42%–64% of the neonatal patients experiencing cardiac surgery, contributing to postoperative morbidity and mortality. Current diagnostic criteria, which are mainly based on serum creatinine and hourly urine output, are not sufficiently sensitive and precise to diagnose neonatal AKI promptly. The purpose of this review is to screen the recent literature, to summarize the novel and cost-effective biomarkers and approaches for neonatal AKI after cardiac surgery (CS-AKI), and to provide a possible research direction for future work.
Data sources We searched PubMed for articles published before November 2019 with pertinent terms. Sixty-seven articles were found and screened. After excluding 48 records, 19 articles were enrolled for final analysis.
Results Nineteen articles were enrolled, and 18 possible urinary biomarkers were identified and evaluated for their ability to diagnose CS-AKI. Urinary neutrophil gelatinase-associated lipocalin (uNGAL), serum cystatin C (sCys), urinary human kidney injury molecule-1 (uKIM-1), urinary liver fatty acid-binding protein (uL-FABP) and interleukin-18 (uIL-18) were the most frequently described as the early predictors of neonatal CS-AKI.
Conclusions Neonates are vulnerable to CS-AKI. UNGAL, sCys, uL-FABP, uKIM-1 and uIL-18 are potential biomarkers for early prediction of neonatal CS-AKI. Renal regional oxygen saturation by near-infrared spectroscopy is a non-invasive approach for early identification of neonatal AKI. Further work should focus on exploring a sensitive and specific combined diagnostic model that includes novel biomarkers and other complementary methods.
- cardiac surgery
- neonatology
- intensive care
- nephrology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Acute kidney injury (AKI), also known as acute kidney failure, covers a wide spectrum of clinical states, from subtle increase of serum creatinine (sCr) to serious injury that requires renal replacement.1 2 AKI is a common complication of patients after cardiac surgery both in adults and in children, and is recognized as one of the most important factors contributing to postoperative morbidity and mortality.3–5
The mechanism of acute kidney injury after cardiac surgery (CS-AKI) is not well understood and can involve multiple factors. Hemodynamic fluctuation, inflammatory/immune factors, coagulation and neurohumoral regulation disorder might play essential roles in the development of CS-AKI. Neonates are vulnerable to CS-AKI. Neonatal renal physiological features and several comorbidities and associated conditions have proved to be high-risk factors for neonatal CS-AKI (box 1). The reported incidence of AKI following pediatric cardiac surgery was 30%–50%, whereas in the neonatal population the incidence was 42%–64%, depending on the definition of AKI and the enrolled cardiac lesions (table 1). The occurrence of CS-AKI has been proven to be associated with short-term and long-term outcomes in neonates. Neonates with CS-AKI require longer duration in mechanical ventilation, intensive care unit stay and hospitalization. The mortality rate of neonates receiving dialysis after cardiac surgeries is 6.4 times higher than that of neonates without AKI. Furthermore, a 2-year follow-up study indicates that the infants surviving from Acute Kidney Injury Network stage 2 and 3 in their neonatal period have lower Z score for height.4 6 Establishing an ‘alarm system’ to identify patients at high risk for AKI might facilitate the initiation of prompt intervention and might improve the outcomes. The purpose of this review is to summarize the recent literature and to describe the novel and cost-effective biomarkers and tools for early diagnosis of neonatal CS-AKI.
The mechanisms of neonatal CS-AKI
Pathophysiology:
Hemodynamic fluctuation
Inflammation/immunity
Others
Risk factors:
CHD, congenital heart disease; CPB, cardiopulmonary bypass; CS-AKI, acute kidney injury after cardiac surgery; DHCA, deep hypothermia cardiac arrest; ECMO, extracorporeal membrane oxygenation; ELBW, extremely low birth weight (birth weight <1000 g); LCOS, low cardiac output syndrome; ROS, reactive oxygen species; VLBW, very low birth weight (birth weight <1500 g).
Incidence of CS-AKI in neonates
DIAGNOSIS OF CS-AKI IN NEONATAL PATIENTS
Several definitions for AKI have been launched since 2004, including the Risk, Injury, Failure, Loss, and End-Stage Kidney Disease (RIFLE), Acute Kidney Injury Network (AKIN), and the Kidney Disease: Improving Global Outcomes (KDIGO) classifications.7–10 The disparities and similarities among these definitions are listed in table 2. In the case of patients with cardiac procedures, severe AKI stages are related to adverse outcome and higher mortality; however, the debate on the standard criteria for CS-AKI remains unsettled and depends on the patient population enrolled and the validated version of each criterion (such as adding a diagnostic period to AKIN and KDIGO systems).11 12 Generally, RIFLE is much more sensitive in identifying the risk-stage patients, and the AKIN and KDIGO may be more specific in diagnosing AKI, particularly in recognizing stage 3 patients. Nevertheless, all three classifications are based on the change of sCr directly and indirectly. The main challenges of diagnosing neonatal AKI are focused on the following items:
The promptness of sCr: sCr obviously will not change until 25%–50% of renal function is lost, and the effect of fluid dilution may conceal the real change in sCr. Therefore, the rise in sCr in neonatal patients always delays until 36–48 hours after surgery. Patients in an early phase of AKI might not be discerned and would miss timely intervention.
Some neonates present non-oliguric AKI, especially preterm neonates due to higher proportion of body water.13 Thus, urine output (UO) less than 0.5 mL/kg/hour is not sufficient, and some researchers refuse to take UO as a reliable indicator of CS-AKI.
The number of nephrons and the tubular maturity are closely related to gestational age.11 12 14 The renal blood flow improves gradually within the initial several weeks after birth. However, glomerular filtration rate (GFR) will not be steady until 2 years of age.15 Accordingly, gestational age, birth weight and postnatal age all have a potential impact on the susceptibility of neonates to AKI.
Definition and classification of neonatal acute kidney injury
Early prediction of CS-AKI in neonatal patients
Regarding the limitations of sCr and UO in early recognition of CS-AKI in neonatal patients, tremendous research has been performed to explore possible serum and urine biomarkers and other non-invasive methods for discriminating patients at high risk for AKI.
Serum and urine biomarkers predicting neonatal CS-AKI
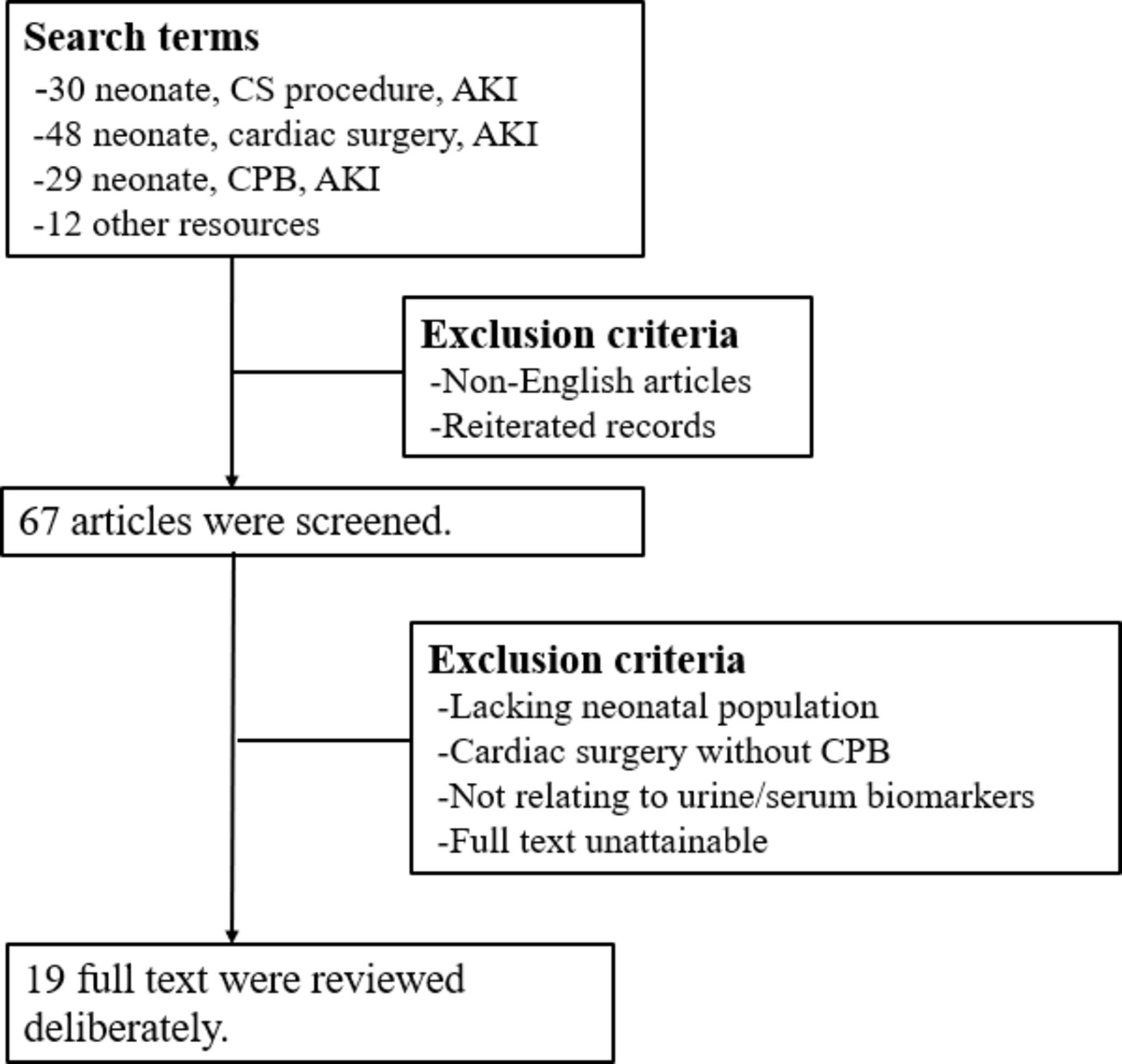
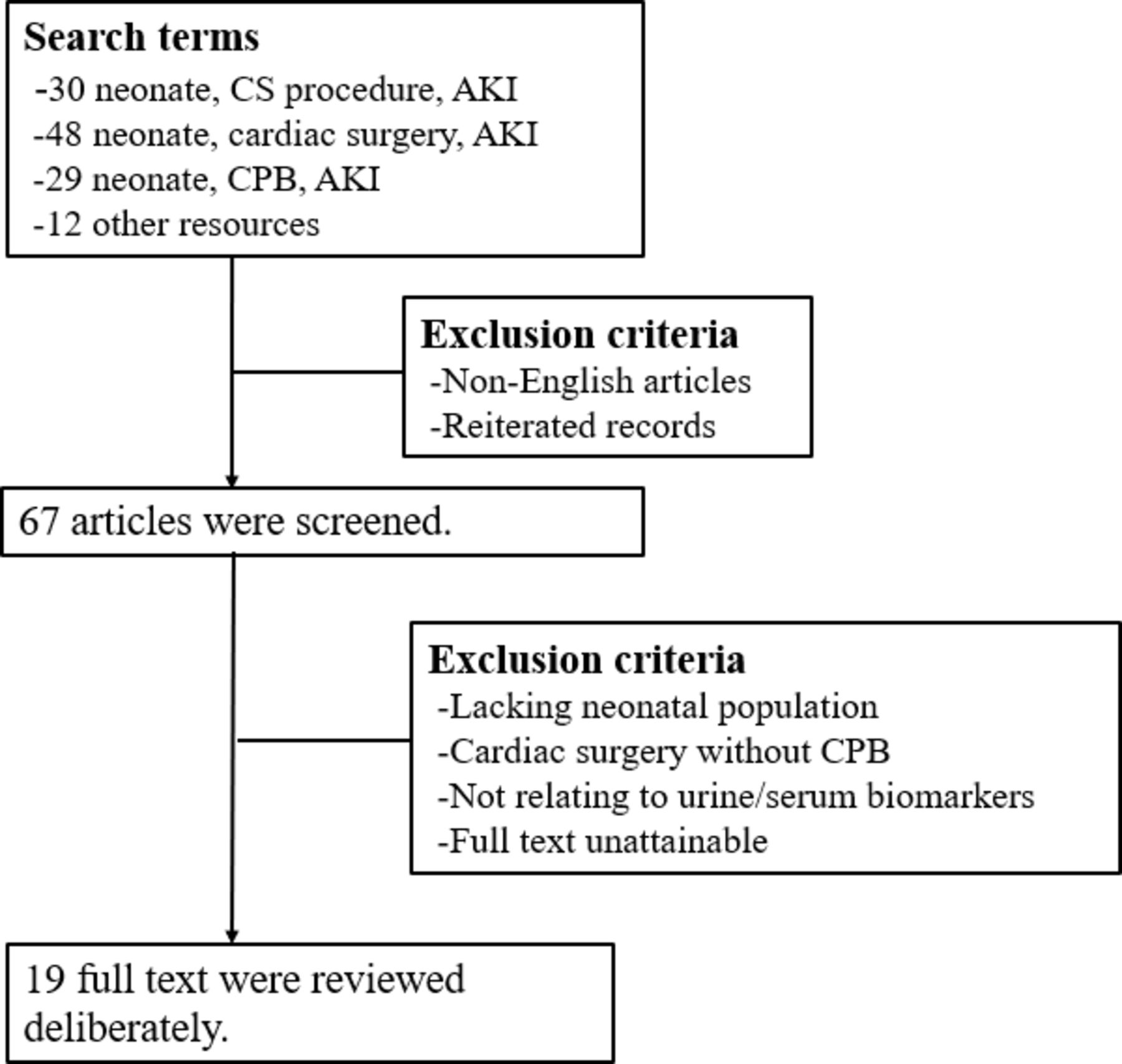
We searched PubMed with terms ‘neonate, cardiac surgery, acute kidney injury’, ‘neonate, cardiac surgical procedure, acute kidney injury’ and ‘neonate, cardiopulmonary bypass, acute kidney injury’ separately. Clinical trial, clinical study, controlled clinical trial, multicenter study, observational study and randomized controlled trial published before November 2019 were considered. A total of 67 articles were screened. After excluding 48 of these records, 19 articles were analyzed. The methodology is explicated in figure 1.
{kind=link}
Literature retrieval process. AKI, acute kidney injury; CPB, cardiopulmonary bypass; CS, cardiac surgical procedure.
It is notable that, in the case of neonates, the application of urinary biomarkers for early prediction or for adding diagnostic value to sCr is prevalent. Urine samples were applied in a total of 15 of the 19 studies we collected. The plausible explanations are that urine-oriented biomarkers can reflect both the structural damage and the functional injury of the kidney directly and that urinary samples can be obtained non-invasively from Foley catheter after cardiac surgery. The utilities of novel biomarkers in neonates are illustrated in table 3.
Literature review of novel biomarkers predicting CS-AKI in neonates
Proximal tubular cell biomarkers
Neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1) and liver fatty acid-binding protein (L-FABP) are secreted by the proximal tubular epithelial cells. Increases in concentration indicate tubular injury.
Elevating serum and urinary NGAL levels have been widely identified in patients with AKI with multiple etiologies. The relationship between NGAL and CS-AKI in neonates was also evaluated recently. In four studies including neonates, the rise in urinary NGAL (uNGAL) occurs as early as about 2 hours after surgery and shows good diagnostic ability for CS-AKI regardless of AKI definitions, even normalized by creatinine, and can be one of the independent risk factors for adverse clinical outcomes.16–22 Other studies also indicate that the value of uNGAL within 12 hours after surgery is a strong predictor of CS-AKI, and it is significantly associated with poor outcomes.21 23 24 A study including 30 neonatal patients concludes that, besides postoperative serum NGAL (sNGAL), preoperative sNGAL is also a potential indicator of CS-AKI.25 But the conclusions are not always on the same page. A study published in 2018 with 59 neonates and infants reveals that both uNGAL and sNGAL are not indicators of CS-AKI. But in the cases experiencing longer cardiopulmonary bypass (CPB) time (≥75 min), uNGAL increases significantly as early as 2 hours after surgery.26
KIM-1, a type 1 transmembrance protein, could not be detected in urine normally, but increases promptly after proximal tubular epithelial cells injury, boosting epithelial repair and phagocytosis. In a study with patients younger than 1 year old (including neonates), urinary KIM-1 at 6 hours after CPB has predictive power for AKI, with an AUC of 0.66.27 L-FABP, which is involved in fatty acid metabolism, expresses highly in ischemic insult and is a sensitive predictor of kidney diseases. Urinary L-FABP (uL-FABP) increases at 2, 6 and 24 hours after surgery and proves to be a strong indicator of CS-AKI in neonatal and infants, and the AUC for uL-FABP is 0.89, 0.75 and 0.87, respectively.23
Biomarkers of GFR
Cystatin C, a low-molecular-weight protein, is filtered freely by the glomerulus. Compared with creatinine, the serum cystatin C (sCys C) level would not be influenced by maternal level, gestational age, sex and muscle mass. Taking these theoretical properties into consideration, Cys C sounds an ideal marker of renal function in neonates in different clinical situations.28–30
In the studies of neonates undergoing cardiac surgery, significant upregulation of sCys C is found at 2 and 8 hours following CPB and has been proven to be an independent predictor of AKI.31 32 Likewise, elevating urinary cystatin C is also detected at a very early period after surgery (0, 2 hours) in patients with poor outcomes.24
Inflammatory biomarkers
Systemic inflammatory response is a major cause of CS-AKI. Research studies have indicated that the traditional inflammatory mediators, including interleukins (ILs), interferon-gamma, tumor necrosis factor-alpha, granulocyte colony-stimulating factor, granulocyte-macrophage colony-stimulating factor, C reactive protein and so on, do upregulate early after cardiac surgery. Theoretically, these phenomena are more likely to be a reaction to CPB than to the renal insult per se.33 34 IL-18, a proinflammatory cytokine, is activated and released into urine after ischemic insult of proximal tubules. However, the role of urinary IL-18 (uIL-18) in predicting AKI is still controversial. Zheng et al35 reveal that in patients developing AKI uIL-18 has the best predictive ability at 4 hours after surgery, with an AUC of 0.835. In contrast, Morgan et al33 do not find a significant difference in IL-18 between AKI and non-AKI patients.
Other biomarkers
In addition to the mainstream biomarkers mentioned, several other biomarkers are reported as potential predictors of CS-AKI. Tissue inhibitor metalloproteinase type 2 (TIMP-2) and insulin-like growth factor-binding protein type 7 (IGFBP-7) are two molecules provoking G1 cell cycle arrest, playing key roles in the development of and recovery from AKI.36 Meersch et al37 identified that urinary TIMP-2*IGFBP-7 concentration demonstrates a highly early predictive value for AKI (4 hours after surgery) in infants and children. Likewise, a recent study including infants and neonates reports that urinary TIMP-2*IGFBP-7 concentration at 12 hours after CPB strongly indicates the occurrence of AKI, with an AUC of 0.71.24
Electrolytic and metabolic disorders are also involved in the kidney insult after cardiac surgery, and persistent hyperphosphatemia may prognose severe renal impairments. Burra et al’s38 study found that serum phosphorus level increased significantly at 24 hours postoperatively in patients with AKI and could be another alternative predictor of CS-AKI. The rise in the preoperative and postoperative levels of fibroblast growth factor 23, a hormone which regulates renal phosphate reabsorption, has also been proven to be associated with severe AKI.39
Furthermore, thrombocytopenia has been identified as a risk factor for CS-AKI, and the degree of the nadir platelet count has a strong relationship with the severity of AKI.40 First postoperative urine albumin to creatinine ratio is also an available marker predicting stage 2 and 3 AKI in patients younger than 2 years old.41 Serum gelsolin is significantly decreased at 6 hours following CPB in patients with AKI and has been proven to be an excellent predictor of CS-AKI in neonates and young infants.42
In general, NGAL, cystatin C, L-FABP, KIM-1 and IL-18 were the most frequently detected for early prediction of CS-AKI. Table 4 illustrates the common time period for each biomarker, all of which occur much earlier than the rise in sCr. However, it is unavoidable that these findings have some limitations. First, the majority of studies were conducted in single-center manners with non-uniform AKI criteria and with limited sample sizes. Second, the findings in this review are obtained from studies including both neonatal and pediatric patients and lack systematic evaluation, particularly in the case of neonates. Third, although the novel biomarkers express rapidly after surgery, the discrepancies in sensitivity and specificity in different clinical settings are huge. Further work aiming to develop a joint application of traditional and novel biomarkers is needed in order to improve diagnostic accuracy.
Common time period of biomarkers predicting neonatal CS-AKI
Renal near-infrared spectroscopy predicting neonatal CS-AKI
Near-infrared spectroscopy (NIRS), a non-invasive, continuous and real-time monitor device, is used to detect regional oxygen saturation (rSO2), namely the oxygen content within the local tissue. This new technology is based on the different absorptions of near-infrared wavelengths by oxygenated and deoxygenated hemoglobin, known as the Beer-Lambert principle. The sensor could be placed on the forehead, the surface of the abdomen, or the left or right side of the spine at the T10–L2 level to detect the cerebral, abdominal and kidney rSO2, respectively. The neonatal cerebral rSO2 was recorded by Jobsis for the first time in 1977.43 In 1991, NIRS was used as a non-invasive tool for evaluating the effect of hypothermic CPB and total circulatory arrest on pediatric cerebral metabolism.44 Since then, tremendous research has been implemented to assess the influence of ischemic insult on the neurological, renal and other organic functions by NIRS in neonates.
A study including 40 neonates and young infants indicates that patients with renal rSO2 <50% more than 2 hours within the first 24 hours after surgery are more susceptible to AKI. In addition, patients with permanently low renal rSO2 need longer mechanical ventilation and inotropic support.24 45 Ruf et al46 continuously monitored the renal rSO2 intraoperatively and 24–48 hours postoperatively and found that intraoperative persistently low renal oximetry (<65%) or significant decrease of oximetry (>25%) was related to the occurrence of AKI and poor outcomes and that the diagnostic value of NIRS might surpass NGAL and cystatin C. These findings indicate that NIRS can be another promising non-invasive bedside monitor for the development of CS-AKI in neonates. Despite the inspiring results, NIRS still has several imperative shortcomings. First, the normal and pathological baseline for renal rSO2 is still lacking, and the variance between individuals is significant. Second, the value of renal rSO2 is easily influenced by the position, exogenous light, and cyanotic and non-cyanotic congenital heart diseases. Therefore, exploring a sensitive and specific combined diagnostic model consisting of NIRS and other chemical markers is inevitable in future work.
CONCLUSION
Neonatal patients are vulnerable to CS-AKI. Identifying the patients at high risk for CS-AKI facilitates timely intervention and improves outcome. UNGAL, serum cystatin C, uL-FABP, uKIM-1 and uIL-18 are the potential biomarkers for early prediction of CS-AKI in neonates. Continuous monitoring of renal rSO2 by NIRS could be a cost-effective complement in the early diagnosis of neonatal AKI. Further work should focus on exploring a sensitive and specific combined diagnostic model that includes novel biomarkers and non-invasive tools.
Acknowledgments
We sincerely appreciate the Key Laboratory for Diagnosis and Therapy of Neonatal Diseases, the Children’s Hospital of Zhejiang University School of Medicine for serving as the scientific advisers.
References
Footnotes
Contributors SSS collected the data and drafted the manuscript. FJJ analyzed the data and assisted in revising the manuscript. SQ designed the study and supervised the drafting of the manuscript. All authors had read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Not required for this review paper.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no data sets generated and/or analyzed for this study. No data, models or codes were generated in this review paper.